Motor Speech Final Slides pt 1 - Stuttering/Cluttering
1/179
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
180 Terms
Fluency
multidimensional construct that is based on observable actions (speech articulation) and underlying neural processing (pre linguistic conceptualization, formulation, motor planning)
Fluency depends on both the language and speech motor processes.
Important to have clear conceptualization of fluency in order to work with individuals who have a fluency impd.
Need to know normal in order to know abnormal
7 Dimensions of Fluency
Continuity
Rate
Rhythm
Effort
Naturalness
Talkativeness
Stability
Different Types of Fluency
Speech Fluency
Semantic Fluency
Syntactic Fluency
Pragmatic Fluency
Breakdown in speech fluency is termed disfluencies.
Linguistic Fluency - refers to effortless and proficiency in which a speaker selects and assembles the linguistic codes, knowledge of vocab, syntax, phoneme, morphemes
Need to know the source of the dysfluency
Any speaker can be more or less fluent dependent on
Demands of the communication situation
The psychophysical state of the person
Social/cultural norms
Communication proficiency
Topic knowledge and cognitive or linguistic demands
Age and status of speech and language development
Self-regard and Self-belief systems
Normal Disfluencies
Hesitations (pauses for language formulation)
Word fillers ("like") or interjections ("um")
Phrase repetition (more than 1 word repeated)
Whole word repetitions (2 or less)
Revisions (change how we say a message)
Fluency Disorder
Classified as a subtype of speech disorder, also includes difficulties in language formulation. Manifested in speech in the form of pauses, hesitations, word repetitions.
Two common speech fluency disorders; Stuttering and Cluttering
Atypical Disfluencies Core and Secondary Behaviors
Part-word (sound/syllable) repetitions, Single syllable whole word repetitions (>2), Prolongations & Blocks
Avoidance, Postponement, Starters, Disguise/Conceal, Interrupter Devices, & Searching Movements /Escape behaviors
General Stuttering Guidelines
Normal Disfluency: 1.5 - 6years
Borderline Stuttering: 1.5 - 3.5years
Beginning Stuttering: 3.5 - 6 years
Intermediate Stuttering: 6 – 13years
Advanced Stuttering: 14+ years
Normal Disfluency
1.5-6 years
Core Behaviors
No more than 10 disfluencies per 100 words
Typically one to two unit repetitions
Mostly repetitions, interjections, & revisions
Borderline Stuttering
1.5-3.5 years
Core Behaviors
11 or more disfluencies / 100 words
Often more than 2 unit repetitions
More repetitions and prolongations than revisions
Loose, relaxed disfluencies
Contributing Factors for Typical Disfluency and Borderline Dysfluency
Demands of language Acquistion
Speech motor control maturation
Family stresses
Threats to security (death in the family, divorce, moving, birth of sibling etc)
Beginning Stuttering
3.5-6 years
Core Behaviors
Emergence of tensing and speeding up of repetitions
Stuttering occurs more often in frequency
Pitch rise accompanies prolongations
Fixed articulatory postures may appear in blocks
Secondary Behaviors
Escape behaviors are present (eye blinks, head jerks) as disfluency progresses
Feelings and Attitudes
Awareness of difficulty and feelings of frustration are present
Contributing Factors
Interplay of constitutional (predispositions)and environmental factors
Child's own temperament
Conditioned reactions causing excess tension and escape behaviors
Intermediate Stuttering
6-13 years
Core Behaviors
Blocks in which sound and airflow are cut off
Increasingly tense blocks, repetitions and prolongations
Secondary Behaviors
Escape behaviors
The emergence of avoidance and disguise behaviors
Feelings and Attitudes
Fear of stuttering emerges
Embarrassment and shame
More tense blocks are met with increased listener surprise or impatience
Fear of listener reactions/punishment increases
Contributing Factors
All previously described, plus
Avoidance conditioning
Fear before stuttering, embarrassment during stuttering, and shame after stuttering contribute to more negative experiences and feelings.
