general and oral pathology epithelial pathology and oral manifestations of systemic diseases
1/51
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
52 Terms
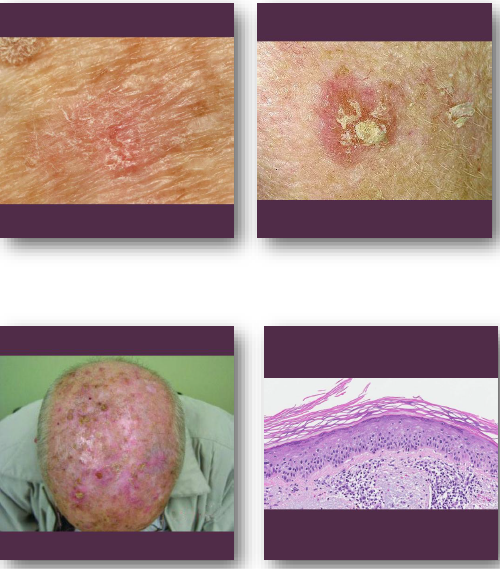
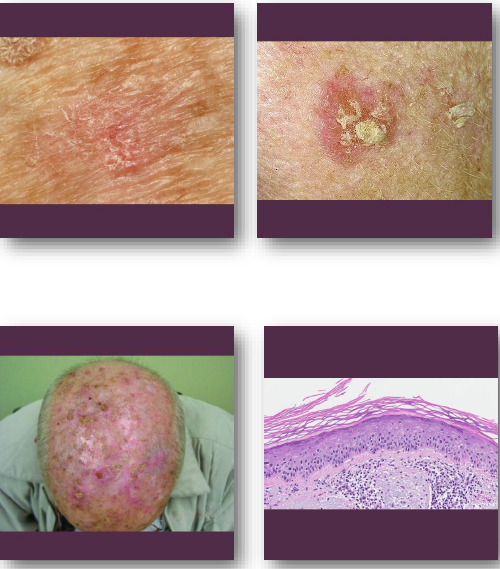
actinic keratosis overview
•Premalignant lesion caused by chronic UV exposure
•Represents early epithelial dysplasia of skin
•Strongly associated with sun-damaged skin
•Precursor to cutaneous squamous cell carcinoma
•Common in fair-skinned older adults
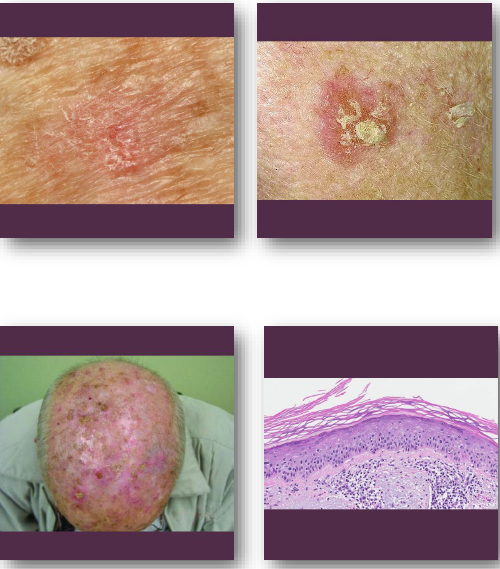
actinic keratosis clinical features
• Rough scaly patch on sun-exposed skin surfaces
• Color ranges from red to tan or brown
• Often easier to feel than to see
• Common on face, ears, and hands
• May be tender or completely asymptomatic
actinic keratosis management and prognosis
• Treated with cryotherapy or topical agents
• Sun protection prevents development of lesions
• Biopsy if lesion thickens or ulcerates
• May progress to squamous cell carcinoma
• Excellent prognosis with early treatment
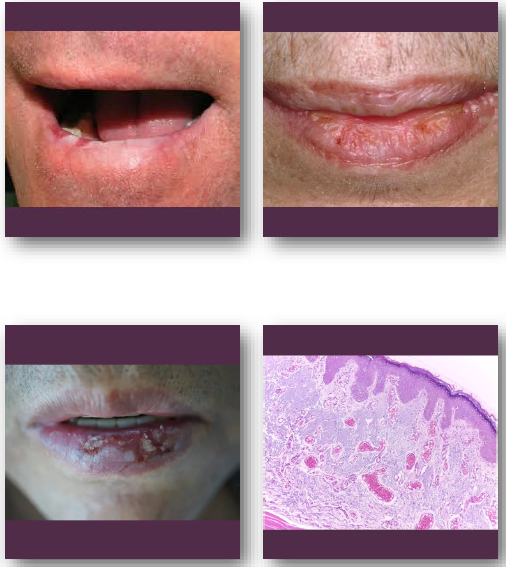
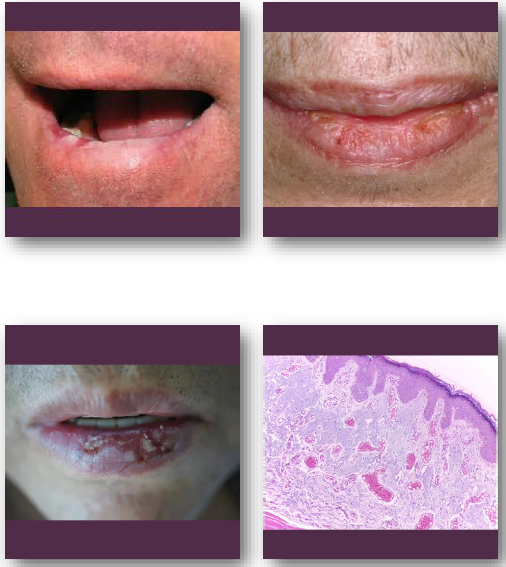
actinic cheilitis overview
•Premalignant lesion of lip from chronic UV exposure
• Represents epithelial dysplasia of vermilion border
•Strongly associated with fair skin and sun exposure
•Most commonly affects lower lip region
•Considered precursor to lip squamous cell carcinoma
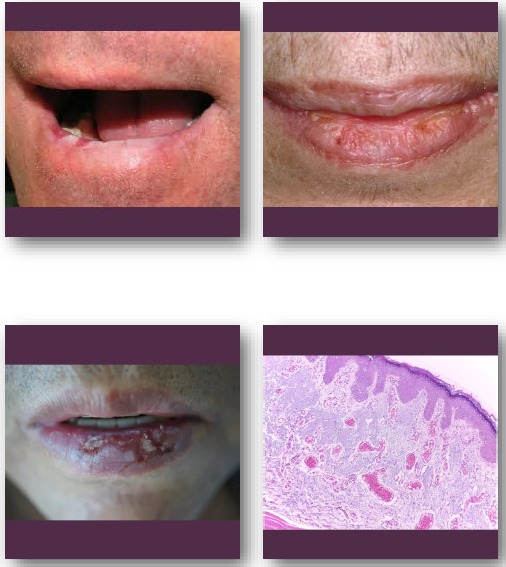
actinic cheilitis clinical feature
•Atrophic, dry, or scaly appearance of lower lip
•Blurring of vermilion border is common finding
•May show fissures, ulceration, or crusting
•Color ranges from pale to erythematous areas
•Usually chronic and slowly progressive
actinic cheilitis management and prognosis
•Biopsy recommended for suspicious or persistent areas
•Sun protection is essential preventive measure
