Operative Obstetrics, Substance Abuse, Teratogens
1/63
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
64 Terms
C-Section
The abdominal delivery of a baby
Frequency has increased over time
Physician fear of malpractice lawsuits
Increase for first time mothers
Introduction of electronic fetal monitoring, decrease in operative vaginal deliveries, and attempts at vaginal breech deliveries
Has been slight increase in TOLACs (trial of labor after cesarean)
Indications for C-section
Performed when vaginal delivery would pose greater risk to mother or fetus
Labor related (MC) – failure to progress or fetal distress
Malpresentation – breech, transverse or oblique lie, face/brow presentation (persistent)
Placental indications – placenta previa, vasa previa, placenta accreta spectrum, severe placental abruption
Prior uterine surgery – prior classical (vertical) C-section, prior uterine rupture, extensive trans-fundal surgery, multiple prior C-sections
Maternal indications – active genital herpes lesions, certain pelvic structural abnormalities, severe cardiac disease, certain neurological conditions (brain aneurysm at risk of rupture), severe preeclampsia with unfavorable cervix
Infectious indications – active HSV lesions, HIV with high viral load (>1000 copies/mL), certain cases of primary CMV or varicella near delivery
Multiple gestation – twin A not vertex, mono-amniotic twins, high-order multiples
Fetal indications – suspected macrosomia, severe fetal growth restriction with abnormal dopplers, certain fetal anomalies
Emergent indications – uterine rupture, cord prolapse, severe abruption with instability, failed operative vaginal delivery
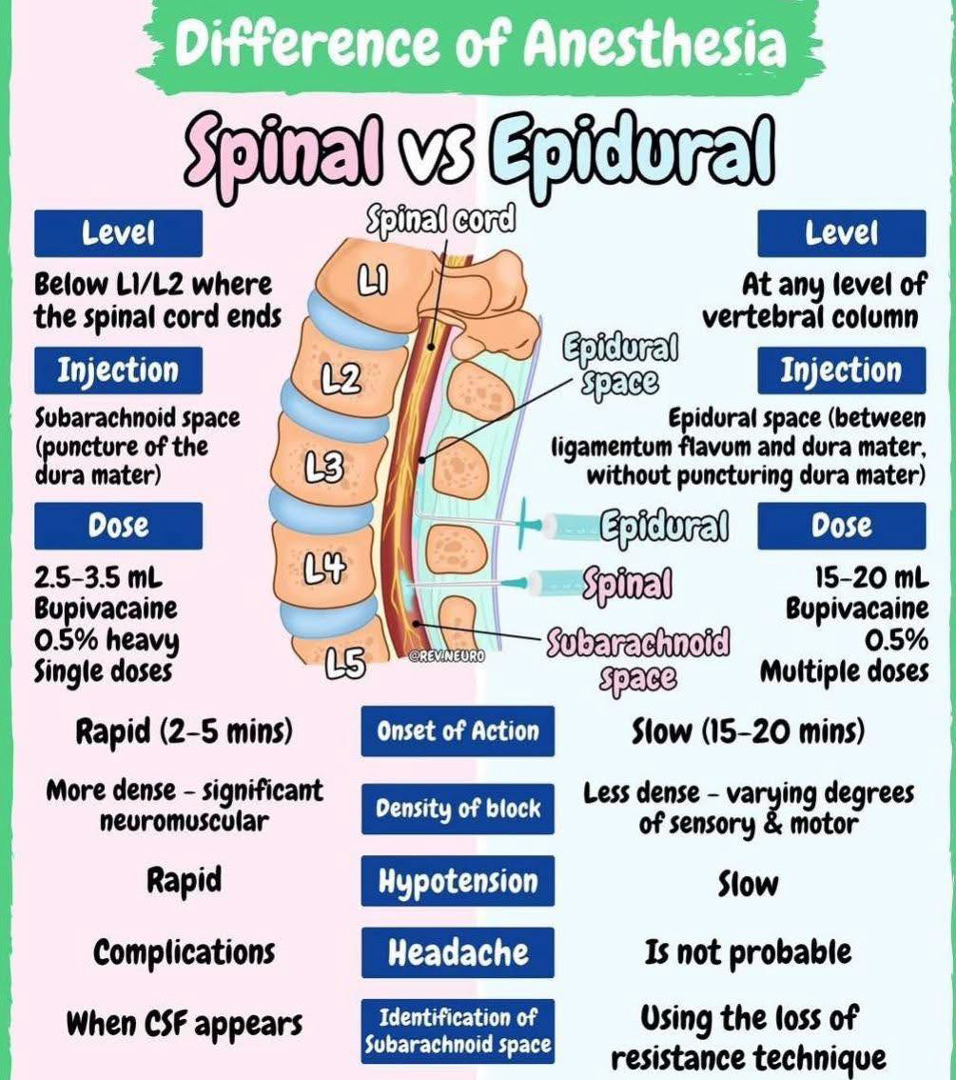
Spinal Anesthesia
A single injection of local anesthetic (± opioid) into the subarachnoid space (CSF) at L3-L4 or L4-L5
Used for scheduled C-sections
Benefits
Onset is very rapid (5-10 min)
Minimal fetal exposure
Limited duration (~1.5-3 hrs)
Risks
Possible hypotension
Post-dural puncture headache

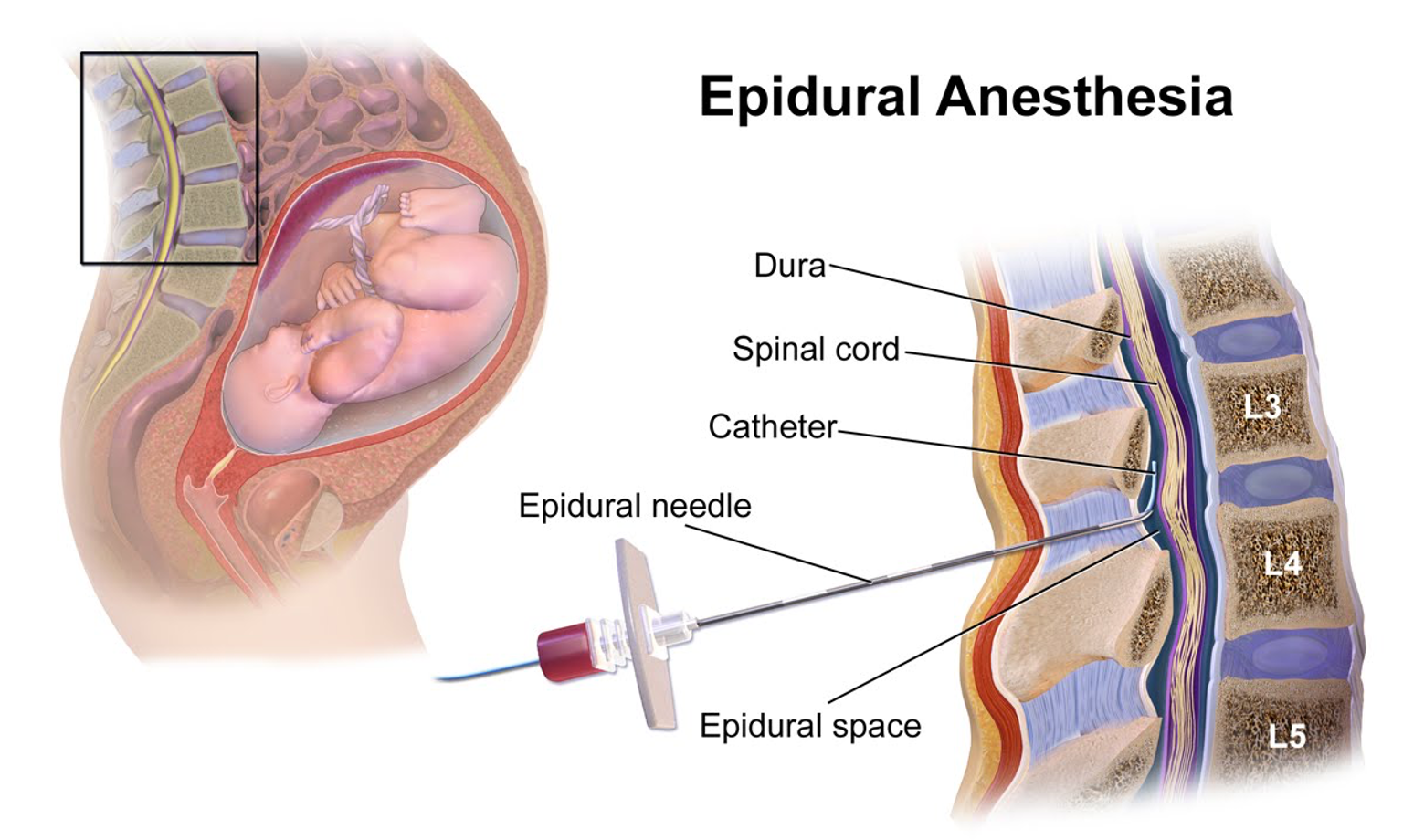
Epidural Anesthesia
Typically used for vaginal birth
Catheter placed into the epidural space and medication infused continuously
Labor epidural that is “topped up” for C-section
Slower onset (10-20 min)
Adjustable dosing, can extend duration
Lower hypotension risk compared to spinal
May fail → need to convert to general anesthesia
Spinal vs Epidural
General Anesthesia
IV induction, endotracheal intubation, inhaled anesthetic maintenance
General Anesthesia Indications
True emergency (ex: uterine rupture, cord prolapse)
Crash C-section
Neuraxial contraindicated
Failed spinal/epidural
Patient refusal
Coagulopathy
Severe thrombocytopenia
General Anesthesia Disadvantages
Higher maternal morbidity and mortality
Risk of aspiration (pregnancy = full stomach)