Advanced Stuttering
14 plus years
Core Behaviors
Long tense blocks, some with tremor (involuntary muscle movements due to tension)
Highly over learned patterns
more difficult to change
Also see tense repetitions and prolongations
Secondary Behaviors
Escape and avoidance behaviors can become more complex
Feelings and Attitudes
Negative self-concept begins to be formed
Contributing Factors
All previously described
Cognitive learning
Most common type of stuttering Is…
neurodevelopmental stuttering also labeled as childhood stuttering, developmental stuttering
Onset in childhood
Most often occurs in pre-k years, absence of a neurological injury, trauma, illness
American Psychiatric Association (2013) adopted "Childhood Onset Fluency Disorder" as part of DSM-5 (Diagnostic and Statistical Manual of Mental Disorders)
WHO (2018) used the label "Developmental Speech Fluency Disorder" when referring to stuttering, classified under broader heading “Neurodevelopmental disorder”
Childhood form stuttering is different from non-developmental form of stuttering also referred to “acquired stuttering” ▪ Neurogenic, pharmacogenic, psychogenic
Possible predictors/factors
Family History
Gender
Age at Onset
Stuttering Severity and Frequency
Duration Since Onset
Duration of Stuttering Moments
Presence of sound prolongations and blocks
Phonological Skill
What causes stuttering?
Physiological
Linguistic
Emotional
Environmental
Multifactorial Framework
Predisposing physiological and linguistic factors may be significant in the onset and development of stuttering.
These predisposing factors interact with emotional and environmental aspects and contribute to severity, persistence and impact on child and family
What are the physiological considerations? Constitutional Makeup
Hereditary Factors
Idea of stuttering is inherited recognized since 1935 by Bryngelson
Studies suggest stuttering usually runs in families;
80% (Yairi, '05, Kidd '84)
66% according to JSHD '91 •
Know family hx is important •
There is a high concordance (60-70%) of stuttering in identical twins compared to fraternal (Andrews et al 1991)
Genetic Link
Mutations of genes in chromosome 12 and 18
Linked 5 genes to stuttering
Congenital/Trauma Studies
Study done by West, Nelson and Berry (1939) - 85/100 no family hx however reported congenital factors (infectious disease, diseases of nervous system, injuries)
Poulos and Webster, 1991 – 57/169 no family hx. 37% of those reported a significant childhood event (anoxia at birth, premature birth, head injury, experiencing intense fear.)
Brain Structure Differences in PWS
Both old and new studies have shown that some individuals who stutter have greater activity in R frontal hemisphere vs L (reversed in typically fluent speakers)
1970s/1980s used EEG to look at cerebral blood flow (CBF)
1995 studies looked at CBF utilizing PET confirming above findings
2 explanations for overactivation of R hemisphere
R side become "wired" for speech vs left during embryonic development
Child initially tries to use inadequate L hemisphere, neural networks fail and its only then they activate the R side
Overactivation in Midbrain - found some structures of the basal ganglia show to be overactive
Underactivity in Speech Motor Areas
Underactivity in Auditory Areas - lack of activity in superior temporal lobe and auditory association areas and Wernickes areas
Whole brain connectivity deficits – deficits found in neural connections involving attention, motor performance, perception and emotion
Structural deficits in L hemisphere that may be involved with programming speech movt's
Brain Function Differences: Neurochemical Link
There is an excess of the neurotransmitter Dopamine
Dopamine antagonist medications have been effective in the treatment of stuttering ex: risperidone
3 Main influences
Genetics, Abnormal development of basal ganglia and/or white matter tracts, & Autoimmune Component (PANDAS)
Sensorimotor Factors
Research has shown areas of the auditory cortex are under activated during stuttering
PWS have deficits in perceiving speech and other sounds under conditions that stress auditory perceptual processing
Reaction Time – PWS have slower reaction time with initiaing and terminating a vowel sound in response to a target, activating respiratory and articulatory movts, slower to respond to auditory and visual signals
Nonspeech Motor Control
Research examining if stuttering is the result of general motor timing/coordination problem rather than a problem limited to speech production
Studies have revealed PWS demonstrate increase difficulty with nonspeech tasks such as sequential finger tapping
Results suggest PWS may have difficultly with response planning, organization and initiation of novel sequences of movement
SPEECH AND LANGUAGE DEVELOPMENTAL FACTORS
Children’s learning of phonology, morphology, syntax and semantics may strain resources resulting in decrease fluency.
CWS demonstrate an increase in language deficits or "dissociations" among language components compared to their fluent peers
SPEECH AND LANGUAGE DEVELOPMENT
CWS exhibit more articulation errors or phonological processes than do their normally fluency peers
30%-40 concurrence
These children were found to be at risk for stuttering to persist
Language Factors
Smith & Webster (2017): Reviewed multiple studies
Many individual differences in language ability and performance
Complex interactions between language and speech skills, developing rapidly during childhood.