•Topical therapy or surgical treatment may be used
•Regular follow-up required due to cancer risk
•Risk of progression to squamous cell carcinoma
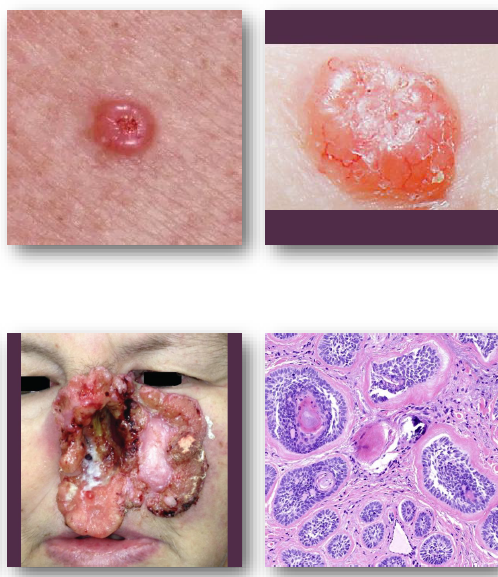
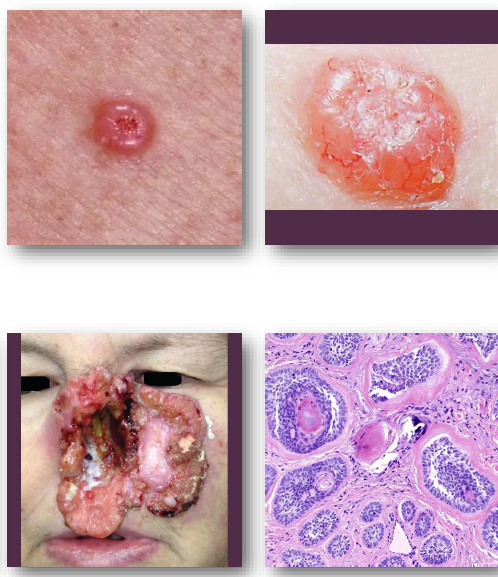
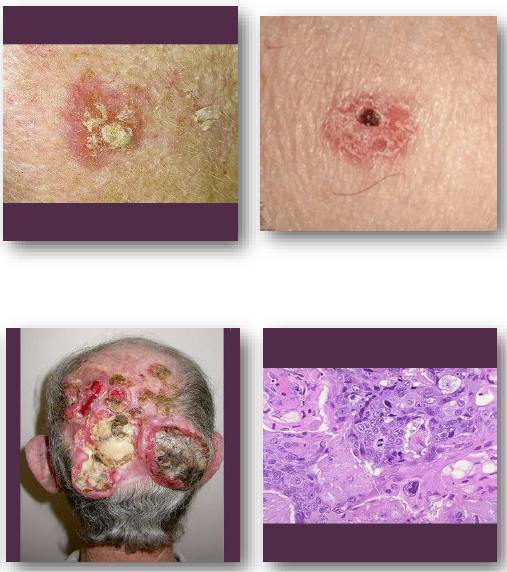
basal cell carcinoma overview
• Most common malignant tumor of the skin
• Arises from basal layer of epithelium
• Strongly associated with UV exposure
• Locally invasive but rarely metastasizes
• Common in fair-skinned individuals
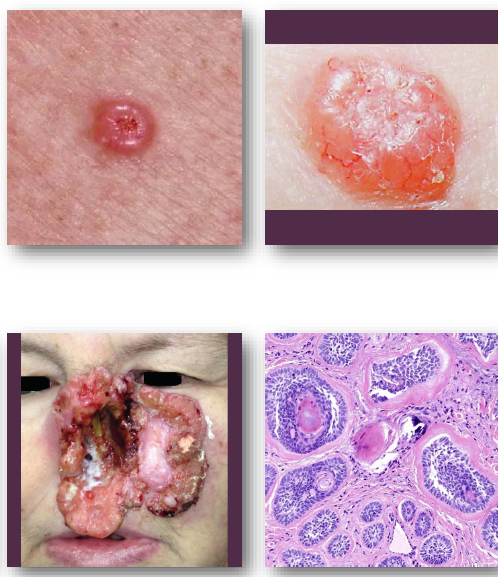
basal cell carcinoma clinical features
pearly papule with rolled and raised borders
central ulceration may be present
surface shows fine blood vessels
common on face and nose region
slow-growing but locally destructive
basal cell carcinoma management and prognosis
Surgical excision is treatment of choice
•Mohs surgery used for high-risk areas
•Excellent prognosis with early detection
•Recurrence possible if incompletely removed
•Rarely metastasizes to distant sites
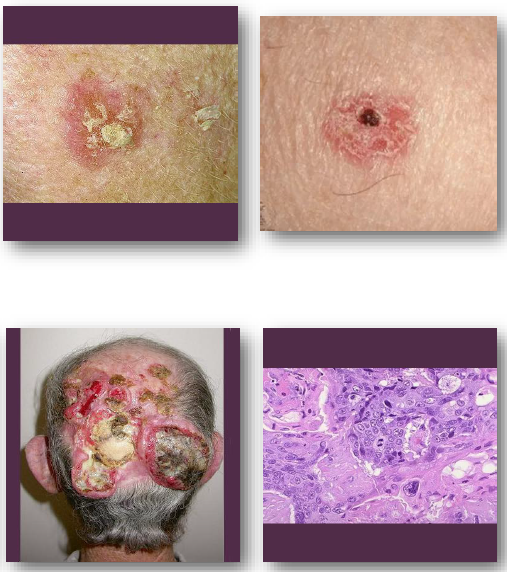
cutaneous squamous cell carcinoma overview
•Malignant tumor of keratinizing epithelium
•Strongly linked to chronic UV exposure
•May arise from actinic keratosis lesions
•More aggressive than basal cell carcinoma
•Risk increased in immunocompromised patients
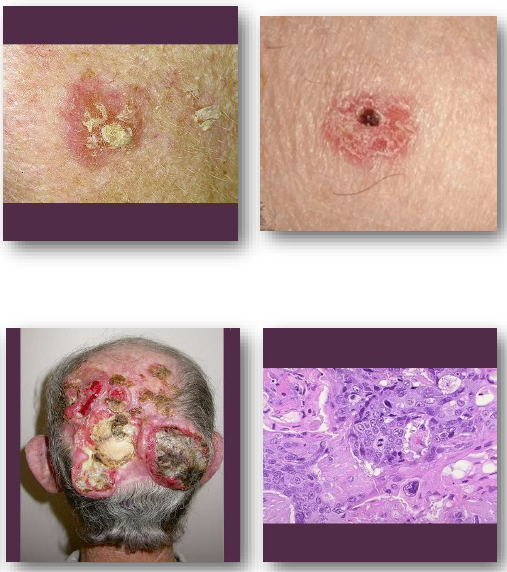
cutaneous squamous cell carcinoma clinical features
•Firm scaly or ulcerated skin lesion
•May present as non-healing ulcer
•Surface may crust or bleed easily
•Common on sun-exposed areas
•Often grows faster than basal cell carcinoma
cutaneous squamous cell carcinoma management and prognosis
•Surgical excision with adequate margins required
•Radiation therapy used in selected cases
•Early detection improves clinical outcomes
•Greater risk of metastasis than BCC
