FSHN 3620 • Exam 2 SG: Ch. 6/7
1/18
Earn XP
Description and Tags
Lactation Nutrition
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
19 Terms
Benefits of breastfeeding for baby
lower risk of:
Diarrhea
Vomiting
Preterm necrotizing enterocolitis
Pneumonia, RSV, whooping cough
Ear infections
Bacterial meningitis
Type 2 diabetes & obesity
Teeth problems
Autoimmune diseases
Dermatitis & wheezing
Food allergies
Mortality
Childhood weight → leaner at 1 yr
Cognitive → increased cognitive ability & higher IQ
Analgesic effects: reduced pain, calmness
Has right amt of macros, micros, & waters
changes composition over time
Sleeping & soothing
Benefits of breastfeeding for mother
lower risk of:
Breast cancer
Ovarian cancer
Endometrial cancer
Quick recovery from childbirth → oxytocin
Increases physical & emotional bonding - strong attachment
Self confidence
Convenient
Helps lose weight
Delays ovulation
Immune system benefits of breastfeeding
Only in breastmilk, not formula
Lactic acid bacteria/bifidobacterium
Mother’s antibodies passed over
decreased risk of:
Respiratory & ear infections
Allergies
ADD
Autism
Asthma
Type 1 diabetes
Increased T-cells
Macrophages, neutrophils, epithelial cells
Immunoglobin A
Better mucosal lining (buterate)
Diverse microbiome
++ Interferon: interferes with viral reproduction.
Lysosome protections against gram-positive bacteria
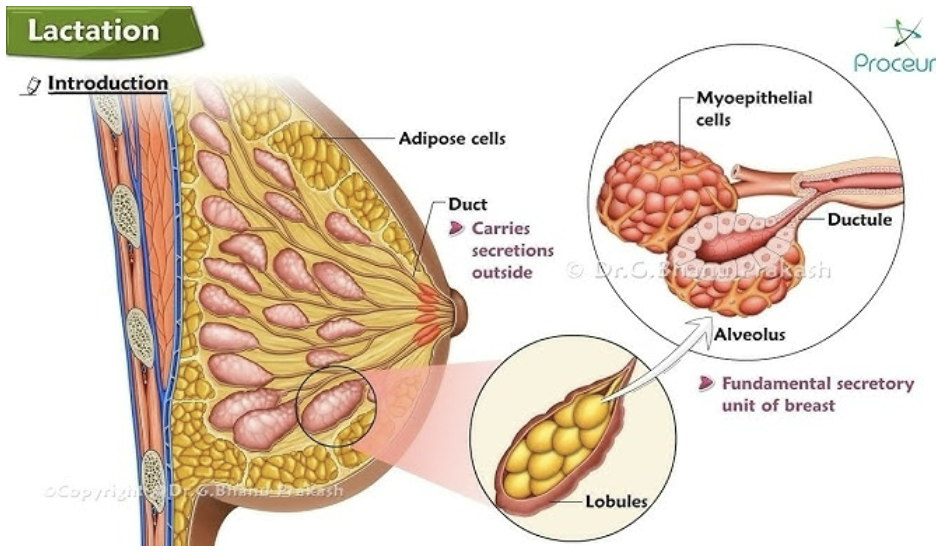
Lactation physiology – how is milk produced?
