COMPOSITE RESINS II & III
1/42
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
43 Terms
what are dental composite resins composed of
methacrylate resin (bulk)
silica powder (filler)
photoinitiator
stabiliser
typically with pigments
what is considered a composite material
where two or more materials are combined in such a way to produce improved properties they are commonly termed composites
e.g. fibreglass
more detailed composition of dental composite resins
matrix: mixture of methacrylate resin monomers
most commonly bis-GMA (formed by the reaction of glycidyl methacrylate with bis-phenol A)
filler: typically a silica powder (SiO2)
other materials like zirconia are also added
photoinitiator
e.g. camphorquinone
inhibitors: for shelf life
what is the main resin monomer in all composites
bisphenol A-glycidyl methacrylate (bis-GMA)
what other monomers are added to composites and what properties do they contribute
to reduce viscosity and improve mixing
e.g. triethylene glycol dimethacrylate (TEGDMA), urethane dimethacrylate (UDMA)
how are dental composites set
by either chemical cure or light activation
how does chemical curing work
two pastes are mixed together
an activator + a free-radical initiator
this approach is effectively obsolete in restorative materials - previously done in the 60s and 70s
» material polymerises on its own accord
how do light activated systems work
contain a photoinitiator
setting is initiated by exposure to an appropriate lamp
» it is controlled when the material polymerises
what wavelength is camphorquinone activated