•Requires close follow-up after treatment

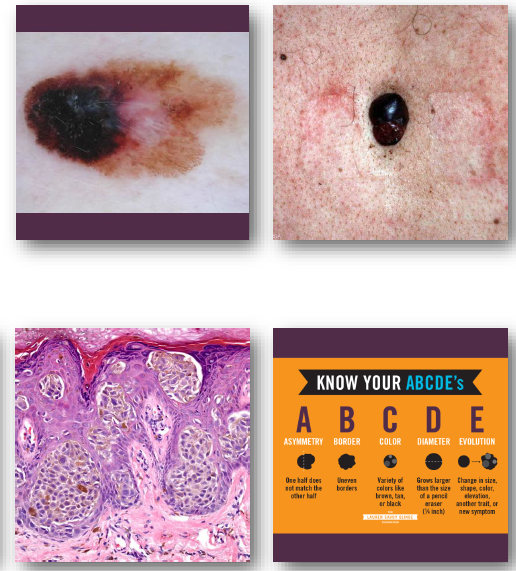
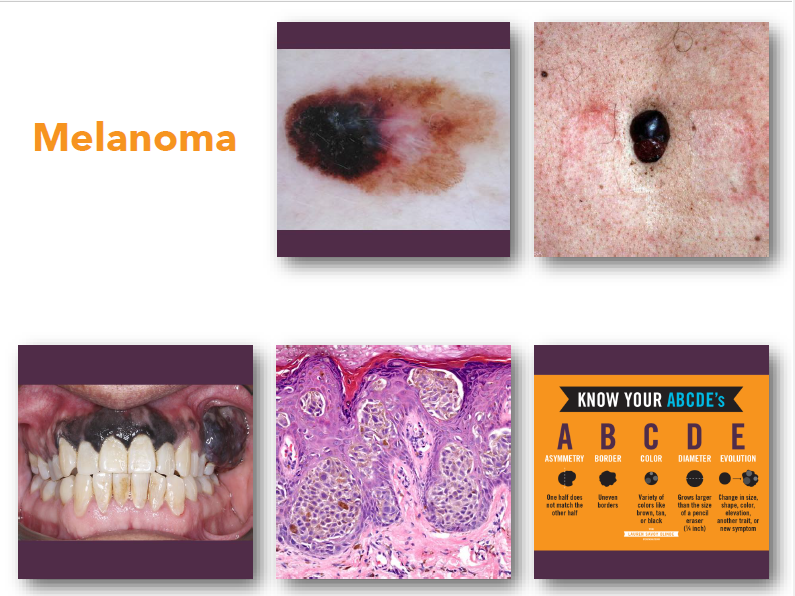
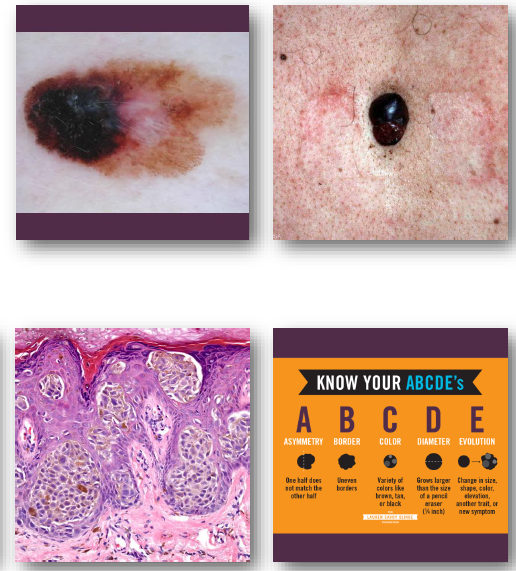
melanoma
•Malignant tumor arising from melanocytes
•Strongly associated with ultraviolet exposure
•Most dangerous form of skin cancer
•Early detection critical for survival
•May occur on skin or mucosal surfaces
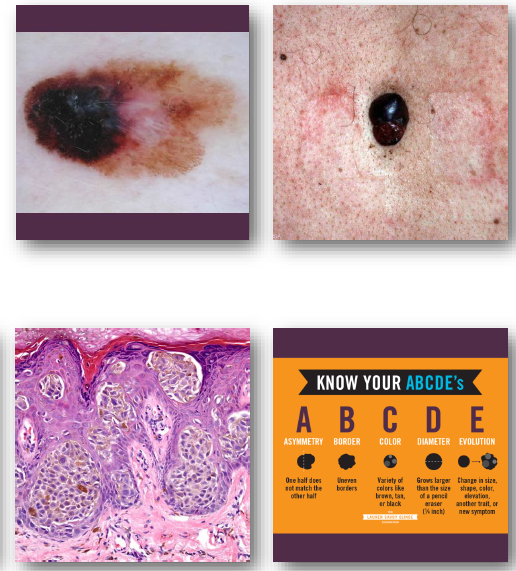
melanoma clinical features
•Irregular asymmetric pigmented lesion
•Varied colors including black and brown
•Borders often irregular or notched
•Diameter often greater than 6 millimeters
•Changes over time are critical warning sign
melanoma management and prognosis
•Early surgical excision is essential
•Prognosis depends on depth of invasion
•High risk of metastasis if advanced
•Requires urgent referral and treatment
•Survival improves with early detection
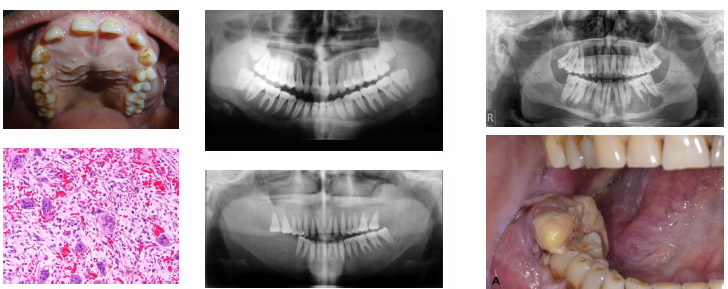
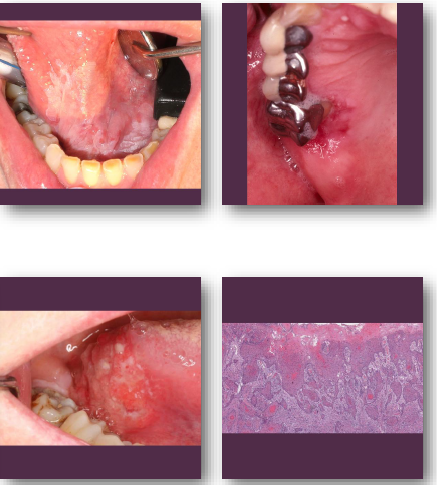
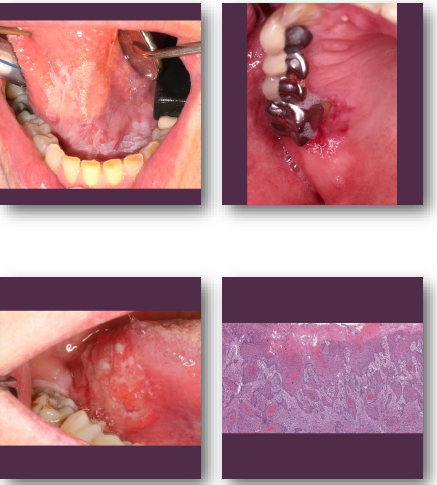
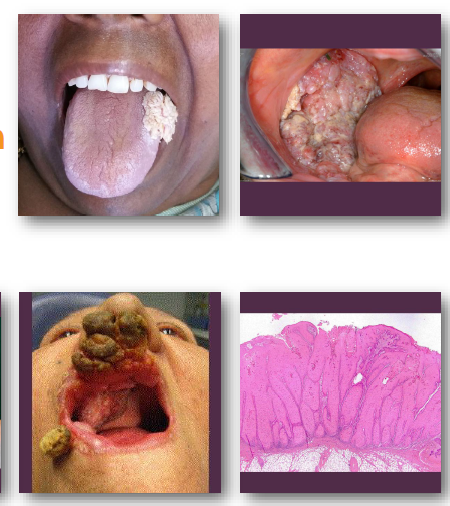
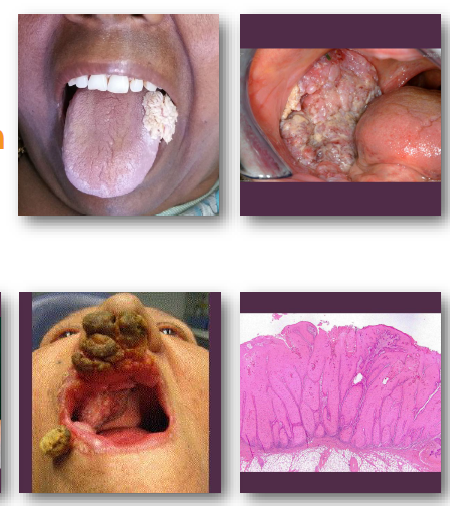
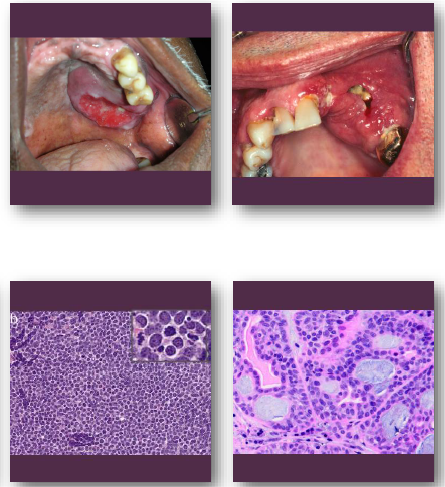
oral squamous cell carcinoma overview
•Most common Malignant tumor of oral stratified epithelium
•Strongly linked to tobacco and alcohol use
•HPV-related cases occur in oropharynx
•Often arises from premalignant lesions
•Includes several aggressive histologic variants

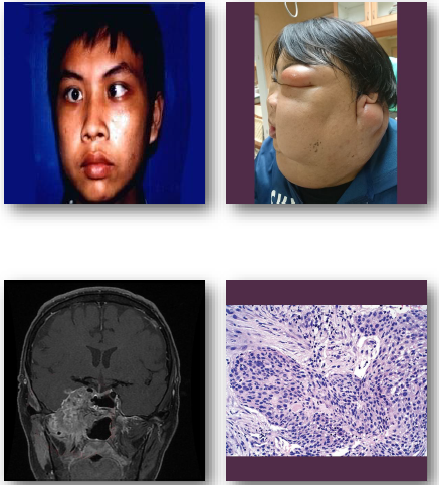
oral squamous cell carcinoma clinical features
•Non-healing ulcer or exophytic mass lesion
•Mixed red and white mucosal appearance
•Induration on palpation is key finding
•Common on tongue and floor of mouth
•May be painless early and painful later
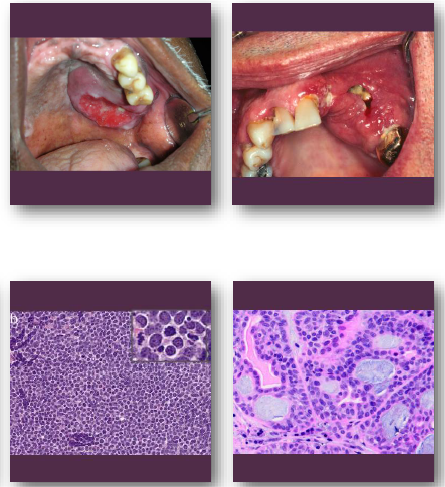
oral squamous cell carcinoma management and prognosis
•Requires biopsy for definitive diagnosis
