Trauma VIVA 2
1/148
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
149 Terms
pathophysiology of a tension pneumothorax
air becomes trapped in the pleural space
as a result of positive pressure or decreased ventilatory effort (fatigue) the air in the pleural space expands
this increased pressure collapses the lung
a injury to lung acts as a one-way valve that allows air into the pleural space, but not out - on exhalation injury seals
how is a pneumothorax treated in hospital?
open thoracostomy
tube thoracostomy
a chest tube is inserted into the pleural space to remove air or fluid between the 4th or 5th intercostal
the tube is a closed one-way drainage system preventing air from re-entering
can also be done by HEMS
sucking chest wound pathophysiology
a pneumothorax associated with chest wall defect (eg penetrating injury)
air enters pleural space directly from external environment, and causes lung to collapse
open pneumothorax
air moves in and out of sucking chest wound
what is the treatment for open pneumothorax?
chest seal
chest tube
surgical repair of injury site
how does a chest seal work in open pneumothorax?
prevents outside air from entering chest cavity during inhalation
what is a haemothorax?
accumilation of blood in the pleural space often caused by thorax injury
what is the treatment for haemothorax?
thoracotstamy drains blood from the pleural space allowing the lung to expand
HEMS can perform thoracostamy (tube or open)
TXA
high flow oxygen
immediate transport
permissive hypertension/bloods
flail chest pathophysiology
two or more rib fractures per rib in three or more ribs
causes free floating segment
results in paradoxical movement of the chest wall
instability of chest wall prevents lungs from fully expanding leading to breathing difficulties
additionally pain results in shallow breathing
this is an injury that may cause pulmonary contusion which then impairs gas exchange
flail chest treatment
oxygen
pain management
positioning
low threshold for advanced car team as these pts can deteriorate quickly
what is obstructive shock?
physical/mechanical obstruction that prevents the heart from filling or pumping effectively
this leads to impaired cardiac output
causes of obstructive shock
cardiac tamponade
tension pneumothorax (mediastinal shift?)
PE
what is a primary brain injury?
occurs at the time of impact
direct injury to the brain
damage done - aim to reduce/control secondary brain injury
what is a secondary brain injury?
later + indirect injury to the brain that occurs after primary brain injury
occurs as a result of physiological factors (eg inflammation, reduced o2 etc)
systemic causes
what is a coup/contra-coup injury?
severe TBI/focal brain injury
impact to skull causes brain to move within skull (coup)
brain hits opposite point of skull (contra-coup)
what is a focal brain injury?
localised injury to a specific area of the brain
commonly caused by contusions, lacerations for vessel damage
what is a brain contusion?
TBI
localised bruising/bleeding on the brain surface often caused by direct impact
size of contusion determines extent of injury
what is a diffuse axonal injury?
A TBI
caused by shearing of nerve fibres and white matter which causes damage and disrupts the transmission of electrical impulses
happens when brain rapidly accelerates/decelerates inside of the skull
causes widespread damage
happens after high speed accidents
what are the types of skull fracture?
linear (80%) - straight line fracture
depressed - broken skull pressed inwards towards brain
open/closed
basilar - fracture to base of skull
systemic causes of secondary brain injury
hypoxia
increased/decreased CO2
hypotension
anaemia
BM changes
intracranial causes of secondary brain injury
seizures
cerebral oedema
haematoma
increased ICP
warning signs of increased ICP
decreased GCS
sluggish non-reactive pupils
hemiplegia
hemiparalysis
cushings triad
cushings triad
increased ICP
bradycardia
widened pulse pressure/hypertension
irregular resps
what is the Monroe Kelly hypothesis?
the skull is a rigid box and its volume is fixed
CFS, blood and brain tissue fill the skull
an increase in one of these components decreases the room left in the skull and thus increases intracranial pressure
what order is the spinal column anatomy
cervical - 7
thoracic - 12
lumbar - 5
sacrum - 5
coccyx - 4
what is the pathophysiology of spinal trauma
within the spinal cord are the motor and sensory nerve tracts
damage to these areas may result in weakness or paralysis, pain
impact of high cervical injury
loss of total ability to breathe
c3, 4 and 5 keep the diaphragm alive
can cause complete paralysis neck down
loss of autonomic control
impact of lower thoracicl injury
T2-11 keep intercostals from heaven
diaphragm functions, loss of intercostal muscles
hypotension associated with spinal trauma
hypotension occurs as a result of loss of sympathetic nervous control
loss of SNS control results in vasodilation, bradycardia and warm dry skin (results in blood pooling)
common in injuries above T6
neurogenic shock
hypovolemia needs to be treated as primary cause
how should increased ICP be prevented?
