Chapter 5: Neuroplasticity and Recovery
1/4
Earn XP
Description and Tags
Lecture 4
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
5 Terms
course of recovery
recovery = progress in functioning compared with the state immediately following occurrence of injury
Most brain damage recovery happens right after the accident, in the first 3-6 months.
Recovery curve flattens, farther you go, less recovery you get
two types of recovery: spontaneous and experience dependent
spontaneous recovery
Spontaneous recovery (injury induced changes): changes in the brain occur in response to the injury at the neuronal level (12-14 weeks), due to neuronal recovery:
Synaptogenesis: creation of new synaptic connections
Structural and functional recovery of penumbra (brain tissue adjacent to site of stroke, a.k.a. the peri-infarct area, which has reduced blood flow and potential damage to the neurons' dendrites): improvement in blood flow (reperfusion), rapid restoration of blood flow
Diffuse and redundant connectivity: if one area is affected, other parts will become more active; activating other areas within a network (more even hemispheric distribution/bilateral activation in lesioned brains, lateralisation in healthy brains) - could be maladaptive
Cortical reorganisation/remapping: new structural and functional connections between cortical areas take over; sometimes peri-infarct areas/more distant areas with similar function take over for damaged area, then function represents itself differently in the cortex - remapping.
As aphasia patients progress in speech, more activation in penumbra and homologous areas in the unaffected hemisphere.
Increased activation in undamaged hemisphere results from insufficient inhibition by damaged hemisphere.
So we should promote plasticity: non-invasive brain stimulation (NIBS) to stimulate/inhibit specific areas - only short-term effects, limited effect on long-term, daily life (not yet In clinical practice or guidelines of stroke, Parkinson, but rTMS used for depression)
experience-dependent recovery
Experience-dependent recovery (dependent learning): promoting plasticity through learning
Taxi drivers: large neurological changes in areas associated with spatial memory (compared to bus drivers);
neurons that fire together wire together,
use it or lose it: brain area is not stimulated -> further decline, not stimuating potential reorganisation.
specificity is key
information that is salient/refers to self is retained better,
repetition/intensity/time matters
Age matters (more neuroplasticity, sometimes better, outdated Kennard principle); sometimes worse to have a brain injury while still young, when older you are helped by habits.
Cognitive deficits only become visible when more complex cognitive skills are needed -> growing into deficits (memory problems at 5 years old, not noticeable because less demands and more help, as you grow the problem is noticed since life becomes more complex).
picture: ICF model (International Classification of Functioning, Disability and Health)
Function recovery (treating the source of the problem, neural plasticity) vs. functional recovery (behavioural compensation; making the process work despite the problem, compensating).
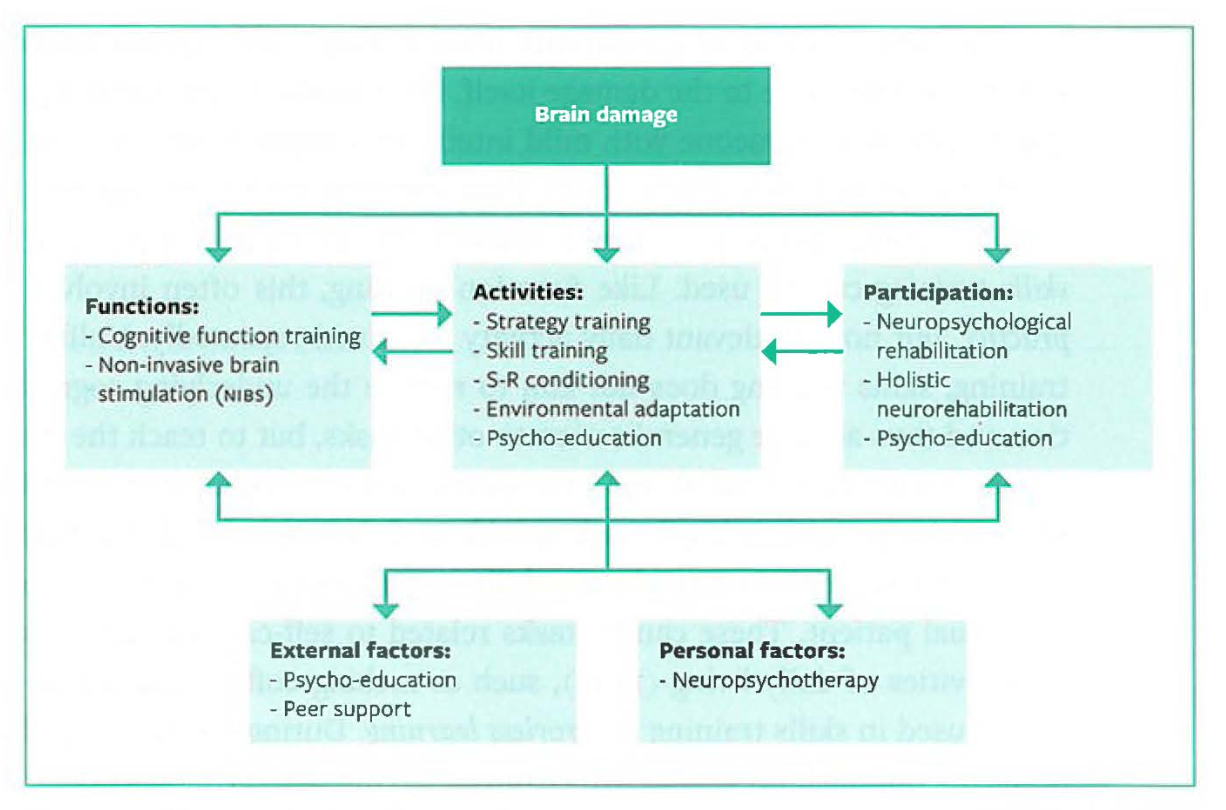
types of cognitive training
Restorative approach: Function training: recovery of cognitive functions occurs through repeated exercise
Effectiveness has not been demonstrated, almost never generalises to real life. Doesn’t really work, near and far transfer:
Near transfer to task strongly related to trained task/content
Far transfer to different task, context, domain.
Generalisation of learning behaviour - applying what is learned to everyday life. Challenge for people with brain injury, as learning depends on intact cognitive functions.
Compensatory approach: Cognitive training: learning strategies to compensate for cognitive impairments. (focuses on activities and participation)
Environmental adaptation: e.g. signs around to help people find their way, notes about where things are
Stimulus-response conditioning (S-R conditioning): limited routine triggered by a stimulus; e.g. laying clothes out to make someone get dressed
Skill training: training a specific skill at task level through repeated exercise. Not aimed at improving underlying cognitive function!, use of "errorless learning" (no guessing or trial and error, always guidance), highly task specific, not aimed at generalisation.
Strategy training: training skills that apply in multiple tasks/situations; e.g. "stop, think, act"
neuropsychological rehabilitation
Neuropsychological treatment has a shorter tradition than diagnostics, most of the research is focused on cognitive impairments
Neuropsychological rehab = focuses on cognitive disorders but also on emotional and behavioural disorders resulting from brain injury.