•Treated with surgery, radiation, chemotherapy
•Prognosis depends on stage at diagnosis
•Variants may show more aggressive behavior
•Risk of recurrence and metastasis exists
Verrucous carcinoma overview
•Low-grade variant of squamous cell carcinoma
•Strongly associated with tobacco use
•Slow-growing but locally invasive lesion
•Rarely metastasizes to distant sites
•Often arises from leukoplakic lesions
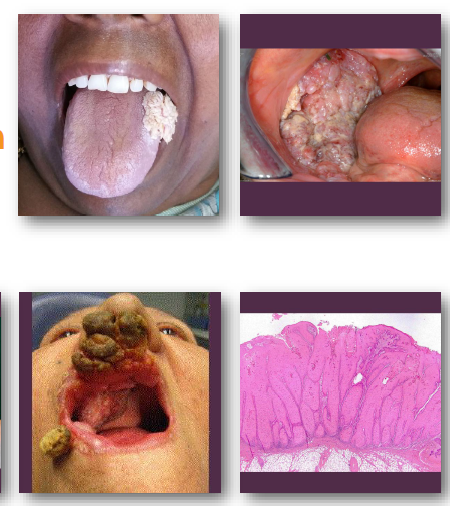
verrucous carcinoma clinical features
•Thick white verrucous or papillary mass lesion
•Broad-based lesion with slow enlargement
•Often involves buccal mucosa or gingiva
•Surface appears rough and warty (verrucous)
•Typically painless in early stages
verrucous carcinoma management and prognosis
•Wide surgical excision is treatment of choice
•Radiation often avoided due to risk factors
•Recurrence possible if incompletely removed
•Excellent prognosis compared to SCC
•Very low metastatic potential
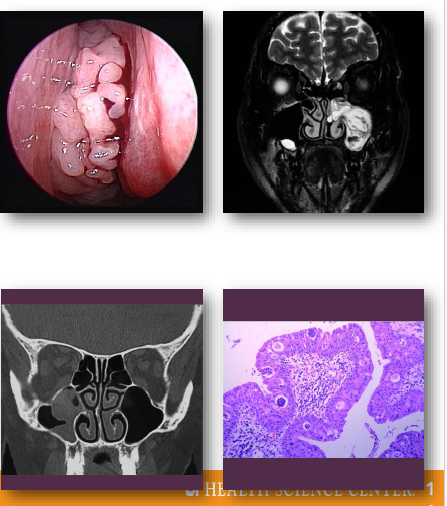
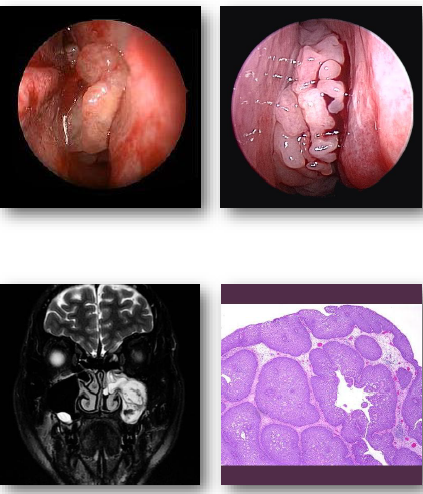
sinonasal papillomas overview
Benign epithelial tumors of sinonasal mucosa
•Includes inverted and exophytic variants
•Associated with HPV infection in some cases
•Locally aggressive with recurrence potential
•Small risk of malignant transformation exists
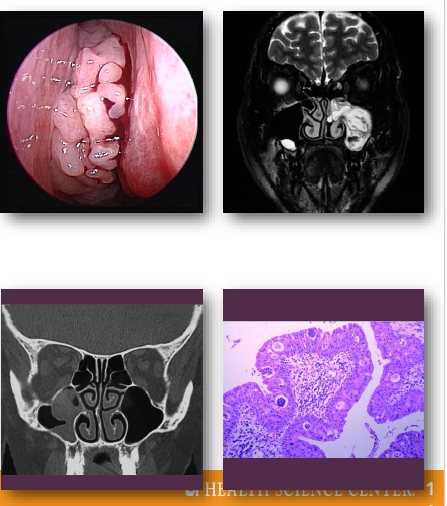
sinonasal papillomas clinical features
•Unilateral nasal obstruction or visible mass
•May present with epistaxis or discharge
•Often arises from lateral nasal wall
•May extend into adjacent sinus spaces
•Symptoms depend on size and location
sinonasal papillomas management and prognosis
•Surgical excision required for treatment
Complete removal reduces recurrence risk
•Long-term follow-up recommended
•Recurrence relatively common
•Small risk of malignant transformation