head packaging up
no ligatures
reduce gagging/vomitting (mindful of adjuncts + ondans)
analgesia
minimise restraint
pathophysiology of pelvic injury
usually occur as a result of high force blunt injury and are associated with polyinjury
high energy damages pelvis (eg pelvic ring)
shearing and tearing forces damage major vessels causing massive internal bleeding (entire blood volume can be lost into pelvis)
this can result in haemorragic shock
what is an anterior/posterior pelvic fracture?
open book fracture
fractures that widen the pelvis
severe risk of bleeding and neuromuscular injury
pt needs massive blood therapy and haemorrhage control
what is the in hospital treatment for open book pelvic fracture?
patient stabilisation - aggressive fluid resuscitation with major blood transfusions
pelvic binding to stabilise pelvis and stop bleed
peritoneal packing
surgical intervention to fix pelvis
antibiotics, pain meds, wound cleaning, rehab
what are the two types of pelvic fractures?
stable - fracture to pelvic ring however it remains intact
unstable - fractures to pelvic ring in two or more places making it unstable. often associated is bleeding
cardiac tamponade pathophysiology
blood fills the pericardium which increases pressure within the sac
this results in the heart being unable to refill or pump blood into circulation
the chambers become depressed limiting filling of heart and reducing stroke volume
results in reduced cardiac output
type of obstructive shock
caused often my penetrating injuries
cardiac tamponade treatment
HEMs can perform clamshell thoracotamy
surgical procedure to expose and access the thoracic cavity
cardiac tamponade can be identified
blood can be removed from the pericardial sac
open cardiac massage can be performed to restart the heart
what is a mid shaft femur fracture?
a fracture to the mid point of the thighbone
requires severe force
these fractures carry the risk of internal haemorrhage as the femoral shaft is highly vascular (1.5L)
risk of hemorrhagic shock
how is a mid shaft femur fracture treated?
Kendrick spint
applies traction to limb and aligns fracture ends
surrounding muscle and tissue tighten to compress vessels
contraindication of kendrick splint
tib/fib fracture
ankle, foot, lower leg injury
what is an open thoracotstamy
CCP skill
surgical procedure
large incision to chest wall with the intention to decompress a tension pneumothorax by attending to air leaks and the injured lung
used in cardiac arrest in suspected TP cause
what is a pneumonix?
large-bore needle used to decompress TP in self ventilating pt
CCP skill
what is a surgical cricothyroidectomy?
scalpel, bougie and tube
gaining front of neck access in cardiac arrest
airway obstruction/occlusion
CCP skill
what is a rapid sequence induction?
anaesthesia to place ET tube
used in pts with traumatic injury who have lost their airway
common in TBIs
what is a resuscitative hysterectomy?
surgical procedure to remove foetus from uterus of pregnant pt in cardiac arrest with traumatic pathology
aims to improve the mothers survival by improving cardiac output by relieving pressure on vessels
neurogenic shock triad
neurogenic shock is a type of obstructive shock
Bradycardia
hypotension
peripheral vasodilation (warm, flushed, dry skin)
why does flail chest cause paradoxical movement
the flail segment moves as a result of pressure changes
the rest of the chest wall moves as a result of muscle action
the segment no longer has this muscle support
traumatic causes of cardiac tamponade
penetrating wounds eg stabbing, impalements
blunt trauma eg impact into steering wheel in RTC
gunshot wounds
medical causes of cardiac tamponade
infectious pericarditis
aortic dissection
what is the trauma triad of death?
each condition exacerbates the other, leading to rapid deterioration so needs to be rapidly acknowledged and addressed
acidosis - impaires enzyme reactions, speeds up fibrinogen breakdown and reduces platelet function
hypothermia - impaired enzyme reactions necessary for blood clotting
impaired clotting
all results in severe blood loss in trauma patients
underlying process of trauma triad of death
hypovolemic shock results in inadequate tissue perfusion which kickstarts triad
hypoxia causes cells to use anaerobic respiration which releases lactic acid into bloodstream causing acidosis, affecting coagulation
bloodloss and reduction in metabolic processes cause hypothermia, which impacts platelet production and enzyme reactions necessary for clotting
acidosis and hypothermia result in coagulopathy
what specialties are available at MTC?