Increase risk for stuttering in bilingual individuals (Howell & Van Borsel 2011) - may demonstrate the strain on language resources
EMOTIONAL FACTORS – ANXIETY & AROUSAL
Research show cognitive stress increases the number of disfluencies in PWS
Bosshardt (2006) proposed that emotion can be one of the brains activities that create interference in the speech and language planning and production systems
Anxiety
Specific relationship between anxiety and stuttering remains unclear
Coping skills can result in greater self acceptance and satisfaction with life for PWS
TEMPERAMENT
CWS score higher on tests that measure the following personality traits
Sensitive temperament
Slower to adapt, high frustration, lack of persistence
More emotionally reactive and less able to regulate emotional responses
Perfectionism
DEVELOPMENTAL FACTORS
Evidence for developmental factors = most onset of stuttering occurs when children are developing most rapidly during their preschool years
Competition for neural resources / Neurological maturation
Language learning and onset of stuttering
Cognitive development – learning to think, remember, problem solve and plan may make demands on neural resources
Environmental Factors
Evidence for environmental factors = higher incidence of stuttering during particular stresses
Higher incidence of stuttering in more competitive cultures
Parents – (Yairi 1997) suggested some CWS grew up with parents who were more demanding and anxious which may have had an impact
Environmental Pressures:
Competing for talk time
Loss of listener attention
Listener impatience
Frequent interruptions
Hurried when speaking
Excited when speaking
Many things to say
Frequent questions (not well supported)
Stressful Life Events
Physical/Emotional Trauma
Moving
Birth of new sibling
Parents separate or divorce
Family member is hospitalized or dies
Parents travel away from home often (one or both)
Holidays which cause change in routine, excitement or anxiety
Comorbidities
Common comorbidities in CWS:
Developmental delay
Reading difficulties
ADD/ADHD
Behavioral Disorders
Diabetes
Asthma
Sickle Cell Anemia
Classical Conditioning (CC)
Learning caused by the association of a neutral stimulus that strongly provokes a response. The conditioning process will cause the formerly neutral stimulus to eventually provoke the response
Operant Conditioning
Learning caused when a behavior is immediately followed by a reward or punishment or the relief of punishment
Initial Conditioned Stimulus
stuttering disfluencies elicit negative reactions which triggers a response to stop them = CR (may play a role in physical tension)
Spread of Conditioning
Several other stimuli are present during the initial CR which may cause disfluencies in other environments
Operant Conditioning and Stuttering
Stuttering behaviors seen in adults who stutter result from a combo of classical and operant learning
Many have viewed stuttering as an avoidance reaction to being punished for normal disfluencies
Unlearning Stuttering(?)
Ages 2-3.5: prevent the CS from eliciting negative emotion resulting in muscle tension
Done by changes in family environment, boosts child's natual fluency, reverse bad feelings, family acceptance
Ages 3.5-6: implement more structured practice and rewards/praise
Ages 6-12: treatment target to elicit the CS and make sure it is NOT followed by the CR (defensive or negative reaction)
Adults and adolescents: Can provide more direct therapy, educating the individual that negative feelings and anticipatory fears are fueling their stuttering
Constitutional Theories
Anomalies of Brain Organization
Disorder of Timing
Reduced Capacity for Internal Modeling
Language Production Deficit
Includes Covert Repair Hypothesis
Multifactorial Dynamic Disorder
Stuttering develops as a result of a Timing Disorder
Van Riper (1982): disruption of timing of muscle sequencing = stuttering
Kent (1994): deficit in central timing that regulates speech production and integrates left-brain segmental and right brain supra-segmental aspects of speech production
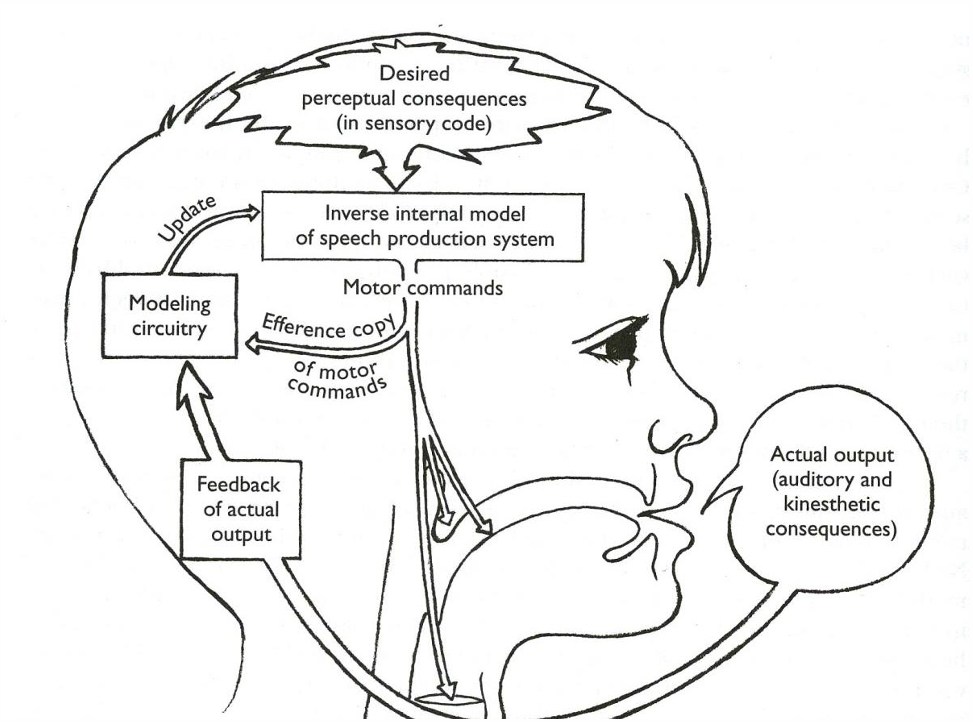
Stuttering develops as a result of a Reduced Capacity for Internal Modeling
Children learn to talk by hearing the sounds of their language and developing a “model” of how to move their articulators to make the sounds they just heard
