multifocal designs and fitting selection
1/37
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
38 Terms
what are the reasons px want multifocal contact lenses
due to old age
patient that are used to wearing CL before presbyopia and still wish to do so
will have difficulties - using phones, reading messages, watch, menus, reading labels etc - don’t want to wear reading glasses so would want MF CLs
what is a multi focal lens by definition and who are they mainly used for/by
MF - aspheric lens that has multiple powers
fitted for presbyopes and also for myopia control in children
state and explain the 3 main designs of multi focal contact lenses (and what is the most common one)
most commonly Soft MF - aspheric - and mostly centre near — although centre distance are made
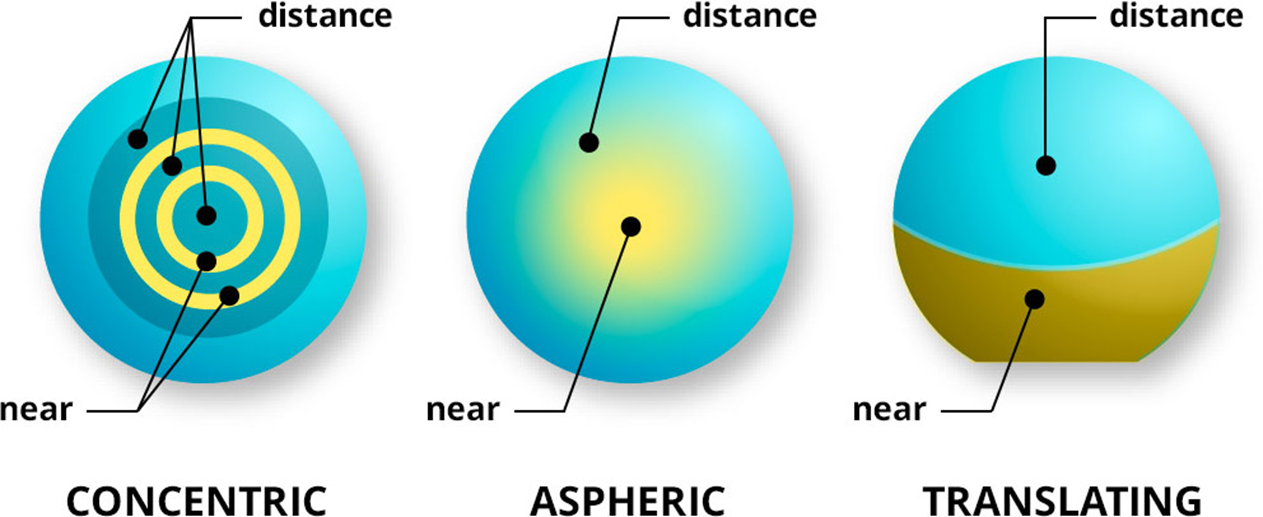
concentric - bullseye pattern - distance and near alternating - strictly speaking a bifocal with 2 distinct powers in each zone
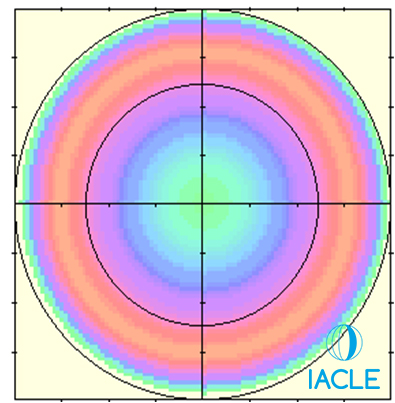
aspheric - near power in centre and distance in periphery (periphery holds no power in terms of rx as outside of visual axis) - Aspheric designs are truly multifocal to the extent that they display a gradual transition in lens power between distance and near - no fixed powers
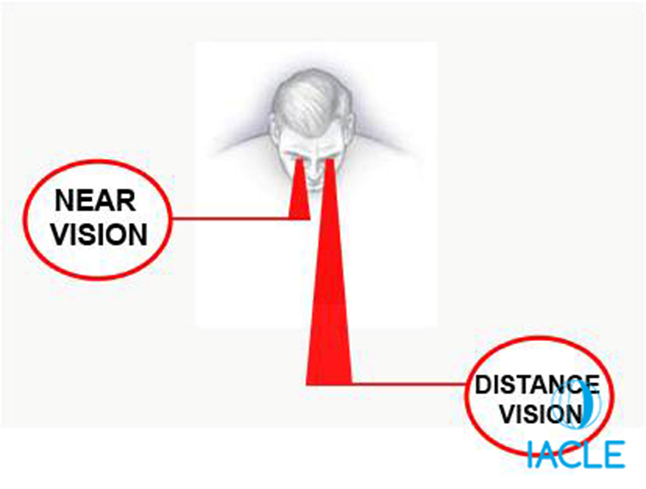
translating - mainly in GP lens designs however still used in MFs - used by moving the reading position into the pupil with downward gaze - when px looks down the near area pushes into their line of sight - strictly speaking this is also bifocal
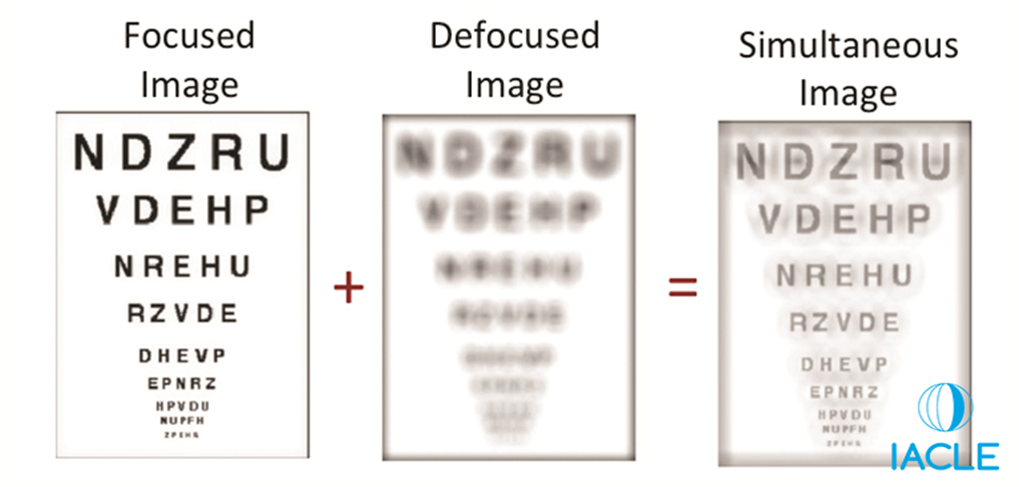
how do multi focal lenses acc work (5)
by simultaneous vision
occurs in each eye - brain suppresses the image that is not required
px who do not have ability to suppress will struggle with these lenses
utilizes information based on where px is looking
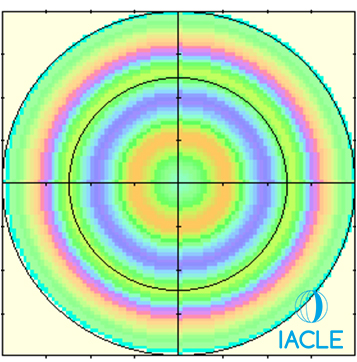
have to make px aware that there vision may be compromised as shown in image below
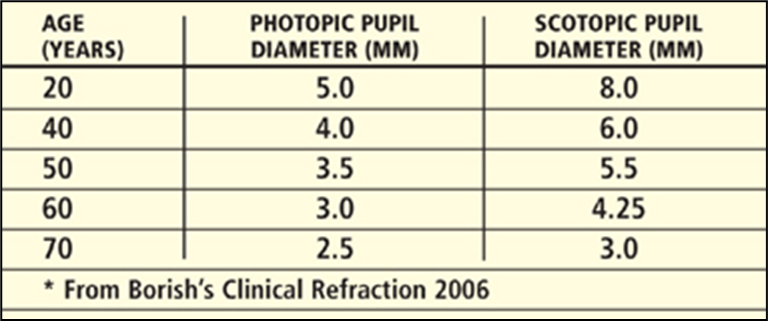
how does the power of lenses alter from centre to periphery in centre distance lenses in terms of illumination and pupil size
◦Low illumination favours near vision - pupils dilate in low illumination - reading power in periphery - able to access near better
◦High illumination favours distance vision - pupil constricts - using mainly central part of lens which contains distance power - peripheral near zones less exposed - distance vision clearer
how does the power of lenses alter from centre to periphery in centre near lenses in terms of illumination and pupil size