Difficult airway risk (edematous airway)
Neonatal respiratory depression (if prolonged induction)
Patient not awake for birth
Neuraxial Anesthesia
Spinal and epidurals are both considered neuraxial
Neru. → nerve/nervous system
Axial → axis (central line of the body)
Neuraxial anesthesia refers to anesthesia delivered along the central nervous system axis
Neuraxial Anesthesia Contraindications
Platelets <70-80k
Coagulopathy
Infection at insertion site
Severe hypovolemia
Patient refusal
Increased intracranial pressure
Neuraxial Anesthesia and Platelets
During neuraxial placement (spinal or epidural), a needle passes through tissues → small blood vessels can be injured and normally bleeding stops quickly
Platelets are essential for clot formation
If platelets are low → bleeding may not stop and blood can accumulate in the epidural or spinal space → forms a spinal epidural hematoma which can compress the spinal cord and cause paralysis
You cannot see bleeding in epidural space and symptoms may not appear immediately
If platelets <70,000 → neuraxial anesthesia is avoided and general anesthesia is used
HELLP syndrome → more caution because platelets are dropping rapidly
C-Section Step 1: Preparation
Confirm indication
Fetal heart check
Consent
IV access
Type & screen
Antibiotics (cefazolin before incision)
Sequential compression devices
Foley catheter
Neuraxial anesthesia