orthopaedic surgery
neurosurgery
vascular services
cardiothoracic surgery
maxillo facial + plastics
specialised trauma teams
27/4 access to these teams
what specialties are available at trauma centres
trauma centres offer immediate resuscitation, stabilization, and care for less severe injuries
patients for severe life threatening injuries may need to later be transferred to MTC after stabilisation
what are the negative impacts of secondary transfer from TC to MTC?
treatment delay
risk of deterioration during transfer
what type of injuries may lead to neurogenic shock
injury to the spinal cord - often above T6
penetrating injuries that damage the spinal cord
side effects from spinal cord Anastasia
inflammation of spinal cord - transverse myelitis
how do seizures cause secondary brain injury?
contribute to hypoxia
exitotoxicity causes cell death
why does hypoxia cause secondary brain injury
depleted ATP
this causes excess glutamate production which causes exitotoxicity
this causes neurones to become damaged or die
why does hypercapnia cause secondary brain injury?
causes cerebral vasodilation which increases blood flow in the brain which thus increases ICP further
why does hypocapnea cause secondary brain injury?
causes cerebral vasoconstriction
reduces blood flow to the brain which causes hypoxia and tissue death
differentiating between tension pneumothorax and haemothorax?
percussion - TP hyperesonant (air), haemothorax (hyporesonant (blood)
TP - distended neck veins, haemothorax flat neck veins due to hypovolemia
TP = obstructive shock, mediastinal shift. haemothorax = hypovolemic shock
txa indication
head injury pt GCS 12 or less
suspected significant internal/external bleed
confirmed miscarriage with excessive bleeding
PPH
within 3 hrs of injury
txa contraindications
known allergy
injury started more than 3hrs ago
suspected GI bleed
txa dose
adults 1G
IV, IO, IM in trauma
paracetamol indication
pain relief (mild/moderate)
high temp with discomfort
what is the dosage for IV paracetamol?
1G every 4-6 hrs
indication for morphine
severe pain
contraindications for morphine
respiratory depression (-10 breaths per min)
hypotension (-90 systolic)
head injury with only pain response/ - GCS 9)
known hypersensitivity
what is the dosage of morphine?
up to 10mg initial dose
max dose of 20mg
indication for ondansetron
nausea/vommiting
this can increase ICP
contraindication for ondansetron
known sensitivity
congenital long QT
infants under a month
dosage of ondansetron
initial dose of 4MG
max dose of 8MG
dose interval of 30 mins
to be given over 2 mins
co-amoxiclav dosage
over 40kg - 1.2G
slow injection over 3-4 mins
when is an IO indicated
trauma (eg burns, hypothermia, TCA, PPH, shock)
cardiac (eg cardiac arrest, MI)
neuro (status epilepticus, stroke, head injury, RSI)
respiratory (all respiratory emergencies)
systemic (sepsis, sickle cell crisis, DKA, dehydration)
when medication/fluids are needed immediately
what are contraindications of IO access?
prosthesis (eg knee replacement)
trauma to bone
no anatomical landmarks
local infection
recent IO (in same bone within 48 hours)
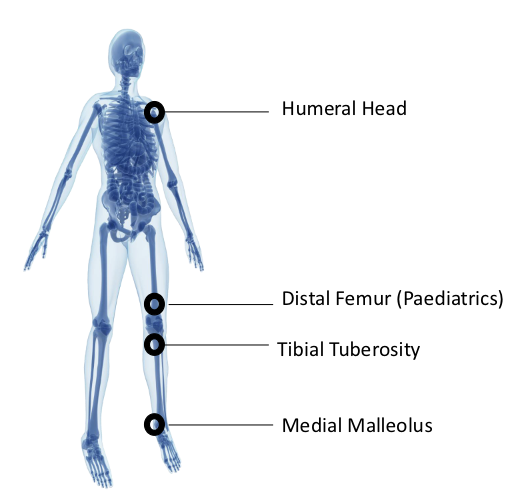
what are the sites for IO access
humeral head
distal femur (paeds)
tibial tuberosity
medial malleolus
bilaterally!!!
what are the IO needle sizes?