approx. 470nm - hence visible blue light is used
what does the term ‘vinyl’ refer to chemically
‘vinyl’ refers to the presence of an electron-rich C=C double bond
name this molecule
what is another term to denote how light activate systems cure/ set
set via free-radical/ vinyl polymerisation
why are photoinitiators needed
the methacrylate vinyl group is a site awaiting release of its internal energy which will be used subsequently to polymerise other methacrylate groups
the key to starting the process of unlocking this internal energy is the creation of a reactive chemical species that seek out the high-density electrons in the C=C
photoinitiators are used to start this process and open up the C=C
what does free radical/ vinyl polymerisation of composite resins lead to
inevitably leads to polymerisation shrinkage
name 3 other photoinitiators apart from camphorquinone
Lucirin
PPD
Ivocerin
what do photoinitiators intend to do
aid the efficiency of photoinitiation of polymerisation and should match the output of the light curing unit
outline the purpose of coupling agents
coupling agents improve adhesion of resin to filler surfaces to increase strength and toughness
they chemically coat the filler particle surfaces
give an example of a coupling agent and outline it
silanes
have been used to coat fillers for over fifty years in industrial composites and dental composite resins
common silane agents:
vinyl triethoxysilane
gamma or 3-methacryloxypropyltrimethoxysilane
what are disadvantages of silanes
silanes age during storage and lose potency
sensitive to water
