Medications
1/26
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
27 Terms
What are the Mode of Action, Hypoglycaemia Risk, Dosing, Side Effects, Counselling, Renal Impairment, Hepatic Impairment, Weight Effect for Metformin ?
Medication Group & Drug | Mode of Action | Hypoglycaemia Risk | Dosing | Side Effects | Counselling | Renal Impairment | Hepatic Impairment | Weight Effect |
Metformin (Biguanide) | ↓ gluconeogenesis so ↓ hepatic glucose production; ↑ peripheral glucose uptake in muscle and adipose; decreases intestinal glucose absorption | Low | 500–1000 mg 1–2× daily; max 2 g/day | GI upset, diarrhoea, B12 deficiency, lactic acidosis (rare) | Take with food; GI effects settle; report fatigue (possible B12 issue) | Reduce dose if eGFR <45; avoid <30 | Caution due to lactic acidosis risk | Neutral / slight loss |
Why is metformin useful in early T2DM?
It works even when β‑cell function is reduced.
What additional metabolic benefits does metformin have?
Improves lipid profile (↓ triglycerides, ↓ LDL)
What conditions other than T2DM can metformin be used for?
Prediabetes, gestational diabetes, PCOS, NA fatty liver disease.
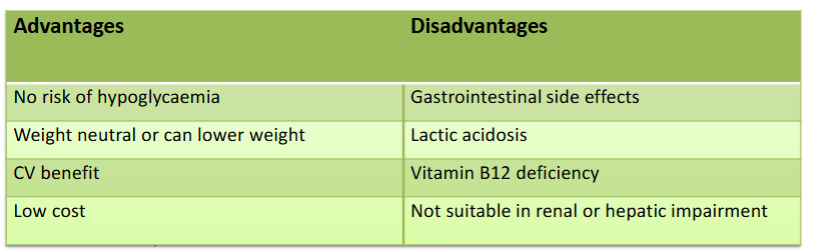
What are the advantages and disadvantages of metformin?
Doesn’t stimulate pancreatic insulin secretion → beneficial when beta cell function is already reduced
What are the Mode of Action, Hypoglycaemia Risk, Dosing, Side Effects, Counselling, Renal Impairment, Hepatic Impairment, Weight Effect for Sulfonylureas?
Medication Group & Drug | Mode of Action | Hypoglycaemia Risk | Dosing | Side Effects | Counselling | Renal Impairment | Hepatic Impairment | Weight Effect |
Sulfonylureas (e.g., Gliclazide) | Stimulate pancreatic insulin secretion | High | Once or twice daily | Hypoglycaemia, weight gain | Eat regularly; recognise/treat hypos; avoid skipping meals | Dose reduction often needed | Caution | Gain |
What is the main risk of using Sulfonylureas?
Hypoglycaemia
What are the Mode of Action, Hypoglycaemia Risk, Dosing, Side Effects, Counselling, Renal Impairment, Hepatic Impairment, Weight Effect for DPP‑4 inhibitors?
Medication Group & Drug | Mode of Action | Hypoglycaemia Risk | Dosing | Side Effects | Counselling | Renal Impairment | Hepatic Impairment | Weight Effect |
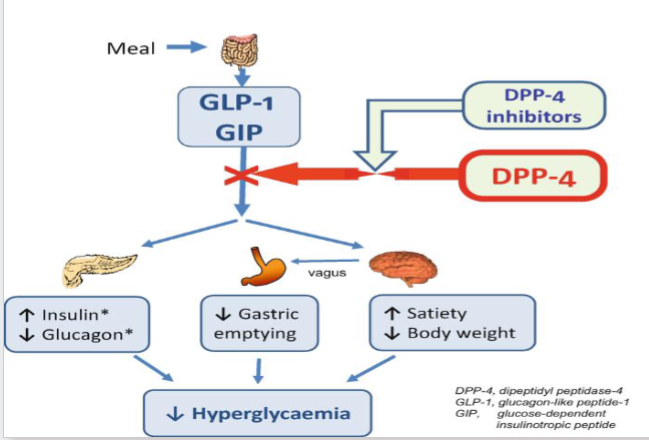
DPP‑4 inhibitors (e.g., Sitagliptin) | Prevents breakdown of GLP-1, ↑ incretin, ↑ insulin, ↓ glucagon | Low | Once daily | Headache, nasopharyngitis, pancreatitis (rare) | Report severe abdominal pain | Dose reduction for most except Linagliptin | Generally safe; caution in severe disease | Neutral |
What are the advantages and disadvantages of DPP‑4 inhibitors?
Weight‑neutral and low hypoglycaemia risk.