◦Low illumination favours distance vision - pupil dilates - exposes more peripheral distance zones - more distance light enters eye - distance vision improves
◦High illumination favours near vision - pupil constricts - using mainly central near zone - more near light enters eye - near vision improves
what are the age related factors we look at when fitting patients with MF lenses (6)
eye lids
conjunctival drag/conjunctiva
tear film
iris and pupil
visual function
cornea
describe the age related changes of the eye lids (4)
•Decrease in muscle tone and elasticity - loose lids
•Non-optimal apposition of lid to globe
•Ptosis
•Ectropion
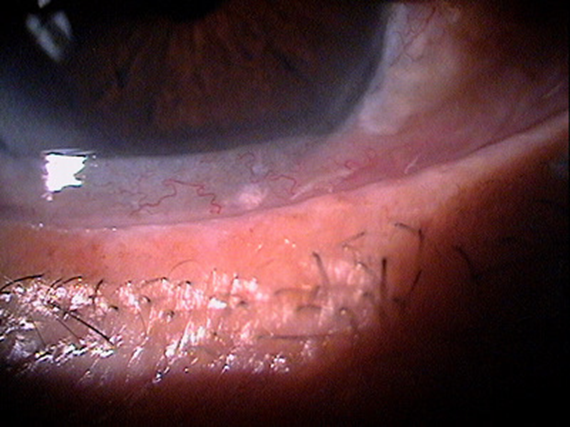
describe the age related changes of the conjunctival drag/conjunctiva (3)
Conjunctivochalasis is a condition characterised by redundant or loose conjunctiva between the globe and eyelid
conjunctiva tends to collect - CL may irritate this
Pingueculae & pterygia
describe the age related changes of the tear film (3)
•Progressive ↓ in tear production due to ↓ in goblet cells & mass of lacrimal gland
•Dry eye – 4 times more prone - CL can exacerbate this
•Drying can ↑ deposition on CLs leading to allergic responses, ↓ vision, irritation & frequent replacement of lenses
describe the age related changes of the iris and pupil (3)
◦Pupil size gradually ↓ with age (senile miosis)
◦Entrance pupil sets limit for translation and centration of contact lens - px with small pupils limited success with MF - as power may fall out of the pupillary zone/if lens decenters
◦May compromise vision in low lighting conditions
describe the age related changes of visual function (2)
↓ in VA - particularly in low contrast and low luminance
Glare sensitivity - decreased retinal luminance
describe the age related changes of the cornea (3)
•Fragility
• Reduced sensitivity
• Endothelial changes
in terms of a case history what do we need to consider when fitting for MF CLs (7)
◦Motivation for use
◦Tasks that are important
◦Previous contact lens wear
◦Previous multifocal spectacle wear
◦Expectations
◦Normal cl related questions
◦#use the word compromise - as not every task will be optimal due to the simultaneous vision of these lenses
describe what we need to consider for tasks that are important for a px when completing a case history (5)
◦Occupation - professional liability / negligence issues - doctors/pilots - px need to be aware of this
◦Primary Need - distance, intermediate or near