pink 15mm - 3-39 KG
blue 25mm - more 3 KG
yellow 45mm - 40KG
how should the correct needle be selected?
depress skin tissue with thumb to gauge depth
confirm with 5mm mark
how should drugs be administered into an IO site?
drugs can’t be dripped, they need to be pushed
eg used three way tap for fluids
under what circumstances can IO be administered in a conscious patient?
altered mental status/GCS less than 8
respiratory compromise SPO2 less than 80 after O2, RR less than 10 or more than 40
systolic BP less than 90
pts in immediate need of medications
profound hypovolemia with altered mental status
what are the indications of needle thoracocentisis
presenting with clinical signs and symptoms of tension pneumothorax
what are the contraindications for needle thoracocentesis?
no tension pneumothorax suggested
how successeful is needle decompression?
canullas will fail in over 1/3 of pts
what is the landmark for needle decompression?
second intercostal space
midclavicular line
above third rib
what are some possible complications of needle decompression?
failure
haematoma
pneumothorax
lung laceration
haemothorax
blocked cannula
displaced cannula
subcutaneous emphysema
air embolism
what is the landmark for needle cric?
ID cricothyroid membrane in midline between Adams apple (thyroid cartilage)
and the cricoid cartilage (next prominent cartilage down from Adams apple)
how is needle cric done?
remove cap and filter of 14g cannula
draw up 2mls air in 10ml syringe
attach o2 tubing to 3 way tap
ID landmark
insert cannula at 45 degrees at a downwards angle + push until give is felt, white aspirating syringe
if air does not enter syringe at this point consider fat plug
remove needle (sharps bin!) and respirate to confirm placement
secure with tape
remove syringe + attach three way tap with o2 tubing on 15L
occlude open port for 1 second for inhalation, then release for 4 seconds exhalation
safe duration of technique is 30-45 mins
what are the indications of needle cricothyroidotomy?
pts in need of oxygen due to life threatening upper airway obstruction
can’t intubate, can’t ventilate
what are contraindications for needle cric?
ability to secure airway by other means
unable to locate/identify landmark
airway trauma rendering access via cricothyroid membrane futile
what are some possible complications of needle cric?
failure
blocked cannula
displaced cannula
posterior trachea puncture
subcutaneous emphysema
hypercapnia
inability to ventilate
when is external jugular vein cannulation indicated?
if IO and peripheral access have both failed/been ruled out
what are contraindications of EJV cannulation?
patients under 18
landmarks cant be identified
one attempt only
should not be first point of attempted access
what are some potential complications of EJV cannulation?
damage to surrounding nerves
damage to surrounding blood vessels including carotid artery
air embolus
potential complications of IO
extravasation - fluids/medications leak into surrounding soft tissue, potentially causing compartment syndrome, tissue necrosis, or skin necrosis
how is EJV cannulation done?
Lay patient supine or even head down slightly.
Turn patient’s head to the opposite side.
Finger on EJV near clavicle to help with tourniquet effect.
Aseptic.
Insert midway down the EJV.
Cannulate in a caudal direction, superficially (10-25 degrees).
Dispose of sharp in sharps bin and secure cannula.
how is IO done?
Aim the needle tip downward at a 45 degree angle to the horizontal plane/90 degrees
Adults: Gently drill into the bone 2cm or until the hub reaches the skin, or you
feel the ‘pop’.Infants: Stop when you feel the ‘pop’ or ‘give’.
what is a burn?
injury caused by exposure to heat/electricity/chemicals/radiation
most commonly affects skin, may also affect airways, lungs, muscle, bone and internal organs
what burns are complex?
all electrical and chemical burns
thermal burns covering critical area
more than 15% TBSA of adult
more than 10% TBSA of child
more than 5% TBSA of child under 1
what are the critical areas?
face
hands
feet
perineum
genitals
major joints
what are the three layers of skin?
epidermis (outermost layer)
demis (nerve endings, blood vessels)
subcutaneous (fat and muscle)
what are the types of burns?
superficial epidermal burns
superficial dermal burns
deep dermal thickness burns
full thickness burns
what are superficial epidermal burns?
involves epidermis only
red + painful
no blistering, no scarring
heals within 7 days
what are superficial dermal burns?
involves epidermis and upper dermis
pale pink, fine blisters, blanches to pressure
extremely painful
heals within 14 days