Then they use auditory feedback as they babble and talk to update their internal model as their speech mechanism matures as they grow
Stuttering is thought to result from a weakness in using the internal model to transform the child’s plans for the sounds of a word into motor commands leading to speech movts
Stuttering as Reduced Capacity for Internal modeling
Only attempts to account for core behaviors
Explains why decrease rate of speech can result in increased fluency
Stuttering develops as a result of a Language Production Deficit
Wingate (1988); Perkins, Kent, and Curlee (1991); and Kolk and Postma (1997) suggested stuttering results from deficits in planning and assembling the units for language production
Language production is monitored internally
If problem in phoneme plan is in error, production halts
Repetitions, prolongations, and blocks can all be explained by different responses to an error
Kolk & Postma's Covert Repair Hypothesis
Disfluencies arise bc speakers attempt to repair internally before starting to speak.
PWS are particularly disfluent bc their phonological encoding abilities are impaired.
They make (and covertly repair) many phonological encoding error
Repetitions = repairs at end of word
Prolongations = repairs in middle of word
Blocks = repairs in beginning of word
Analogy
Analogy to putting together the components of language production
Quality control inside the shop = internal monitoring
Quality control outside = auditory feedback
If internal model detects an error in phonetic planning, results in halting of speech (same as if there was a problem in the bike, halts production)
Stuttering results if internal checkpoint detects error, and speaker retries, prolongs, or pushes ahead despite error
hypothesis of a language production deficits in stuttering Physcolinguistic Approach
A dyssynchrony between 2 components of language production ◦ paralinguistic (right side) ◦ linguistic (left side) resulting in disfluencies
Proposes the difference between normal disfluencies and stuttering is that PWS feel pressure to continue to speak even if the dyssynchrony is detected (push forward) as well as a sense of loss of control (decrease awareness)
Stuttering develops as a result of a Multifactorial Dynamic Disorder
Smith –believes stuttering is mainly caused by a motor speech disorder that is then influenced by cognitive, linguistic and psychosocial factors.
Viewed as “dynamic” bcthe disfluencies are the outward manifestations of an underlying, ever changing inner situation
Multifactorial Dynamic Disorder
suggest there is no one cause of stuttering, but an array of factors contributing to it
The problem is to find the relevant factors and discover how they interact
Diagnosogenic Theory
Johnson thought stuttering is cause by children who were misdiagnosed by their parents or other listeners when demonstrating typical disfluencies which resulted in tension/avoidance and then increase hesitation
Johnsons stated: "The problem is not with the child's mouth but in the parent's ears.“
Widely accepted theory throughout 1940s/50s
Pinpointed environmental factors as the sole cause of stuttering, blame parent's negative reactions
Communication Failure and Anticipatory Struggle
Oliver Bloodstein(1987; 1997) proposed that in many cases, stuttering begins when a child finds talking difficult, experiencing frustration and failure
Anticipated difficulty in talking produces tension resulting in fragmented speech
This leads to more frustration and failure in communication, which increases anticipation of difficulty
Capacities and Demands View
Stuttering may emerge when child’s capacities for fluency are overwhelmed by demands
Examples
Capacities : Child’s ability to plan and program for language while making fast, coordinated movements for speech ◦
Demands : Some children’s advanced conceptual and linguistic abilities; models of rapid and complex speech and language in environment; emotional stress on child from environment
treatment based on reducing demands and, when possible, increasing capacities
Joseph Sheehan
"A child's who has begun to stutter is probably a child who has too many demands placed on him while receiving too little support." ◦
Believed stuttering is a result of learned behavior
Viewed stuttering as the result of a conflict between opposing drives to speak (approach) and to hold back from speaking (avoidance).