◦Functioning Environment - direction of gaze, duration of fixation - mainly straight ahead/left/right
◦Secondary Need - social, part-time other occupations
tell patient we won’t be able to help with ALL tasks - need to find out what is a priority and what they intend to wear these lenses for
explain why we need to assess ocular dominance (3)
Dominant Eye corrected for Distance: (DD)
Non-Dominant Eye corrected for Near: (NN)
This is the crux for choosing the trial lenses for your patient
describe the different tests to assess ocular dominance (3)
Blur suppression
Distant spotlight viewed with optimal DISTANCE Rx worn in front of both eyes
Transfer a +lens of ADD power between the two eyes
Ask in which eye is it easier to ignore the ‘starburst’ = that is the NON-Dominant eye/the eye that can accept the most plus/has the least amount of blur with plus
+2.00DS blur test
Similar concept but letter chart employed
If NO preference then select eye with best acuity as the Dominant Eye
Sighting dominance
ask px to look at a target and form a diamond shape around it
then close each eye one a time and ask px with which eye open does the target stay the most in the shape
this eye is the dominant eye

state the different types of fitting options of CLs (4)
mono vision - one eye sees distance and one eye sees near - NOT MF CLs - will be spherical or toric CLs
modified monovision - mixture between spherical/toric and MF - MF that are adapted to provide clearer vision at distance/near
multifocals
spectacles over-refraction - some px can wear CLs for all tasks however some may also need glasses due to simultaneous vision not giving them the vision the require for certain tasks
explain the shortcomings of monovision fitting (4)
has a success rate of 67% - 2/3rds - while 1/3 unsuccessful
causes reduced stereopsis & contrast
Adaptation period (need to learn suppression of 2 images)
Add > 2.25 D loss of intermediate vision - after +1.50 will lose intermediate vision - some near tasks won’t be able to be done
explain advantages of mono vision and what px it would be a beneficial fit for (3)
Greatest success appears around +1.50D add
best for px with - high astigmatism
and for those that seek perfect vision
why would a patient be refitted from monovision to multi focals
if the add has increased too much - struggling with intermediate vision
explain the process of refitting from monovision to MFs (3)
◦The adapted monovision patient must re-learn to see BINOCULARLY, there is a re-adjustment period so you need to fully prepare them - they need to be fully informed that there will be a longer chair time - adaption period