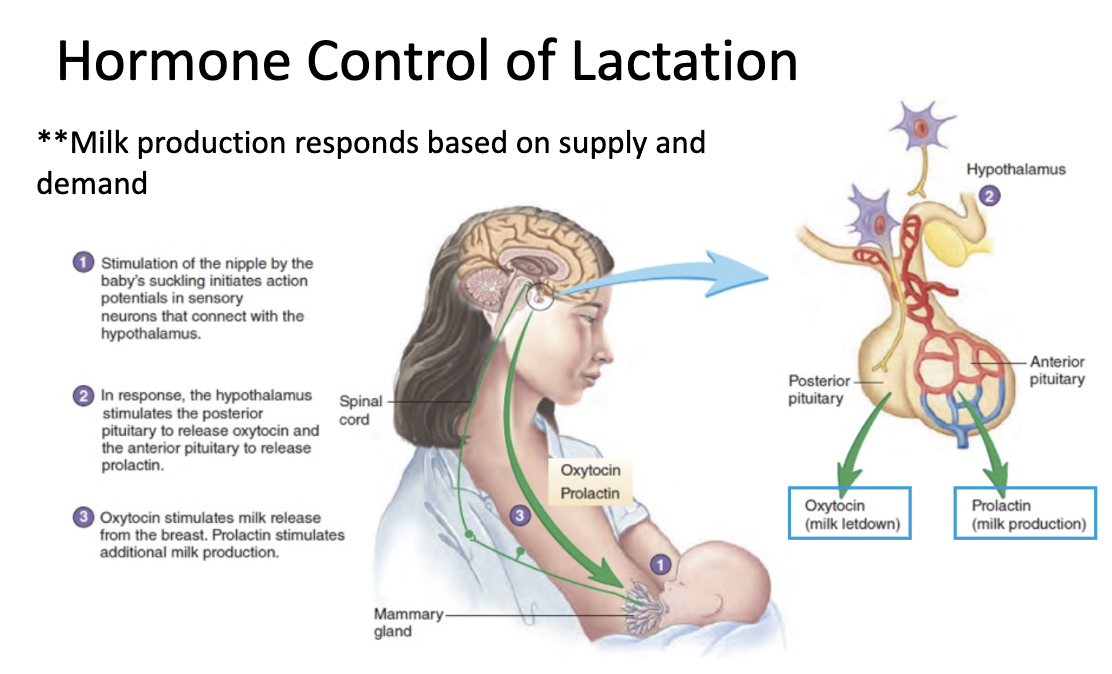
Prolactin: hormone that stimulates milk production.
Stimulated by suckling
Oxytocin: hormone responsible for ejection of milk from milk gland.
Stimulated by suckling or nipple stimulation
Acts on uterus during & after delivery
Hormones involved in lactation – how are they stimulated and what do they do?
SoL = Stage of Lactation
Estrogen
Role: ductal growth
SoL: mammary gland differentiation with menstruation
Progesterone
Role: alveolar development
SoL: after onset of menses & during pregnancy
Human growth hormone
Role: development of terminal end buds
SoL: mammary gland development
Human placental lactogen
Role: alveolar development
SoL: Pregnancy
Prolactin
Role: alveolar development & milk secretion
SoL: pregnancy & breastfeeding (from 3rd trimester → weaning)
Oxytocin
Role: Letdown: ejection of milk from myoepithelial cells
SoL: from onset of milk secretion → weaning
Nutritional composition of breastmilk
Lipids (3-5% mature milk)
Lowest in foremilk, doubled in hindmilk
20.9–26.2 kcal/oz or 65–75 kcal/dL
DHA: retinal development, high IQ scores
Essential for retinal development
Higher concentration in preterm milk
Levels influenced by maternal diet
Protein
Antiviral & antimicrobial effects
Lower content
Classes
Casein
Whey
Mucins
CHOs
Monosaccharides (glucose)
Polysaccharides
Oligosaccharides
200+
Promote growth of beneficial bacteria
Innate immune protection
Lactose: enhances calcium absorption
Dominant CHO
Enhances calcium absorption
Protein-bound CHOs
Cholesterol
Growth & replication of cells
Not impacted by maternal diet
Vit A → growth & development through 6 mo.