“Don’t avoid, don’t’ hide, don’t deny your stuttering. The only way you’ll ever get over your fear of stuttering and thus become genuinely fluent; is to meet it head-on. Always do the thing you fear, and gradually you will learn not to fear it.”
Integrated Perspective
Two Stage Model of Stuttering-Stuttering may often develop in two stages
Primary stage is simpler disfluencies that are the result of how the brain handles speech and language production
Secondary stage is a more complex pattern that is the result of the child’s and environment’s reaction to disfluencies
First Stage Primary Stuttering
Based on PWS have differences in the way their brains process sensory information and produce motor output (auditory motor processing)
Caused by a genetic inheritance or early brain damage
How does this inefficiency lead to Primary Stuttering?
Many existing theories suggest dyssynchrony, at some level, is responsible for repetitions, prolongations, or blocks
Therefore Primary stuttering may be the result of a decrease in organization of speech and language networks in the brain, which can resolve via maturation or reorganization
Perspectives on Secondary Stuttering
Instead of saying the secondary behaviors observed are a result of the core behaviors, Guitar believes a child's temperament and "in the moment" responses and interaction with learning can result in secondary behaviors.
These reactions may constitute the components of secondary stuttering (i.e., increased tension, escape, and avoidance)
Because a reactive temperament causes emotional arousal, events that caused the emotion will be more deeply learned (learning is enhanced by emotion)
Children who react to primary stuttering with increased tension, escape, and avoidance behaviors will be more likely to continue these secondary behaviors long term
Behaviors associated with high emotion are likely to be retained permanently
Therefore, treatment of those with secondary stuttering may be most effective if coping skills are taught, e.g. gentle onsets, slow rate, light contacts
Possibly two predispositions for Stuttering?
Primary and secondary stuttering may have two predispositions.
Primary most common: stuttering that is resolved through neural maturation and reorganization
Secondary : a predisposition for a reactive temperament
How's Child's Development interact with Two Predispositions – 3 ways
1. Interaction with speech and language development ◦ Child with primary stuttering may be able to recover if speech and language demands are low or language ability is strong
Another child with primary stuttering may not recover so easily if language development demands are high or child is not strong in speech and language
2. Interaction with brain maturation
Some individuals will recover early because they have greater neural plasticity
Females appear to have greater organizational plasticity and more widely distributed language centers
3. Interactions with social-emotional development
As social-emotional development creates stress on children, those with higher temperaments may be more likely to have more negative reactions to difficulty with speech
Interactions with Environmental Factors
Primary Stuttering
An environment that is slow-paced and accepting may be more likely to give children freedom to develop fluency at their own pace
An environment that is fast-paced and demanding may be more likely to delay recovery
Secondary Stuttering
•Families can help reactive child develop skills to manage stress, thus decreasing likelihood of stuttering becoming persistent
Some life events (e.g., divorce, hospitalization) can increase vulnerable children’s reactivity, thus increasing likelihood of stuttering becoming persistent
Treatment Pre-K
Lots of modeling, slower speaking rate (including pauses)
Reduce environmental stresses/pressure
Goal is to avoid negative reaction – work with caregivers on accepting the repetitions
Treatment - School Age
Assess the amount of tension present
Assess escape/avoidance behaviors
If present, reduce fear
Practice fluent speech to develop confidence (great focus if secondary behaviors are not present)
Treatment - Adolescents and Adults
Need to first work on diminishing their defensive reactions that trigger tension and secondary behaviors.
