9 & 10- dental ceramic materials
1/23
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
24 Terms
Advantages of ceramics
Excellent aesthetics- good translucent and texture
Biocompatible- non toxic, well tolerated by tissues, minimal allergy compared to metals
Colour stability- resistant to staining and discolouration overtime
High compressive strength- good for load bearing areas
Chemical stability- resistant to corrosion and oral fluids
Low thermal conductivity- protects pulp form temp changes
5 Disadvantages of ceramics
Brittle- low tensile stress- prone to fracture under stress
Technique sensitive
Wears (abrasive to) opposing teeth
Difficult repair
Costly
How can dental ceramics be classified?
Type
Use- denture teeth, metal-ceramics, veneers, inlays, crowns, anterior bridges
Processing method- sintering, casting or machining
Substructure material- cast metal, staged metal, glass ceramic, CAD-CAM, sintered core
Compared to metal ceramics, what are the advantages of all ceramic restorations?(7)
Increased translucency
Improved fluorescence
Greater contribution of color from the underlying tooth structure
Inertness
Biocompatibility
Resistance to corrosion
Low temperature / electrical conductivity
Why do all new types of ceramic have a lower incidence of fracture?(3)
All ceramic restos made of stronger materials + better fabrication
Can be etched and bonded to underlying tooth with new dentin adhesives
Greater reduction means thicker and stronger resto
How can ceramics be classified based on composition?
Glass-based Ceramics
Feldspathic porcelain
Leucite-reinforced ceramics
Lithium disilicate
Glass-infiltrated Ceramics
In-Ceram (alumina-based)
Polycrystalline Ceramics
Zirconia
Alumina
Indications of ceramics?
Anterior Restorations- veneers, crowns
Posterior Crowns- esp with high-strength ceramics like zirconia
Inlays and Onlays- Conservative restorations with good esthetics
Fixed Partial Dentures (Bridges)- Short-span bridges using high-strength ceramics
Implant-supported Prostheses- Zirconia frameworks for implants
Full-mouth Rehabilitation- need esthetics and durability
Contraindications for ceramics?
Parafunctional Habits- Bruxism increases fracture risk
Limited Tooth Structure- Insufficient support may lead to failure
Poor Oral Hygiene- Risk of secondary caries and restoration failure
Deep Subgingival Margins- Difficult bonding and isolation
Heavy Occlusal Forces- May lead to fracture, especially in weaker ceramics
Types of full ceramic crown and their pros vs cons?
Feldspathic- very aesthetic but weaker
Lithium disilicate- good balance of aesthetics and strength
Zirconia- very strong, for posteriors
What are the advantages vs disadvantages of shoulder margin on ceramics and how can you reduce the fracture index?
Very aesthetic, risk of fracture during cementation, use limited to vestibular area of anterior teeth
Need special shoulder, costly
Do perfect impression and tooth prep, avoid using in posteriors, not for bridges, use cemented adhesive
Advantages of ceramic veneers
Colour- stable better control and natural
Bond strength- strong bond between etched veneer to enamel
Periodontal health- glazed surface- less plaque acc
Resistant to abrasion
Strong
Resistant to fluid adsorption
What is the umbrella effect and how can we avoid it?
The lip acts as a umbrella- can see raised margin and dark interdental papilla due to shadow
In veneres- light reflected so avoids it
Disadvantages of ceramic veneers
Time consuming
Repair difficult once luted to enamel
Technique sensitive- indirect
Colour- can’t modify once luted
Need tooth prep
Fragile
Indications of ceramic veneers?
Discoloration- Due to fluorosis, tetracycline staining
Enamel defects- types of enamel hypoplasias and hypocalcification
Diastema- can close
Malpositioned teeth- The esthetic illusion of straight teeth can be developed
Malocclusion- The configuration of lingual surfaces of anterior teeth can be changed to develop incisal guidance or centric holding in malocclusions or periodontally compromised teeth.