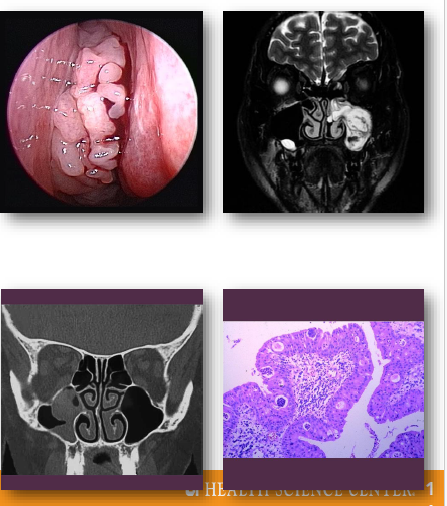
fungiform sinonasal papilloma
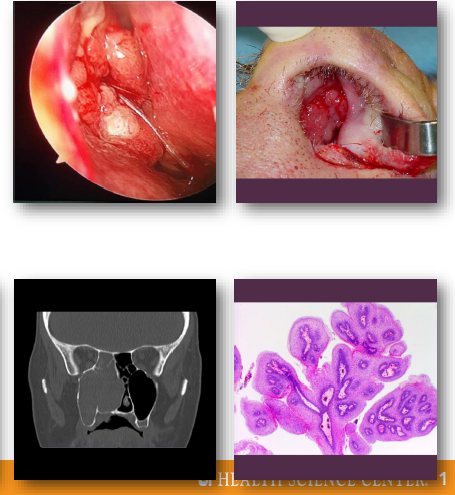
inverted sinonasal papilloma
nasoparyngeal carcinoma overview
•Malignant epithelial tumor of nasopharynx
•Strongly associated with Epstein-Barr virus
•Higher incidence in specific populations
•Often presents late due to hidden location
•Early metastasis to regional lymph nodes
nasopharyngeal carcinoma clinical features
•Nasal obstruction or recurrent epistaxis
•Neck mass from lymph node involvement
•Hearing loss or ear fullness symptoms
•Headache or cranial nerve deficits
•Symptoms often subtle in early stages
nasopharyngeal carcinoma management and prognosis
•Primarily treated with radiation therapy
•Chemotherapy used for advanced disease
•Prognosis depends on stage at diagnosis
•High risk of regional metastasis
•Early detection improves survival rates
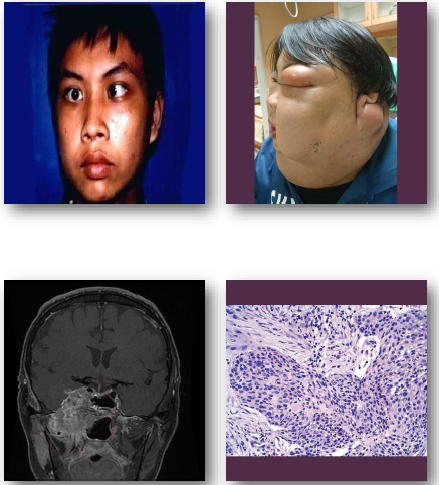
carcinoma of the maxillary sinus overview
•Malignant epithelial tumor of maxillary sinus
•Often squamous cell carcinoma histologically
•Associated with occupational and environmental exposures
•Frequently presents at advanced stage
•Close proximity to orbit and cranial structures
carcinoma of the maxillary sinus management and prognosis
• Requires combined surgical and oncologic therapy
• Radiation therapy commonly included in treatment
• Prognosis depends on stage at diagnosis
•Often poor due to delayed detection
Requires multidisciplinary management approach
oral manifestations of systemic disease
medical history includes a full review of systems
ROS surveys major body systems and functions
oral findings may signal undiagnosed disease
some oral signs are specific, others non specific
recognition guides care and medical referral
endocrine system
glands secrete hormones into blood stream
hormones then regulate growth, metabolism, function