What are the Mode of Action, Hypoglycaemia Risk, Dosing, Side Effects, Counselling, Renal Impairment, Hepatic Impairment, Weight Effect for SGLT2 inhibitors?
Medication Group & Drug | Mode of Action | GLP‑1 RAs (e.g., Semaglutide) | Mimic incretin; slow gastric emptying | Low (unless with insulin/SU) | Weekly or daily injection | Nausea, vomiting, diarrhoea, pancreatitis (rare) | Smaller meals; nausea improves; report abdominal pain | Usually no adjustment; caution if severe | Limited data; caution | Significant loss |
Na glucose co-transporter 2 inhibitors (e.g., Empagliflozin, dapagliflozin) | In the PCT it ↑ urinary glucose excretion, decreases plasma glucose control | Low | Once daily T2DM | Genital infections, UTIs, dehydration, DKA (rare) | Hydration; genital hygiene; stop during acute illness | Reduced efficacy at low eGFR; avoid if too low | Generally safe; caution in severe disease | Loss |
What are the advantages and disadvantages of SGLT2-inhibitors?
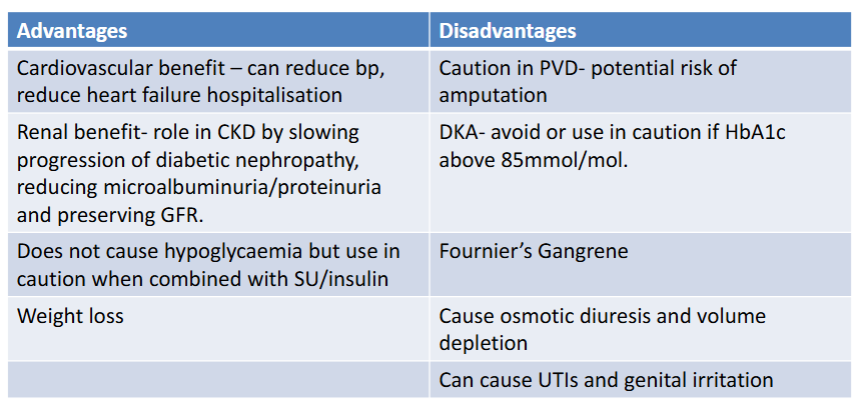
How can GFR levels affect SGLT2 effectiveness?
If GFR < 45 there might be renal impairment glycaemic effects. Should continue to help glucose control
What counselling tips are given to patients on SGLT2?
Sick day rules as can increase risk of DKA
If ill with diarrhoea, vomiting, fever, dehydration then STOP
Restart 24hrs after feeling better.
Keep hydrated by drinking lots of water/fluid
Stop sglt2 prior to any planned surgery
Avoid eating very low carb diet/ketogenic diet increased risk of ketosis
What are the Mode of Action, Hypoglycaemia Risk, Dosing, Side Effects, Counselling, Renal Impairment, Hepatic Impairment, Weight Effect for GLP-1 RAs?
Medication Group & Drug | Mode of Action | Hypoglycaemia Risk | Dosing | Side Effects | Counselling | Renal Impairment | Hepatic Impairment | Weight Effect |
GLP‑1 RAs (e.g., Semaglutide) | Increases insulin secretion, decreases glucagon and gastric emptying | Low (unless with insulin/SU) | Weekly or daily injection | Nausea, vomiting, diarrhoea, pancreatitis (rare) | Smaller meals; nausea improves; report abdominal pain | Usually no adjustment; caution if severe | Limited data; caution | Significant loss |
What are the advantages and disadvantages of GLP-1 receptor agonists?
What are the Mode of Action, Hypoglycaemia Risk, Dosing, Side Effects, Counselling, Renal Impairment, Hepatic Impairment, Weight Effect for insulin? T1DM
Medication Group & Drug | Mode of Action | Hypoglycaemia Risk | Dosing | Side Effects | Counselling | Renal Impairment | Hepatic Impairment | Weight Effect |
Replaces/supplements endogenous insulin | High | Individualised; basal/bolus regimens | Hypoglycaemia, weight gain, injection‑site reactions | Hypo recognition; rotate sites; monitor glucose | Lower requirements as renal function declines | May need adjustment | Replaces/supplements endogenous insulin | High |
When might insulin be needed in T2DM?
Severe hyperglycaemia
Catabolic symptoms
Failure of oral therapy
Acute illness or surgery
How do meglitinides work and when are they used?
Repaglinide
Stimulate beta cells for rapid, short‑acting insulin release.