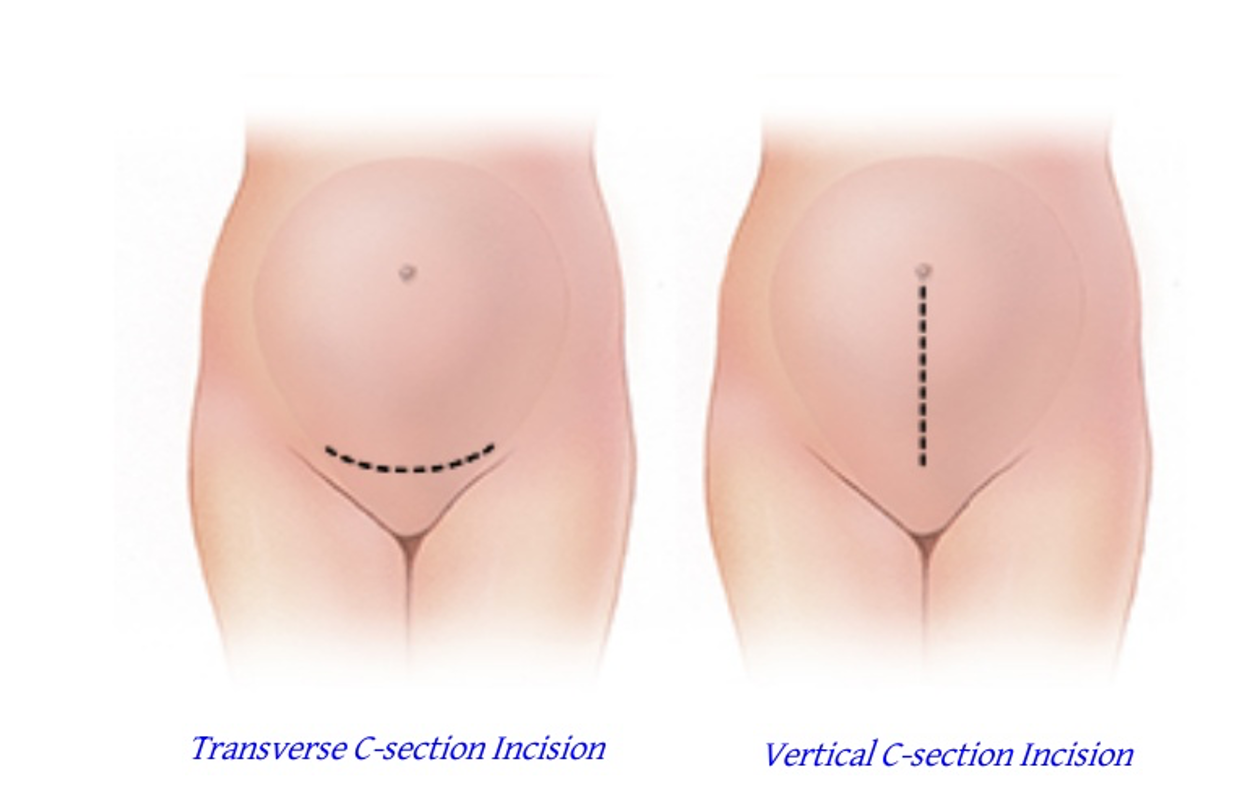
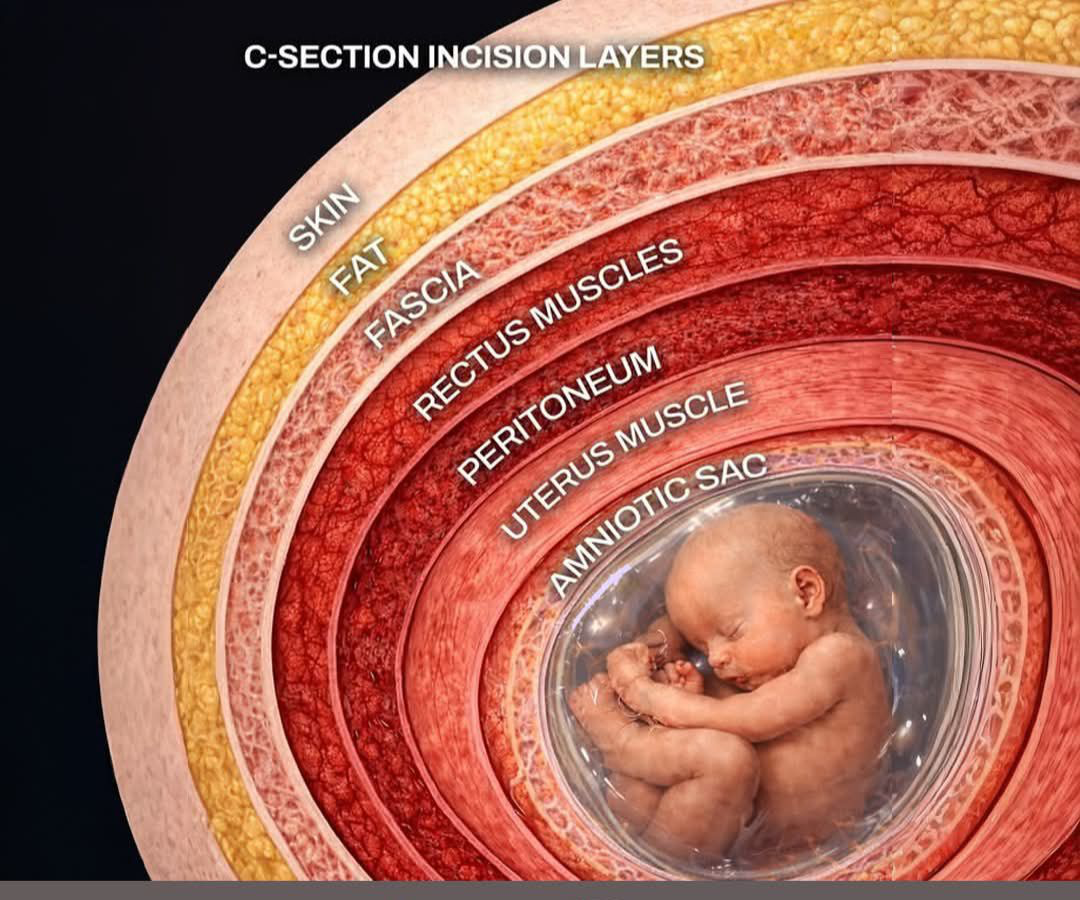
C-Section Step 2: Skin Incision
Most commonly Pfannensxiel incision → curved transverse incision 2-3 cm above pubic symphysis, through the skin and subcutaneous tissue
C-Section Step 3: Open Fascia
Incise anterior rectus sheath transversely
Extend laterally
Separate fascia from rectus muscles

C-Section Step 4: separate rectus muscles
Rectus muscles separated in midline
Enter peritoneum carefully (bladder could be there)
Extend peritoneal opening
Now the abdomen is entered

C-Section Step 5: expose the uterus
Identify the lower uterine segment
Bladder blade is inserted
Create bladder flap (depends on surgeon)
Incise vesicouterine peritoneum
Push bladder down
C-Section Step 6: uterine incision (hysterotomy)
Low transverse uterine incision
Small transverse incision in lower uterine segment
Do very slowly
Extend bluntly with fingers or scissors
C-Section Step 7: deliver the baby
Rupture membranes (if intact)
Deliver fetal head
Gentle but firm fundal pressure
Suction mouth/nose if needed
Clamp and cut cord
Neonatal team received baby
Time from incision to delivery ideally <5 minutes
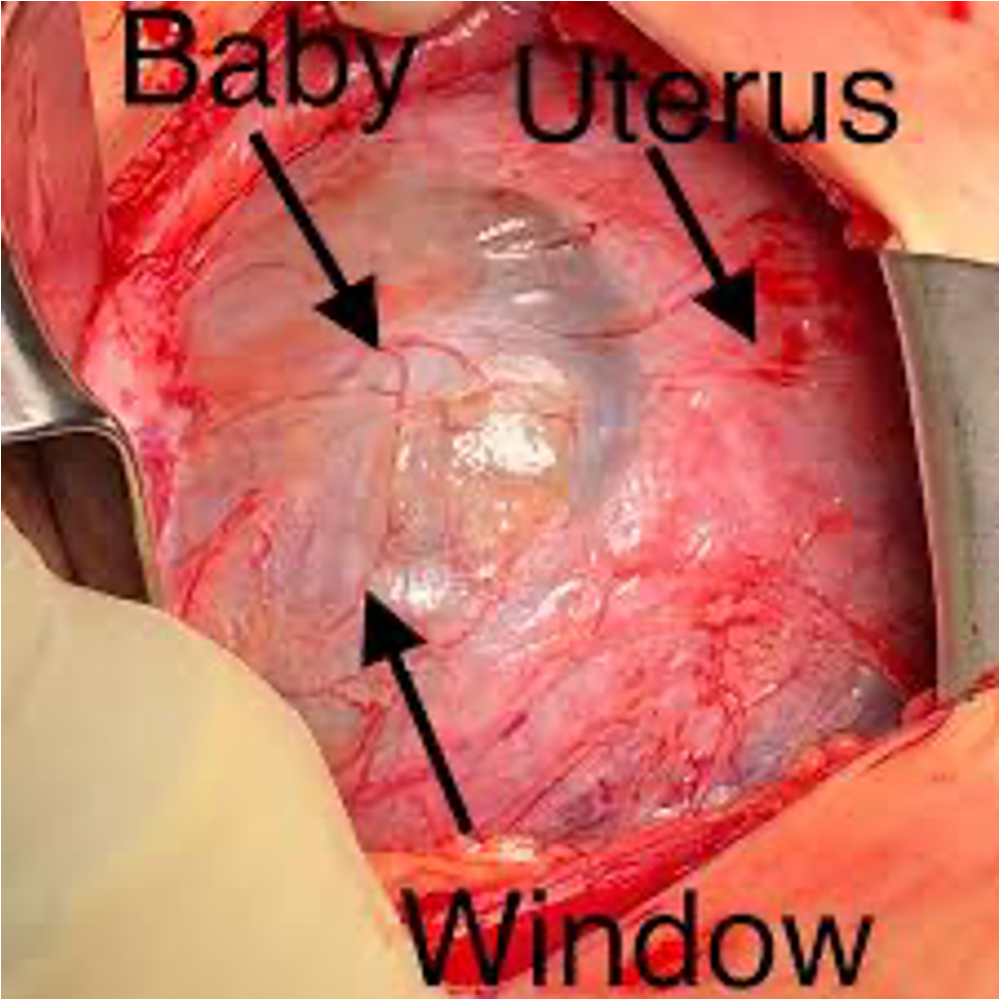
Uterine Window
Refers to marked thinning of a prior uterine scar where the myometrium is so thin that the fetal membranes or even the fetus can be seen through it but the uterus has not fully ruptured