target organs respond via specific receptors
negative feedback controls hormone levels tightly
disorders reflect hypo- or hypertension states
pituitary gland overview
has anterior and posterior lobes
• Anterior lobe secretes multiple regulatory hormones
•Hormones include GH, ACTH, TSH, FSH, and LH
•Pituitary hormones regulate multiple target organs
•Not all disorders show oral findings clinically
pituitary hormones
regulate multiple target organs
GH, ACTH, TSH, FSH, and LH
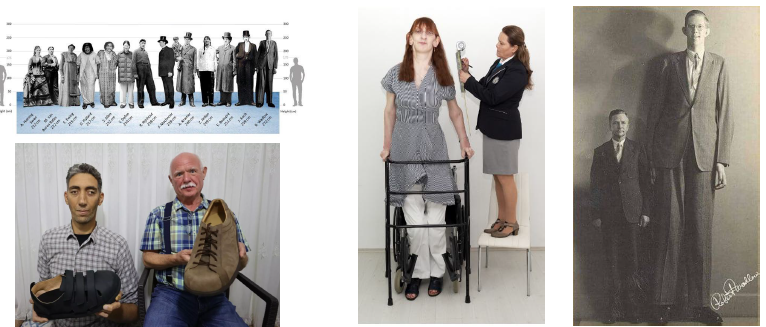
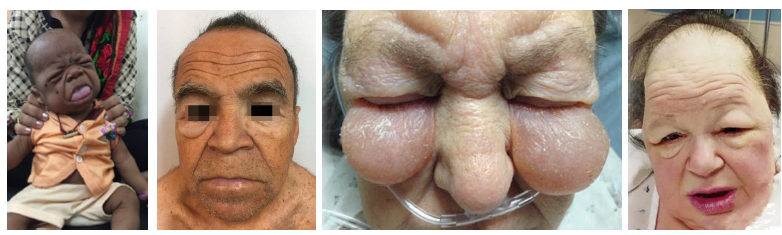
giantism clinical and radiographic features
GH excess in childhood before epiphyseal closure
marked with extreme height, long limbs, and large hands
disproportionate body growth and skeletal size
jaws enlarges with generalized macrodontia
oral structures with normal in form but enlarged
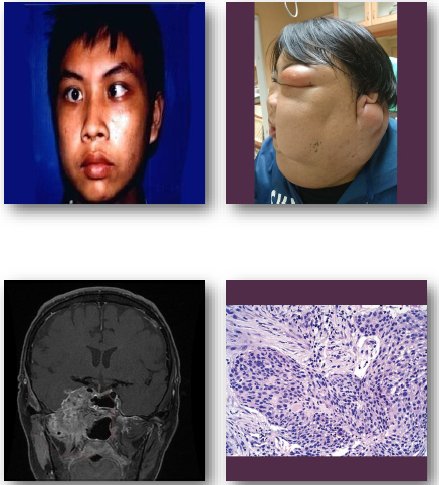
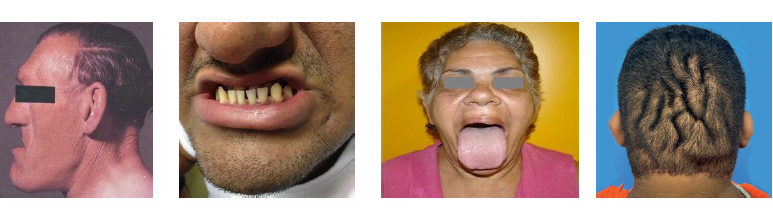
acromegaly clinical and radiographic features
GH excess after closure of epiphyseal plates
enlargement of hands, feet, and facial bones
mandibular prognathism with coarse features
macroglossia with spacing of normal teeth
associated systemic disease risk increased
hypopituitarism overview and etiology
reduced production of one or more pituitary hormones
often involves hypothalamus or anterior pituitary
GH deficiency leads to pituitary dwarfism state
may reflect hormone deficiency or tissue resistance
effects depend on specific hormone deficiency

hypopituitarism clinical and radiographic features
short stature with normal body proportions present
facial structures proportionate but small than normal
maxilla and mandible reduced in overall size
teeth small with delayed eruption patterns
retention of primary teeth may be observed

hypopituitarism management and prognosis