◦Take them out of monovision, fit distance-only CLs & provide Ready Readers to use for a few days to re-adjust to binocular vision before refitting
◦Fit them that day encouraging them with their ‘range of vision’ especially at intermediate & night driving will be so much better (see in 3D again)
what is another alternative to monovision instead of refitting to MFs (3)
enhanced monovision as an option - complementary to modified mono vision:
SV correction in dominant eye
Bifocal in other eye
what are the different types of modified monovision (4)
Dominant eye | Non dominant eye |
Single vision cl for distance | Multifocal lens biased towards near prescription |
Multifocal biased for the distance (not fitting full reading addition) | Multifocal lens biased towards near prescription |
Large OZ for CD design | Small OZ for CD design |
Small OZ for CN design | Large OZ for CN design |
what px should NOT wear a multifocal contact lens (4)
◦Monocular patients - strabismic or blind eye - cannot have 2 eyes seeing 2 separate things
◦Poor binocularity - Intermittent diplopia
◦Amblyopic patients
◦Poor BCVA in either eye - cataract
what px may struggle with multifocal CLs (5)
◦High astigmatism, especially oblique axes
◦Perfectionist personalities, unwilling to #compromise
◦High adds +3.00 and above
◦Low myopes with low adds
◦Emmetropic presbyopes - if they see perfectly in distance will be unwilling to go degraded distance vision
what is pseudophakia (2)
◦Anyone who has a SV IOL after surgery is pseudophakic and will become a full presbyope – regardless of age
◦Fit as per fitting guide for adults with multifocal contact lenses
explain what paediatric aphakia is and how it should be corrected (5)
due to congenital cataract - has to be removed
however as they cannot take an IOL due to immature anatomy - will need CLs/spectacles in place for distance and near until then
Multifocal contact lenses would be an appropriate option for these children once they have a SV IOL in place and have adult like physiology, such that the standard lenses fit
Extended range MF CL are possible in hydrogel for the event that the child does not have an IOL yet in place, by school going age
CD both eyes - High adds
probability of success with MFs
High probability of success | Moderate probability of success | Low probability of success |
Moderate to high hyperopia | Moderate to high myopia | Low ametropia or emmetropia |
No astigmatism | Astigmatism <1 dp | Astigmatism >2 dp |