Need to bring awareness of the learned behaviors
Need to reinforce most listeners are patient not rejecting
Acceptance is key here! Building a trust is key
Client Needs
Need to try to look at each client with fresh eyes
• Don't make promises
• Can't resolve things in 1 session
• Need to know client's goals
• Need to know how the client views their stuttering
• how they want to talk about it/phrasing
• Need to build rapport/trust with client and family
Insurance Considerations & Privacy Rights
Clients need to look into what services are covered by their insurance (unfortunately, may impact your treatment)
Need to know HIPAA Laws
Need to know what circumstances require you to break confidentiality
Assessing Stuttering Behavior
Mode of measurement needs to be reliable: Intra-raterreliabiltyand Inter-rater reliability \
Speech samples –good idea to get one in tx, one in home environment. Want it to be around 300 syllables of conversational speech, 200 syllable for reading sample
Frequency –how often does the individual stutter in speech/reading. Provides info on stuttering level
Types of disfluencies
Duration –longer stuttering are worse then shorter ones
Looking at secondary behaviors
Assessing Severity: SSI-4 most commonly used
Stuttering Severity Instrument (SSI-4)
Assessing surface/overt features:
More than one sample of spontaneous speech
Overall score is based on sum of 3 components:
% syllables stuttered in readingand conversation
Duration of 3 longest blocks (Mean duration)
Physical Behaviors
Standardized severity rating for children and adults
Assessing Severity
Test of Childhood Stuttering (TOCS)
Scale of Rating Severity of Stuttering (less reliable)
Lidcombe Program's Severity Rating Scale (good to use outside of treatment)
Speaking and Reading Rate –can be calculated by counting syllables or words per minute. Also part of SSI-4
Fluency Bank
Stuttering Prediction Instrument ages 3-8
Assessing Feelings: Pre-k age
The KiddyCAT consists of 12 yes/no questions. Only use if the client is aware of their stuttering
The Impact of Stuttering on Preschoolers and Parents Survey–20 questions, used to determine if treatment is appropriate (example figure 8.6)
The Behavioral Style Questionnaire –used to assess temperament
Short Behavioral Inhibition Scale –7 point scale to measure sensitive temperament via parent report
Assessing Feelings: School Age
A-19 Scale: Needs further research but good tool to start a discussion
Communication Attitude Test: well researched for reliability, can determine negative feelings for children 6 and older
Overall Assessment of the Speaker's Experience of Stuttering (OASES): assess impact stuttering has on the client's day to day life, helpful for treatment planning
Teacher's Assessment of Student Communicative Competence (TASCC):Questionnaire filled out by teachers to reflect students' communication in classroom
Assessing Feelings: Adolescents and Adults
Attitudes (S-24): Reliable questionnaire that can be completed for testing and re-testing attitudes
Stutterer's Self-Rating of Reactions to Speech Situations (SSRSS): Questionnaire that assesses frequency of stuttering during various situations
Perceptions of Stuttering Inventory (PSI): Questionnaire that assesses client's perception, may be helpful in determining awareness
Locus of Control: Scale used by clinicians to estimate how much control the client has on their stuttering
Preschool Assessment
Parent/child interaction observation
Parent interview
Obtain speech sample
Need to obtain child's awareness/feelings
Keep eye out for any other language/behavioral concerns
Comprehensive Assessment
1 . Background information– case history, informal observation, tapes from home
2 . Interviews: client, parent, teacher, key individuals
3. Observation of speech behaviors– characteristics of stuttering, related behaviors
4. Assessment of other speech, language, hearing
5. Surveys
6. Present of feelings and attitudes results:
1. No treatment warranted
2. Watchful waiting with regular family contact
3. Clinician-guided environmental change
4. Clinician-guided parent or caregiver delivered tx
Diagnosis - Typical
The following assessed would determine a _______ disfluency:
<10 disfluencies per 100 syllables
Disfluencies mostly consist of multisyllabic word/phrase reps, revisions and interjections
Repetition units are 2 or fewer
The ratio of stutter like and total disfluencies will be <50%
All disfluencies are relaxed
Diagnosis - Borderline
Have >10 disfluencies per 100 syllables (still are relaxed though)
May see more syllable reps and/or prolongations
Ratio for stutter like disfluencies is greater than 50%
Diagnosis - Beginning
Usually will see in older pre-k age
Observation of tension
Increase in prolongations
Avoidance behaviors may be present
Recommendations for Typical Fluency
Focus on family concerns vs child's disfluencies
Educate them on typical disfluencies
Provide them the assessment results to back up your conclusions
Provide them reasons for re-consult
Recommendations for Children with Borderline or Beginning Stuttering
Enhance fluency, decide if an indirect or direct approach is the best
Decrease/eliminate defensive responses to stuttering
Implement Severity Rating Scale for parents to complete at home daily.