water absorbed into composite restorations may result in hydrolysis of the silane bond and gradual loss of properties
state properties of dental composite resins
tough and relatively wear resistant
durable
insoluble
aesthetic
can achieve good bond strength with tooth tissue
relatively safe and biocompatible if handled correctly
what are 2 disadvantages of dental composite resins
hydrophobic so need bonding system to adhere to hydrophilic tooth tissue
contract during setting (polymerisation shrinkage)
what did the Norwegian Institute of Public Health conclude in their 2016 review
there was no difference in adverse health effects of composite resins compared to amalgam
risks were very low
although quality of evidence was moderate to low
how many phases are in a composite resin
3
what are the three phases in a composite resin and outline them
organic phase (resin matrix)
monomer, initiator, inhibitors, pigments
dispersed phase (inorganic filler)
glass, quartz, colloidal silica
interfacial phase (coupling agent)
what is the purpose of each phase
organic phase forms the polymer backbone to provide tensile strength
dispersed phase improves mechanical properties (wear and compressive strength) and decreases shrinkage
interfacial phase provides an adhesive bond between organic and dispersed inorganic phases
—
all components of the dental composite contribute to the properties of the final restoration
if a tooth that needs to be restored has a very exposed pulp, what is used to protect the pulp before the restoration is put in
liner