Extremely thin lower uterine segment
Weak prior scar and increased risk of uterine rupture in future pregnancies
Usually recommended to not get pregnant again
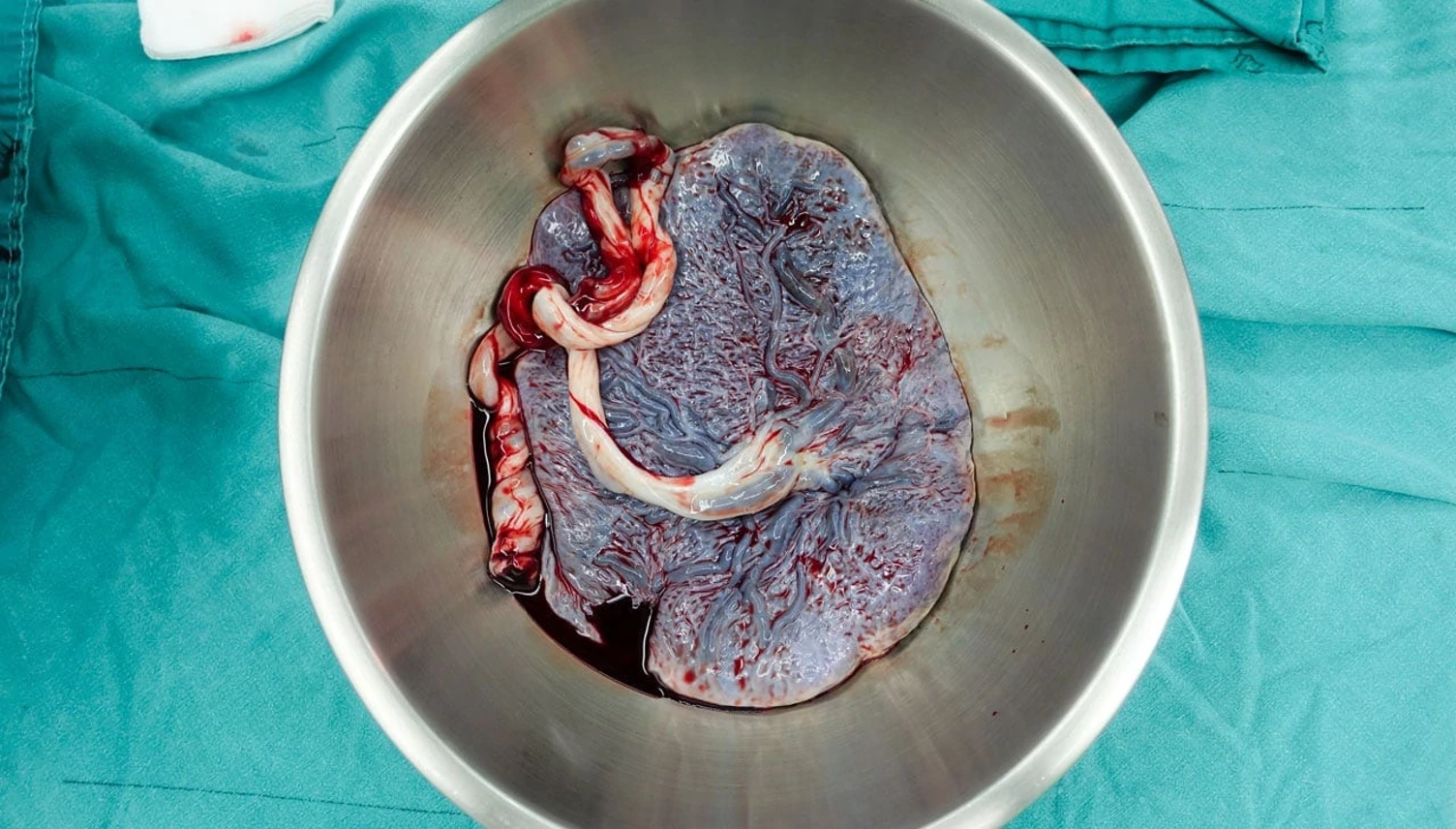
C-Section Step 8: deliver the placenta
Gentle and controlled cord traction
Uterine massage
Oxytocin started (especially if boggy uterus)
C-Section Step 9: inspect the uterus
Check cavity for retained tissue
Clear clots
Assess incision edges
C-Section Step 10: close the uterus
Usually 1-2 layer closure
Absorbable suture
Ensure hemostasis
C-Section Step 11: close the abdomen
Return uterus into abdomen (lots of pressure for the patient)
Irrigate
Close fascia (most important layer)
Re-approximate subcutaneous tissue (if thick)
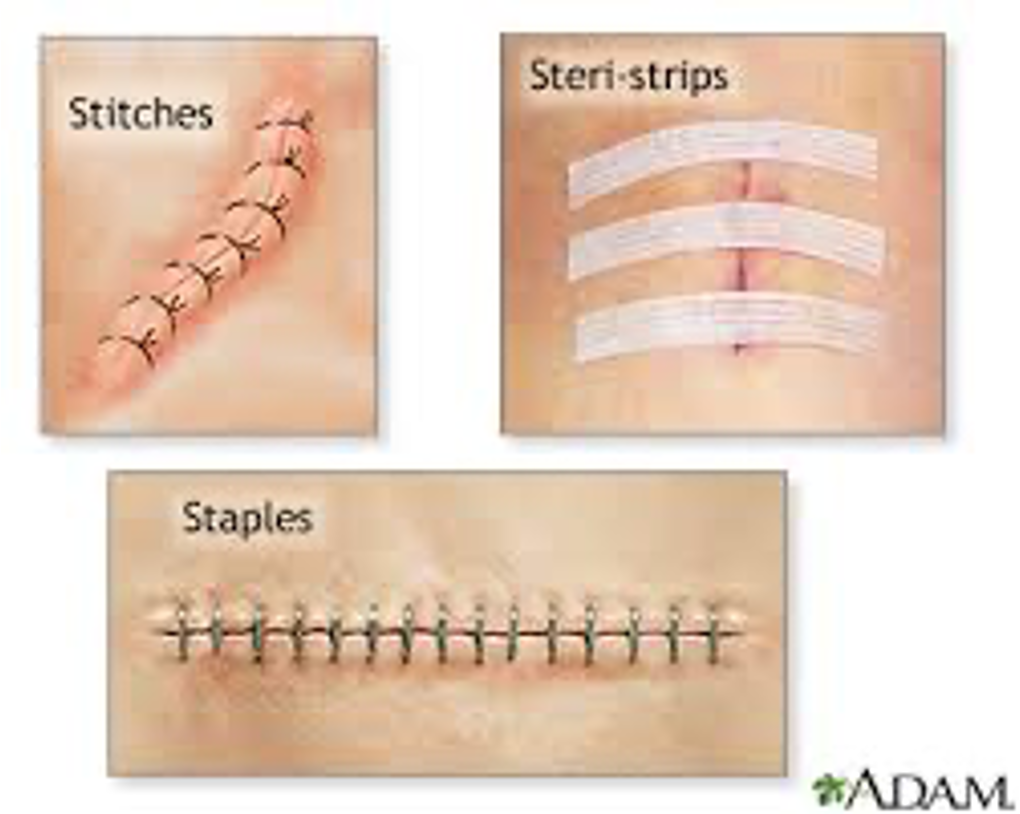
Close skin (sutures, staples, or glue)
C-section Incision Layers
Common C-section Intra-op Complications
Uterine incision extension
Bladder injury
Postpartum hemorrhage
Adhesions (repeat cases)
Bowel injury (rare)
Effects of C-section for Newborn
Immediate effects
Respiratory distress (MC)
During vaginal birth the uterine contractions help squeeze fluid from fetal lungs; catecholamine surge helps clear lung fluid
In C-section there is no “thoracic squeeze” → less catecholamine surge; delayed lung fluid clearance
This results in transient tachypnea of the newborn (TTN)
Rapid breathing, mild oxygen need, usually resolves in 24-72 hours