Colostrum has x2 conc. as mature milk
Deficient infants → increased risk of eye problems, infection, iron deficiency anemia, & growth failure
Vit D → calcium absorption & bone metabolism
Deficiency occurs when mother is deficient – predisposed to neonatal hypocalcemia & rickets
Vit E → antioxidant, maintains neurological structure & function
Muscle & RBC integrity
Vit K → development of clotting factors & prevents bleeding in newborns
Vit K shot at birth prevents deficiency bleeding
Water-soluble vitamins are responsive to content of maternal diet or vitamin status
Milk provides adequate W-S vitamins
Rare vit B12 status
Minerals
Growth
Contribute to osmolality of milk
Highly available → magnesium, calcium, iron, & zinc
Iron
Vit C & lactose promote iron absorption
Maintained up to 9 mo.
Exclusively breastfed infants are less likely to be anemic
Zinc
Bound to protein & highly available
Rare deficiency – appears as dermatitis or intractable diaper rash
Defect in mammary gland uptake of zinc causes low milk conc.
Trace minerals – copper, selenium, chromium, manganese, molybdenum, nickel, & fluorine are present in small conc.
Essential for growth & development
Not influenced by mother’s diet
Stages of lactogenesis & how they are different from each other
Lactogenesis I: milk begins to form, lactose & protein content of milk increase.
Large gaps between alveolar cells
Begins at 16 wks gestation → few days PP
Colostrum: higher in immunological factors, growth factors, vitamin A, protein, & CHO
Lactogenesis II: increased blood flow to mammary gland & decrease in maternal progesterone levels. Significant changes to milk composition & quality.
2–8 days PP
Tight junctions between alveolar cells close
Clinically – onset of copious milk secretion
Transitional Milk: higher in lactose & lower in sodium.
Lactogenesis III (galactopoiesis): milk production begins, is maintained, and milk composition becomes stable.
9 days PP
Mature milk: higher in cal & fat.
Letdown reflex: an infant suckling at the breast stimulates the pituitary to release the hormones prolactin & oxytocin.
Maternal diet while breastfeeding – what is important? How many extra calories are needed? What nutrients should be a focus?
+ 500 kcal, minimum 1800 kcal/day
Organic, non-GMO, less processed food
Lean proteins → lentils, beans, lean meats
Healthy fats → salmon, chia seeds
Whole grains → oatmeal or quinoa
Fruits & vegetable → colorful
Low-fat milk products → yogurt, cheese
Water → drink to thirst
RDA: 3.8 L
Well-nourished breastfeeding women do not need routine vitamin or mineral supp.
Should target specific needs
Importance of breastfeeding promotion & support
Key teaching points prior to birth
Request early first feeding & skin-to-skin contact
Practice frequent, exclusive breastfeeding
Ask to be taught swallowing indicators
Learn indicators of sufficient intake
Ask for help if it hurts
Know sources for help
Understand PP rest & recovery needs
Avoid supp. unless medically indicated
Peer counselors & peer group discussions
Programs supporting breastfeeding
Farmers Market Nutrition Program
WIC
USDA
Baby Friendly Hospital Initiative
WHO’s International/UNICEF Code on Marketing of Breast Milk Substitute
Maternal exposures effects on breastmilk — DRUGS
Cytotoxic drugs that may interfere with the cellular metabolism of the nursing infant
Drugs of abuse for which adverse effects on the infant during breastfeeding have been reported
Radioactive compounds that require temporary cessation of breastfeeding
Drugs for which the effect on nursing infants is unknown, but may be of concern
Drugs that have been associated with significant effect on some nursing infants and should be given to nursing mothers with caution
Maternal medications usually compatible with breastfeeding
Food and environmental agents having no effect on breastfeeding
Recommendations
Specific knowledge about a medication’s safety
Closely monitor milk production (some meds suppress)
Progestin-only oral contraceptive & implants
Steroid implants & Depo-Provera shot 6 wks PP
Avoid long-acting forms
Schedule doses carefully
Evaluate the infant
Choose drug that produces least amt in milk
Maternal exposures effects on breastmilk — ALCOHOL