Provide educational materials about stuttering + Getting parents involved is key!
Factors that are associated with recovery without tx
1. Decrease in stuttering-like disfluencies during the 12mos after onset
2. Female gender
3. No family hx or relatives that have successfully recovered
4. Good language and articulation skills
5. Good nonverbal intelligence scores
6. Outgoing, carefree temperament
Assessment School Age & Speech sample
Assessment
Similar to pre-k but now need to involve school
Still need to assess frequency, type of disfluencies, secondary behaviors
In addition to the parent interview, need to complete teacher interview
Classroom observation
Need to assess artic and language skills?
Speech Sample
Obtain conversational sample (optimally 300-400 syllables)
Obtain a reading sample (can you SSI-4 passage)
Need to assess pattern of disfluencies, severity, speech rate
Recommendations School Age
May consider trial therapy– It may not be clear if a child at this age is truly demonstrating stuttering or just a high level of typical disfluencies
Depending on severity and impact stuttering has on child's learning, may start with in-classroom tx, then needed "pullout" tx
Depending on client's awareness, you may want to address negative feelings/tension
Adolescent/Adult Assessment & Recommendations
Assessment
Questionnaire now includes attitude/avoidance questions (can mail out the OASES)
Interview – can be more direct, ask about past tx and the client's perception of their speech
Speech sample; conversational and reading
Informally assess receptive language, articulation and voice
Screen hearing
Recommendations
Need to determine stuttering level
Again, important to determine cause
It is important for these individuals to complete self therapy
Important to work on tx plan together
May need to bargain with the client if hesitant ("let's try 4 sessions, and then you can decide if you want to continue")
May rec trial therapy to assess their response on various treatment techniques
At this stage, tx can focus on having the client modify (play around) with their stutter
Important to address feelings/attitudes– How they feel as an individual who stutters– How they feel prior, during and after they stutter
After Initial Eval
Same for all levels
Discuss initial impressions
Educate on possible causes for disfluencies
Probable tx interventions
Give environmental/home recs
Meet informally with parents/caregivers weekly
Impact of Clinician and Clinician Views
Impact
Empathy
Warmth – makes client feel accepted, liked, nurtured.
Genuineness
Evidence-based practice
Continuing education
Creativity and Critical thinking
Views
What you believe the etiology is will shape your treatment.
Need to still make sure you are backing up your treatments with EBP and/or solid rationale
Your beliefs as a clinician may also shape the way you educate the parents/caregivers
Treatment Goals/Potential Goals
Important to ask;
What does this client need?
What does this client need from ME?
What is the most important thing to address?
What are some barriers of progress?
Goals:
Reduce frequency of stuttering
Reduce secondary behaviors (eye blinks, tension, head nods, avoidance behaviors)
Reduce negative feelings
Reduce avoidance
Create fluency-facilitating environment
Improve overall communication skills
Stuttering Modification
Stuttering modification strategies = involves working directly with the precise stutter, identify it and work on muscle relaxation during the actual stutter and decrease reaction
Ie: pull-outs, re-dos (we will discuss all of them in details when we get to treatment)
Purpose:
To increase awareness of physical tension
Reduce physical tension
Reduce struggling behaviors/unlearn secondary behaviors
Reduce negative reactions of the speaker Increase feelings of self-control
Increase awareness of speech that is disfluent
Approach stuttering in a relaxed approach
Reduce feelings of sensitive about disfluencies
Increase feelings of openness and acceptance
Reduced negative reactions to stuttering
Fluency Shaping
Fluency Shaping (enhancing) Techniques = involves changing the way the client speaks by tweaking rate, breathing, articulation. Does not address feelings or secondary behaviors, do not bring attention to specific stutters
breathing techniques, light articulatory contact
Purpose:
Obtain fluent speech outside of stuttering behaviors, or before stuttering events.
Prevent the intensity or frequency of stuttering behavior.
Allow for success in achieving fluency to increase confidence, decrease negative reactions to stuttering by promoting fluent speech.
Alter speakers’ articulation, speech rate, breath patterns, voice productions and other aspects of communication to reduce vulnerabilities to disfluencies.