diagnosis based on delayed growth and development
hormone testing confirms specific deficiencies
growth hormone therapy used before plate closure
early treatment improved growth and outcomes
systemic complications depend on underlying cause

non-achondroplastic short stature: overview
•Proportionate short stature due to endocrine causes
•GH deficiency leads to pituitary dwarfism state
•Hypothyroidism causes growth and development delay
•Genetic syndromes produce varied growth patterns
•Chronic disease may impair normal growth
thyroid gland
•Thyroid gland lies anterior to the larynx in neck
•Butterfly shape with two lobes and central isthmus
•Secretes T3 and T4 regulating metabolism rate
•Controlled by TSH from anterior pituitary gland
•Disorders reflect hypo-or hyperthyroid states
hyperthyroidism (graves disease) overview
•Excess T3 and T4 cause hypermetabolic state
•Often due to autoimmune Graves disease process
•Autoantibodies stimulate thyroid continuously
•Leads to thyrotoxicosis with systemic effects
•Most common in women age 20 to 40 years

hyperthyroidism (graves disease) clinical features
•Heat intolerance, sweating, anxiety, tremor
•Weight loss despite increased appetite present
•Tachycardia, hypertension, cardiac strain risk
•Exophthalmos with protruding eyes characteristic
•Oral burning, caries, perio risk increased

hyperthyroidism (graves) management and diagnosis
•Diagnosis confirmed with labs and iodine uptake
•Beta blockers used to control systemic symptoms
•Monitor for thyroid storm in untreated patients
•Short low stress appointments recommended
•Avoid epinephrine in uncontrolled cases

hypothyroidism overview and etiology
•Deficiency of thyroid hormones T3 and T4 present
•Most commonly due to Hashimoto thyroiditis
•Autoimmune destruction leads to gland failure