Quickly passes into breastmilk
Oxytocin release is blocked, prolactin increased
Gives infant sleeping problems
Infant won’t consume as much milk
Change in odor & flavor of milk
Maternal exposures effects on breastmilk — NICOTINE (SMOKING)
Health risks for infants
Otitis media
Exacerbations of asthma
Respiratory infection
GI dysregulation (colic, & acid reflux)
SIDS
Lower milk output
Lower fat concentrations
Change in odor & flavor of milk
Within gradual intake in days time → infant can metabolize nicotine in liver & excrete chemical in kidney
Exposure to organochloride pesticides, PCBs & hexachlorobenzene through breast milk & second-hand smoke
Safety of nicotine gum in lactation has not been determined
Stop smoking or avoid smoking before feeding & around infant
Maternal exposures effects on breastmilk — E-CIGARETTES & VAPING
Little research about effects
Stop smoking or avoid smoking at least 30 min before breastfeeding & breastfeed right before smoking
Maternal exposures effects on breastmilk - MARIJUANA
Delta-9-tetrahydrocannabinol (THC), an active ingredient in marijuana, transfers and concentrates in breast milk and is absorbed and metabolized by the nursing infant
decrease in infant motor development at 1 year of age
impairment of DNA & RNA formation & neurotransmitter systems essential for proper growth & development has been described
increased risks in behavior & neurodevelopmental problems
Maternal exposure effects on breastmilk — CAFFEINE
Moderate intake causes no problems for most breastfeeding mothers & babies
A dose of caffeine equivalent to a cup of coffee results in breast milk levels of 1% of the level in maternal plasma &, consequently, low levels in the infant
Accumulates in the infant
symptoms – infants being wakeful, hyperactive, & fussy
Some infants are sensitive to caffeine intake, monitor it
Recommendations for limiting exposures to breastmilk
Avoid smoking & drinking
Be aware in purchasing homes built before 1978 (lead paint)
Eat variety of foods low in animal fats
Increase consumption of grains, fruits, & veggies
Eat organic if possible
Avoid fish high in mercury (swordfish, shark, tuna, king mackerel, tilefish, & locally caught fish from areas with fish advisories)
Limit exposure to chemicals
Tap water through home filter
Remove plastic cover of dry-cleaned clothing, air out garments
Avoid occupational exposure to chemical contaminants
Alert other family members to be sensitive to contaminant residue they may bring into the home
Neonatal jaundice
yellow discoloration of the skin caused by too much bilirubin in the blood (hyperbilirubinemia)
Common & benign, goes away on its own/minimal intervention
Serum bilirubin levels: 5–7 mg/dL (85–199 mol/L)
Risk factors (maternal)
Diabetes
Rh sensitization
Previous child with phototherapy
Race: East Asian or Mediterranean
Risk factors (infant)
Premature or late-term
High total serum bilirubin levels at discharge
Poor breastfeeding in exclusive breastfed infant
Blood group incompatibility e.g. ABO
Hemolytic disease e.g. Glu-6-P dehydrogenase deficiency (G6PD)
Kernicterus
The chronic and permanent clinical sequelae that are the end result of very high untreated bilirubin levels. Excessive bilirubin in the system is deposited in the brain, causing toxicity to the basal ganglia and various brainstem nuclei.
AKA bilirubin encephalopathy
Mortality 50%
Survivors burdened with — cerebral palsy, hearing loss, paralysis of upward gaze, intellectual & other handicaps
Increased bilirubin leads to seizures and brain damage
Treatment & Prevention
AAP guidelines for the management of hyperbilirubinemia in healthy term infants
Guidelines for newborns in the nursery
All babies should be monitored over the first few weeks
Continuation of breastfeeding
Breastfeeding preterm infants
Nutritional benefits
Ease of protein digestion
Fat absorption
Improved lactose digestion
Healthy & Development Benefits
Better visual acuity
Greater motor & mental development (1.5 yrs)
Greater verbal intelligence (7-8 yrs)
Lower incidence of serious infectious disease
Enterocolitis & sepsis
Nosocomial infection rates decreased
Antibodies in milk via entermammary system