Reduce Frequency
Operant treatment– positive reinforcement for fluency or tactfully calling attention to stuttering to allow "do-overs"
Positive reinforcement: verbal praise, tangible prizes, rewards when child produces fluent speech
Fluency shaping techniques– Find a level and/or method that results in fluent speech and then advance
Reduce Secondary Behaviors
Based on belief that secondary behaviors are fueled by negative feelings that result in increased tension/fear and then rewarded bc person pushes through tension to produce word.
Implement stuttering modification strategies that directly address the precise stutter and associated negative feeling
Reduce negative emotions by:
Objectively studying it with client
Desensitizing the frustration and embarrassment
Implementing stuttering modification strategy; cancellations/redos, pull-outs,
Reduce Negative Feelings
Use cognitive behavioral therapy – helping clients think and feel more positively about their speech, listeners and diving into the environments/situations that elicit negative emotions
Reduce Avoidance
Because of temperament, learned behavior or both the avoidance may be "hard-wired" in
Usually see with intermediate/advanced stuttering
Start by addressing negative emotions, fears, perceived listener reactions – client needs to learn new responses to old stimuli
Create Fluency Facilitating Environment
Tweaking an environment might be the only thing needed with borderline stuttering
Have parents speak at slower rate, frequent pauses, increase 1:1 attention
For school-age children, important to involve the classroom.
For adults, important for them to create a supportive environment, get loved ones involved
Fluency Shaping (enhancing) Techniques
involves changing the way the client speaks by tweaking rate, breathing, articulation. Does not address feelings or secondary behaviors, do not bring attention to specific stutters
Purpose
Obtain fluent speech outside of stuttering behaviors, or before stuttering events.
Prevent the intensity or frequency of stuttering behavior.
Allow for success in achieving fluency to increase confidence, decrease negative reactions to stuttering by promoting fluent speech.
Alter speakers’ articulation, speech rate, breath patterns, voice productions and other aspects of communication to reduce vulnerabilities to disfluencies
Fluency Enhancing Techniques
Light Contact: Producing plosive sounds more gently/decrease tension
Easy onset: Producing non-plosive sounds more easily
Slower speech rate/stretched speech: Slow down rate of speech or prolong speech sounds in a general capacity
Relaxed breath: Work on coordinating respiration with phonation. Understanding deep breaths vs shallow vs full breaths
Pausing: Identifying/creating natual breaths allowing for pausing
Stuttering Modification Strategies
involves working directly with the precise stutter, identify it and work on muscle relaxation during the actual stutter and decrease reaction
Purpose
To increase awareness of physical tension
Reduce physical tension
Reduce struggling behaviors/unlearn secondary behaviors
Reduce negative reactions of the speaker Increase feelings of self-control
Increase awareness of speech that is disfluent
Approach stuttering in a relaxed approach
Reduce feelings of sensitive about disfluencies
Increase feelings of openness and acceptance
Reduced negative reactions to stuttering
Stuttering Modification Strategies
Pull-outs/sliding: stretching of the actual stuttering moment. (ie: sssssslide)
Bouncing: Produce words with more ease. Increase awareness of where tension is (ie: Ball = B B B Ball)
Cancellation/re-do: Produce word again after stutter with less tension and at a slower rate, more controlled (ie: "I w w w want (want) to go)
Catching the stutter: Only to use during tx. Have client identify tension/stuttering moments by signaling to increase awareness.
Intentional stuttering: Used to reduce anxiety, increase sense of control
Borderline? Potential Goals
Reduce frequency of stuttering
Reduce secondary behaviors (eye blinks, tension, head nods, avoidance behaviors)
Reduce negative feelings
Reduce avoidance
Create fluency-facilitating environment
Improve overall communication skills
Reduce Frequency
Operant treatment – positive reinforcement for fluency or tactfully calling attention to stuttering to allow "do-overs"
Positive reinforcement: verbal praise, tangible prizes, rewards when child produces fluent speech
Fluency shaping techniques
Find a level and/or method that results in fluent speech and then advance
Create Fluency Facilitating Environment
Tweaking an environment might be the only thing needed with borderline stuttering
Have parents speak at slower rate, frequent pauses, increase 1:1 attention
For school-age children, important to involve the classroom.
For adults, important for them to create a supportive environment, get loved ones involved
Education
Educating the parents/ family is so important
Can provide them video/book/website recs
Write down specific modeling techniques
Brainstorm together how to facilitate fluency in their home environment
Educate and then Collaborate! Partnership with Parents
Begin by identifying factors which disrupt fluency
Child Related vs environmental
And then educate & collaborate:
Listen and Learn; Communicate openly
Share decision making
Respect parent’s choices/opinions