Poor restorations
Aging- mask color changes
Wear patterns
Contraindications of ceramic veneers
Need enough available enamel- if tooth mainly dentin and cementum use crowns
Inability to etch enamel- temp teeth or excess fluoride
Oral habits- bruxism or biting foreign objects
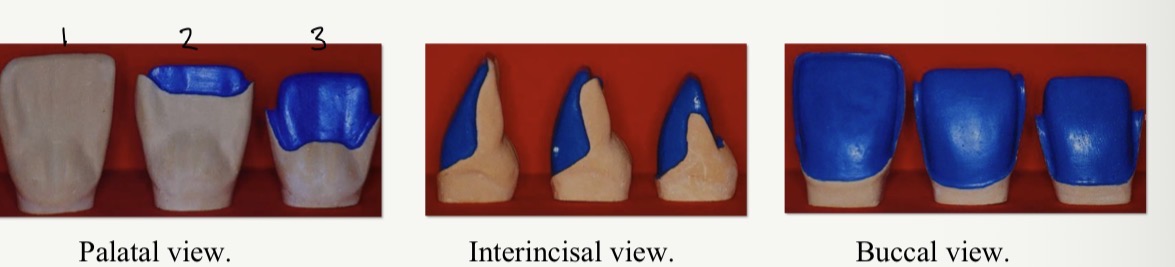
3 types of veneer prep
Not exceed incisal edge (contact lens)
Exceeds incisal edge (classic type)
Widely exceeds incisal edge (three quarter type)
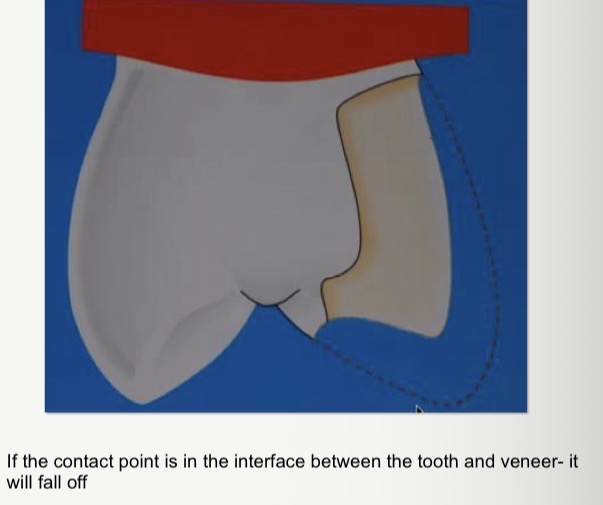
What should you consider when doing veneer prep on premolars?
Avoid positioning the contact point of the antagonist directly over the junction between the ceramic veneer and the natural tooth
Advantages of incisal reduction compared to contact lens type?
Reduces angular fractures: thicker ceramic
Greater aesthetics
Allows to change the shape of the teeth
Facilitates changes in dental position
Facilitates the manipulation and cementation of the veneers.
Allows the margin to be placed outside the occlusal impact area (main point)

What’s the name of the bur and when do we use it?
Veneer depth cutting bur for vestibular preparation
Types of retraction cord- disadvantage?
Normal black cord fine thickness, second yellow cord– has to be removed when putting second light silicone in the sulcus
Need someone to help you remove the cord while you pour the silicone
Have to use at least 1 retraction cord
What’s the main problem caused by mixing clay based material with an astringent ?
retraction may not be sufficient and uniform around the tooth- problems with impression material tearing or difficulties reading the margins in the lab
Non cord method- clay based material mixed with astringent (paste) and injected into sulcus
What other non cord method can be used for surgical retraction and their disadvantage?
Laser, trimming bur, electrocautery or radio frequency device- leaves troughs around tooth
May need firmer tissue ablation for hemostasis
But cause trauma to gingiva- may not return to og state
How to bond veneers/prep veneers for bond?
Remove provisional and clean tooth
Try in
Clean and dry veneer- 9.6% hydrofluoric acid 2 mins
Orthophosphoric acid 20secs to clean
Apply silane agent inside veneer for 1 min and dry
Place matrix in interproximal
How do you prep en ale and dentin for a veneer?
Etch 37% orthophosphoric acid 30secs in enamel, 2-secs dentin - wash + dry
Apply dentin adhesive- lightly dry
Place cement on veneer and place
Polymerise each surface for 1 min
Pass floss interdentalkg