To control post‑prandial glucose spikes
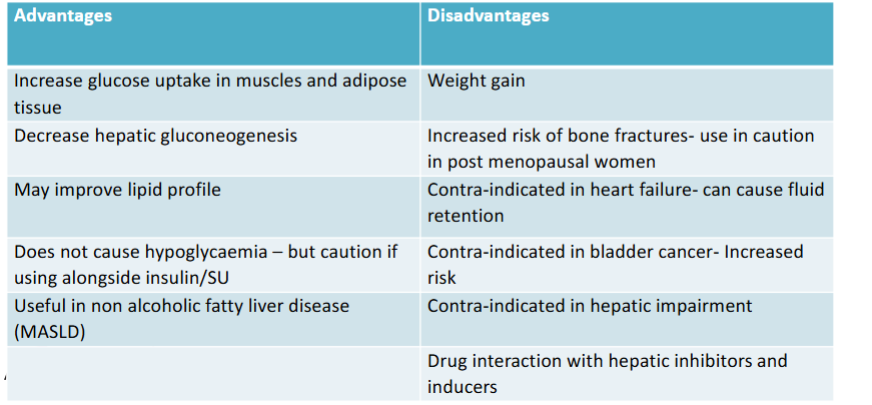
What is the mechanism of Tiazolidinediones and a key ADR?
Pioglitazone
Peroxisome Proliferator-Activated Receptor gamma agonists
Increase insulin sensitivity in muscle, liver, and adipose tissue.
Fluid retention → risk of heart failure
What are the advantages and disadvantages of Tiazolidinediones?
What are alpha-glucosidase inhibitors?
Acarbose
Very rarely used
Inhibit intestinal alpha-glucosidase in the small intestine.
Delays breakdown of carbohydrate leading to a slower absorption of glucose.
Beneficial in reducing post prandial spikes
Can cause GI side effects
Contra-indicated in IBD
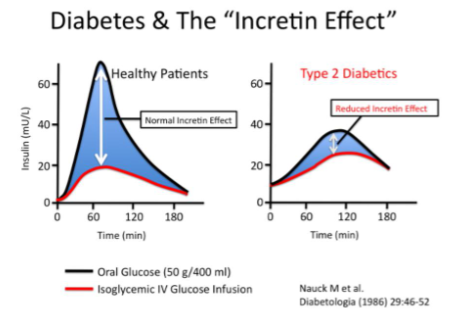
What is the incretin effect?
Where oral glucose intake produces a greater insulin response than the same amount of glucose given intravenously, even when blood glucose levels are similar, due to gut hormones.
Incretin hormone peptides released from the GI tract after food has been ingested.
These peptides stimulate additional insulin release beyond pancreatic beta cells
In type 2 diabetes this ‘incretin effect’ is reduced
What are the main incretin hormones?
GLP-1
Glucagon dependent insulinotropic polypeptide
GLP agnonists
Resisntant to degradation by DPP4 enzymes that inactivate incretins
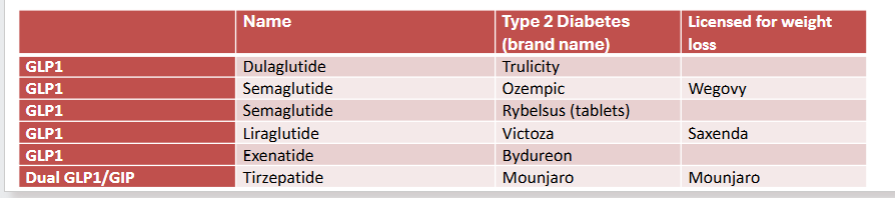
How are GLP1s given?
Subcutaneous injection or oral tablets (semaglutide only). Weekly or daily injection
Not substitute for insulin. Contra-indicated type 1 diabetes
Severe and persistent abdominal pain with or without vomiting can be a sign of acute pancreatitis - should be stopped.
Risk of hypoglycaemia if given alongside insulin and/or SU- monitor closely
Due to delay in gastric emptying/absorption then can interact with some oral medications
Extra precaution required with contraception and adjustment of HRT when starting GLP therapy and
for 4 weeks at every dose change.Counselling on missed doses for weekly injections, must have at least 4 day interval between each
dose
Counselling tips for women on contraception or HRTs
Incretin based therapy (GLP1 and GIP), delay gastric emptying and may reduce the absorption of any oral form of contraception and HRT.
FSRH guideline for GLP therapy and contraception:
All women taking GLP should use contraception
Those taking tirzepatide (Mounjaro) should switch to a non-oral method or add a barrier method for 4 weeks after initiation and 4 weeks after each dose increase.
If possible, transfer to transdermal form of delivery
If not possible double dose of progesterone for 4 week on initiation and every dose increase for 4 weeks
Types of GLP1 drugs