•More common in females age 45 to 65 years
•Associated with other autoimmune disorders
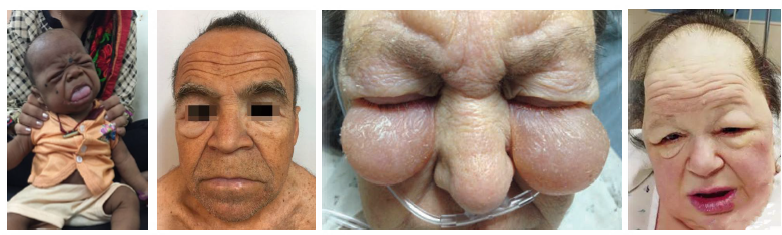
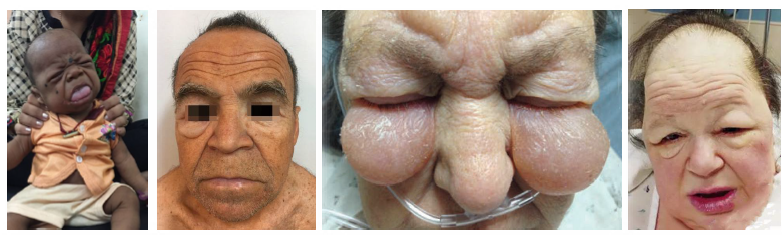
hypothyroidism clinical and radiographic features
Fatigue, weight gain, cold intolerance common
•Bradycardia, slowed metabolism, mental slowing
•Macroglossia with thick lips and facial features
•Delayed eruption and jaw osteoporosis noted
•Xerostomia and oral changes may be present
hypothyroidism management and prognosis
•Diagnosis confirmed by thyroid hormone levels
•Managed with synthetic thyroid hormone therapy
•Early treatment prevents severe complications
•Monitor for delayed healing and xerostomia
•Dental care modified based on disease control
parathyroid glands
• glands located adjacent to thyroid lobes
•Secrete PTH regulating serum calcium levels
•PTH mobilizes calcium from bone stores
•Increases intestinal absorption and renal retention
•Disorders reflect increased or decreased PTH levels
hyperparathyroidism overview
excess PTH increases serum calcium levels
primary due to tumor or gland hyperplasia
secondary due to chronic hypocalcemia states
renal failure common cause of secondary type
leads to bone resorption and systemic effects
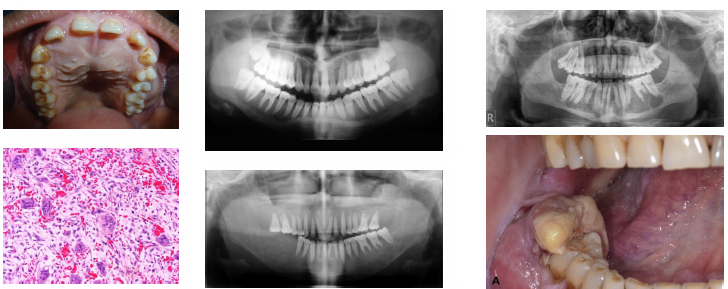
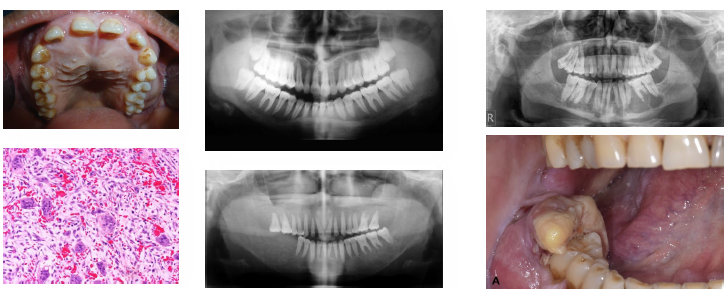
hyperparathyroidism clinical radiographic features
•"Stones bones groans" classic symptom pattern
•Renal stones due to hypercalcemia levels
•Ground glass bone with lamina dura loss
•Brown tumors cause jaw radiolucencies
•Bone and root resorption may be evident
hyperparathyroidism management
•Diagnosis shows elevated PTH and calcium levels
•Primary treated with surgical gland removal
•Secondary managed by correcting hypocalcemia
•Vitamin D and diet used in renal patients
•Dental findings may prompt initial diagnosis