what does composite polymerisation result in
a set matrix containing dispersed filler particles (typically silica)
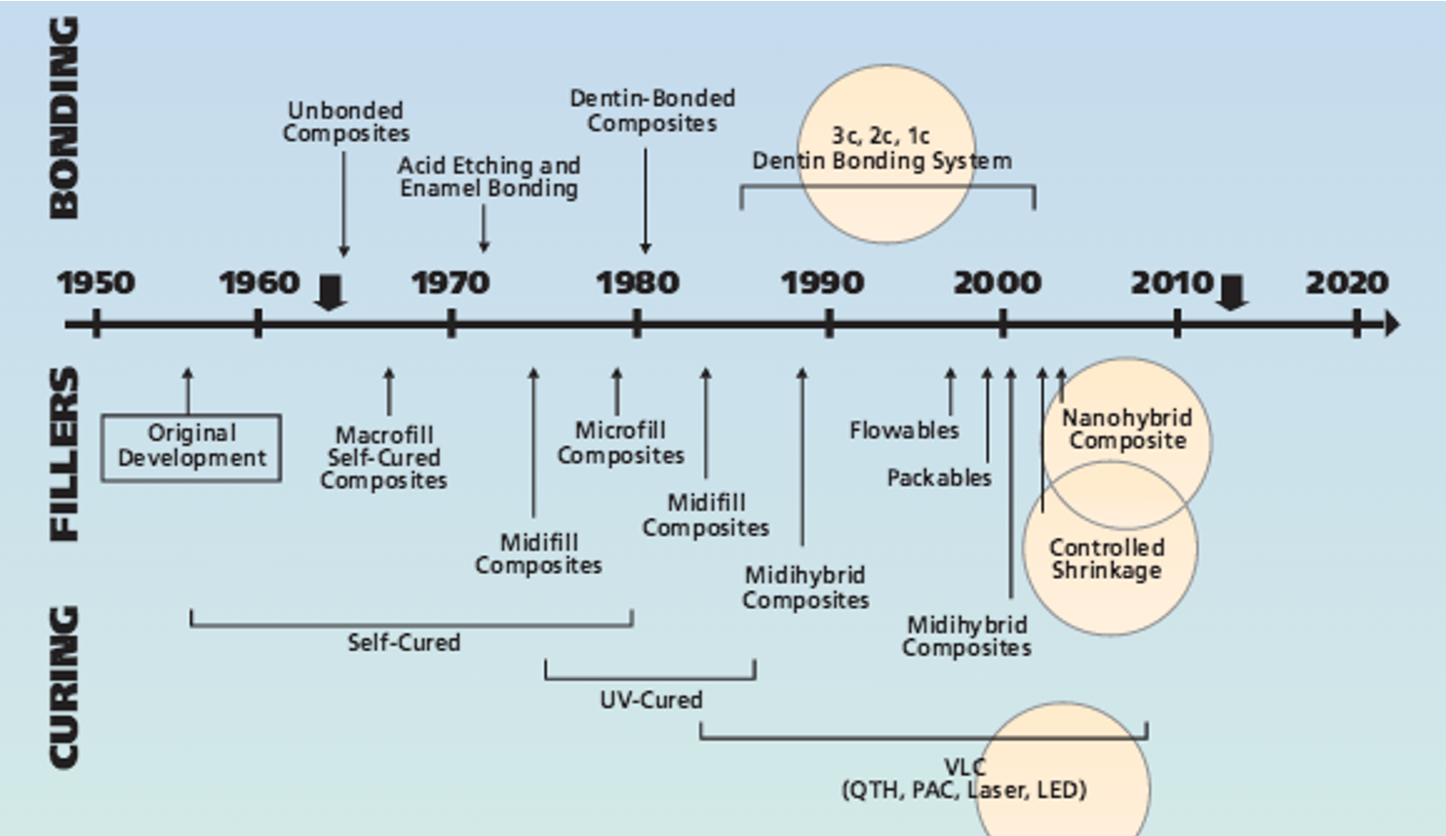
what has been a major evolution in composites
filler particles have decreased in size overtime (the more filler you can get into a composite the less it will shrink)
filler particles have now gotten down to the nano scale
why are big filler particles not ideal
cannot achieve translucency
material would be much more opaque - unaesthetic
smaller filler particles = less polymerisation shrinkage
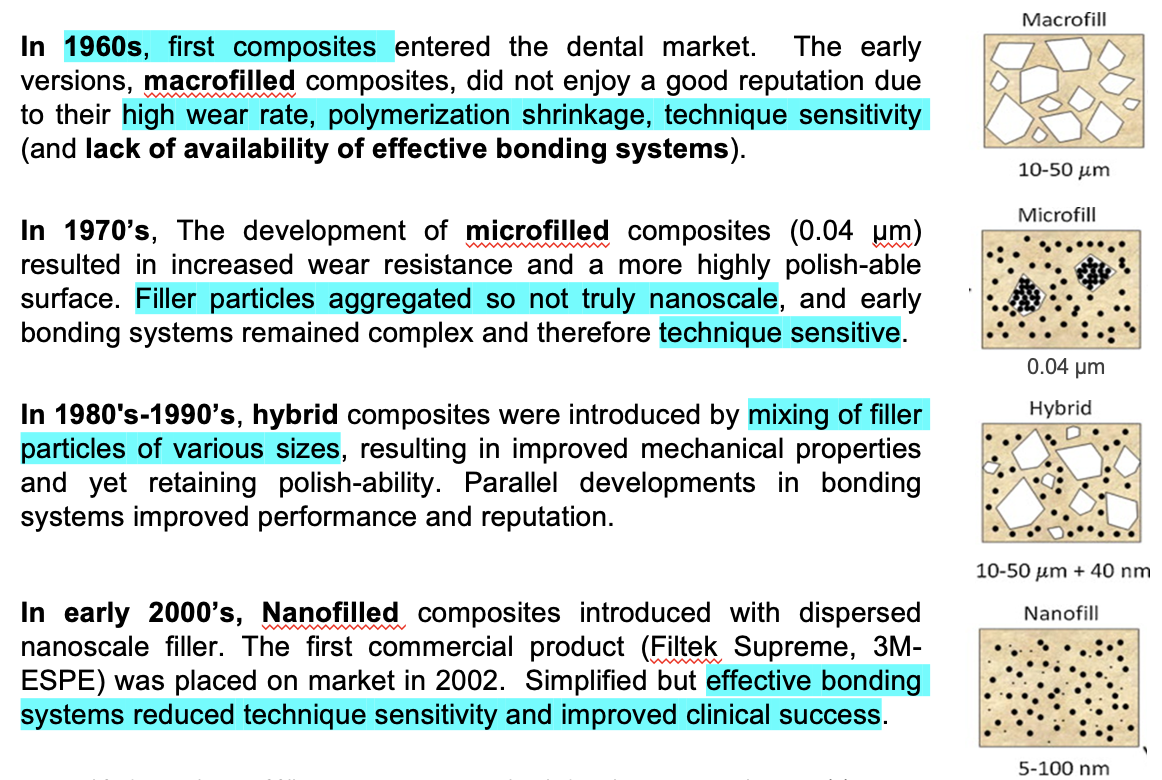
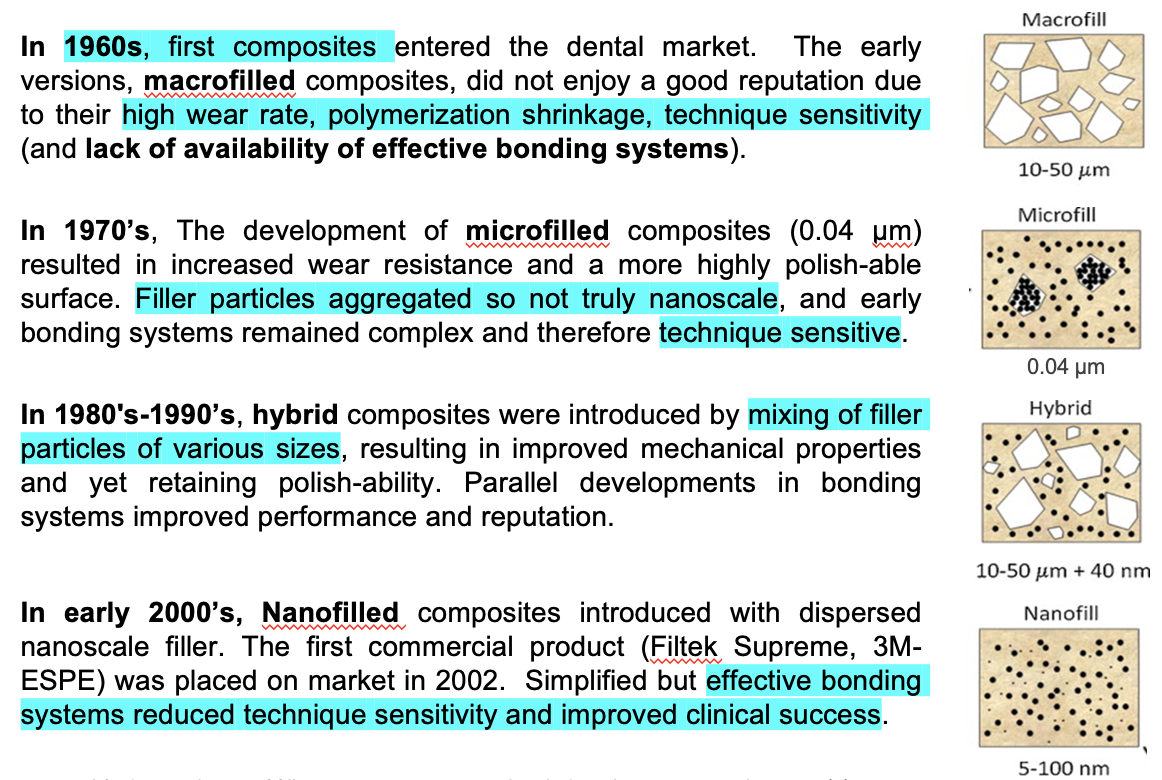
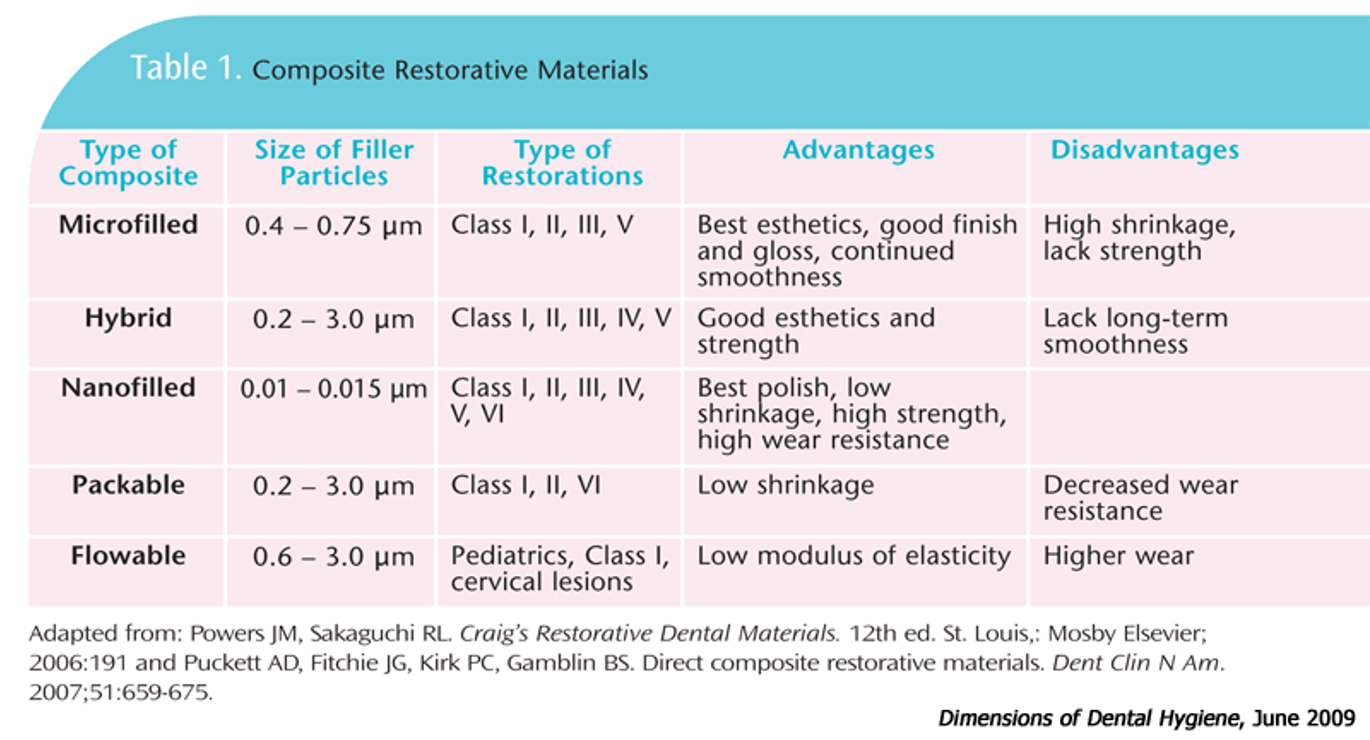
table showing relationship between filler size and properties
what are claimed advantages of nanofilled over conventional composites
potentially superior fracture toughness, high strength and excellent wear resistance
high polishability
very low polymerisation shrinkage
stable and natural interface
high surface to volume ratio which allows higher filler loading to give workable consistencies
nanosized fillers are unable to scatter or absorb visible light which increases translucency » realistic appearance of natural tooth tissue
studies showing properties of nanocomposites
several studies reported reduced wear of nanofilled Filtrek Supreme® compared to hybrid composites and other tooth-coloured restoratives
these studies provide little info. on the mechanisms responsible for reported properties
subject is controversial - at least one paper reporting increased wear for nanocomposites (Turssi et al. 2006)
—
» shows that improvements in material properties do not always manifest as improvements in clinical performance
nano VS micro composites
lab tests show that nanomaterials are more resistant to wear than micro
but composites do not generally fail through wear
how do composites usually fail
fracture
microleakage
secondary caries
what are the advantages associated with decreased filler size
increased resistance to wear and potentially greater strength
increased ability to polish
improved translucency
combined with increased filler volume potential to decrease polymerisation shrinkage
what aspects of composite resin determines clinical outcome
arguably not the selection or quality of the composite that (mainly) determines clinical outcome but:
the correct use of a modern bonding system
good clinical technique e.g. to eliminate moisture contamination or effects of shrinkage
polymerisation shrinkage is inevitable in _____________
methacrylates
what are the risks of bulk composite placement
inadequate cure at depth
shrinkage may cause weak or incomplete interface with tooth tissue » risk of
microleakage, discolouration of margins, secondary caries
how do we clinically minimise polymerisation shrinkage
composite is placed and cured in layers
generally, what is the depth considered to be a reasonable thickness for an individual composite layer
2mm
what is limiting the ‘thinness’ of layers
oxygen inhibition of polymerisation
i.e. if the composite layer is too thin the oxygen from the atmosphere will inhibit polymerisation
timeline showing the evolution of composites