More common if elective C-section before 39 weeks and no labor prior to surgery
Lower initial breastfeeding rates
Possibly due to delayed skin-to-skin, maternal pain/recovery, separation in the OR, effects of anesthesia
Microbiome & immune effects
Babies born vaginally are exposed to maternal vaginal and gut flora
C-section babies are exposed more to skin and hospital flora
Research shows differences in early gut microbiome composition, and some studies suggest small associations with: higher rates of asthma, allergies, T1 DM, obesity
Breastfeeding helps normalize microbiome differences
Positive Effects of C-section for Newborn
Prevents hypoxic injury in fetal distress
Prevents trauma in breech birth
Prevents birth injuries
Reduces vertical HSV transmission
Reduces HIV transmission (if high viral load)
In many cases, it is lifesaving
TOLAC vs VBAC
TOLAC = trial of labor after Cesarean section
TOLAC is an attempt at vaginal delivery: the goal is to achieve VBAC but still may result in another C-section if labor fails (failed TOLAC ending in repeat C-section usually has more complications)
Higher likelihood if prior vaginal delivery has occurred
Lower likelihood if labor is induced or augmentation is required
Women who had C-section for breech are more successful with TOLAC than women who had C-section for arrest of labor
VBAC = vaginal birth after Cesarean section
Not all TOLACs will end up with VBACs, it is just a trial and may end up in a C-section regardless
Best case scenario and elective repeat C-section is the next best scenario
As TOLACs increased over time, so did reports of uterine rupture and other complications → increased liability → reversed to higher C-section rates → needs to be risk/benefit conversation with patient
TOLAC Candidates
High VBAC success rates and low rupture risk
Candidates:
One prior low transverse C-section (best candidate)
Prior vaginal delivery (strong predictor of success)
Vaginal birth before or after C-section
Spontaneous labor
Nonrecurring indication for prior C-section
Ex: breech, fetal distress, placenta previa
Adequate pelvis/average fetal size
Institution capable of emergency C-section
TOLAC Contraindications
Prior classical (vertical) uterine incision
High rupture risk
Prior uterine rupture
High recurrence risk
Prior T-incision or J incision (incisions on uterus)
Extensive trans-fundal uterine surgery
Myomectomy entering cavity
Deep uterine construction
Contraindications to vaginal delivery
Placenta previa, vasa previa, transverse lie, active HSV lesions
TOLAC Relative Contraindications
Lower success rate
Multiple prior C-sections (2+)
Suspected macrosomia (>4500 g)
Obesity
Induction of labor
Prior arrest of descent
Short inter-pregnancy interval (<18 mo)
TOLAC Procedure