Young presbyopes, low addition | Medium presbyopes, medium addition | Old presbyopes, high addition |
Normal pupil size (3–5 mm) | Large pupil size (>5 mm) | Small pupil size (<3 mm) |
Highly motivated | Moderately motivated | Not motivated |
Aware of vision compromise | Accept not much vision compromise | Unrealistic expectations |
Good manual dexterity | Medium manual dexterity | Poor manual dexterity |
Frequent changes in focus | Long time in near work | High visual demands (night driving) |
AIR OPTIX Aqua Multifocal
CN and aspheric
low add up to +1 / medium – +1.25 to +2 / high is above +2
PureVision Multifocal
Aspheric - just have low and high
undesirable (broad range of adds that are covered) – low = 0.75 to 1.50 / high 1.50-2.50
if between 1.50 and a 2 (which one will work best) may result in fitting unequal additions – however px dependent
Biofinity Multifocal D/N
only CL that has CD design
unique – they have specific adds no low, medium or high – order according to px rx
ACUVUE Oasys for Presbyopia
strictly bifocal – concentric not aspheric in design
has a definitive plus ,minus, plus, minus – not discrete
explain the use of daily disposable multi focal lenses (4)
•Convenient
•Part-time wear - occasions
•No CL care products – as disposable
•Targeted materials for ‘dry eye’ – designed to treat a dry eye – materials best manufactured for px prone to DE
when would translating lenses be fitted and who would we NOT fit these lenses on (5)
not very common in a soft CL design - would only really be fit for a custom lens order
exclude fitting for:
•Loose lower eyelids – lens would drop below – uses lower lid to rest on
•Atypical lid apertures - lower lid too far above limbus / lower lid below limbus
•Poor or ‘flick’ (incomplete) blinkers
•Near vision at or above eye level
how do we assess the fit of multi focal lenses (3)
Visualize reading segment position using an ophthalmoscope
cannot use retinoscope - will not be able to determine with and against movements as multiple powers within the pupil
can use ophthalmoscope to determine sufficient coverage with pupil in diff POF to be able to read
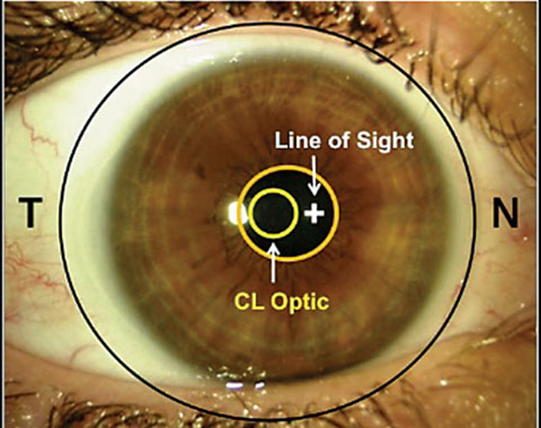
what is the KEY consideration for concentric and aspheric lenses
CENTRATION – as power lies in middle of the lens – needs to matched with pupil - so needs to be centred well
what is the KEY consideration for translation lenses
MOVEMENT and LID RELATIONSHIP – px can only read if lens moves – can move in that gaze – not too tight that it doesn’t move up when px looks down