Oxytocin and epidural are acceptable
NOT safe to use prostaglandins for cervical ripening (ex: misoprostol, cervidil)
Increased risk of uterine rupture
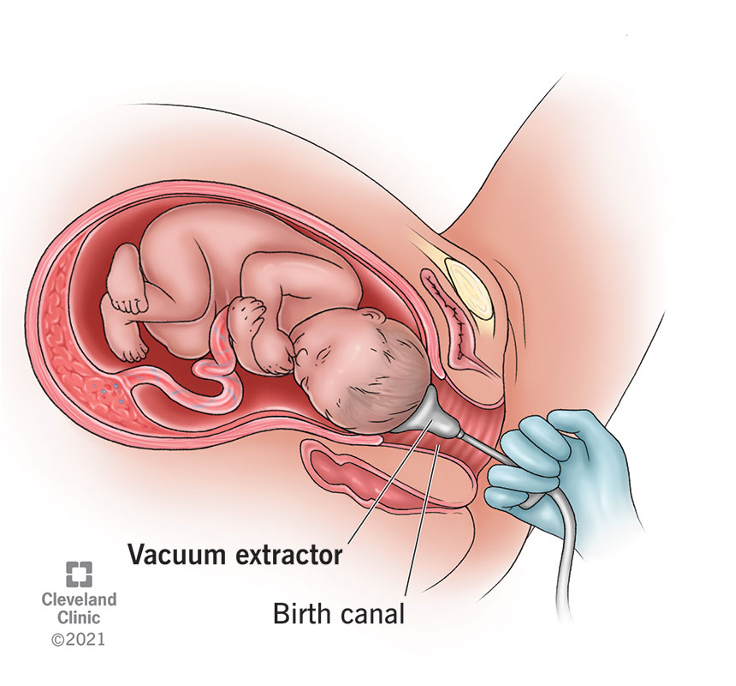
Operative Vaginal Delivery
Assisted vaginal birth using forceps or vacuum to expedite delivery of the fetal head
Used when vaginal delivery is possible but needs assistance
Types:
Vacuum extraction
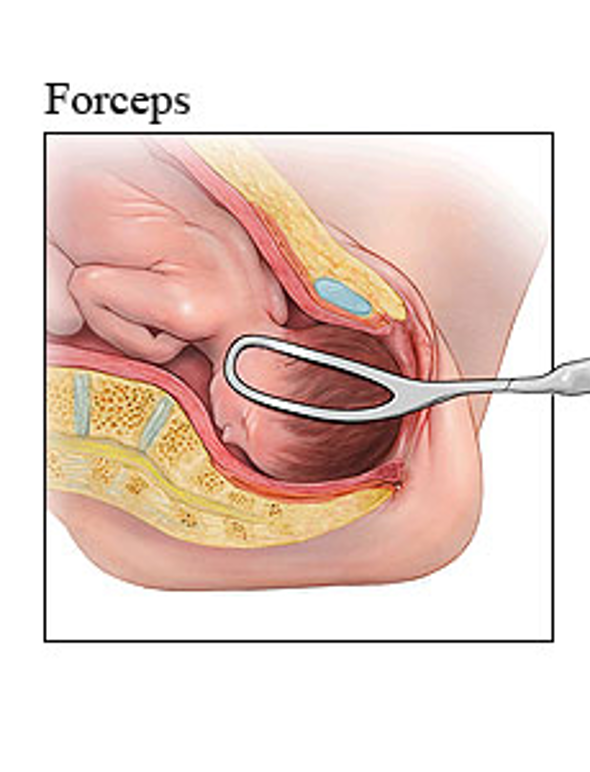
Forceps delivery
Vacuum Extraction
Soft or rigid suction cup applied to fetal scalp → negative pressure created → traction applied during contractions
Forceps Delivery
Two metal blades placed around fetal head → traction applied
Can also rotate fetal head
Used less commonly
Indications for Operative Delivery
Prolonged second stage of labor
Non-reassuring fetal heart tracing
When delivery is needed quickly
Maternal exhaustion
Maternal medical conditions when pushing should be limited
Cardiac disease
Severe preeclampsia
Certain neurologic conditions
Prerequisites for Operative Delivery
All MUST be present
Full cervical dilation
Ruptured membranes
Known fetal position
Fetal head engaged (+2 station)
No suspicion of cephalopelvic disproportion
Adequate anesthesia
Empty bladder
Informed consent
Ability to proceed to emergency C-section if needed
Operative Delivery Maternal Complications
Perineal lacerations (higher risk with forceps)
Vaginal tears
Postpartum hemorrhage
Pelvic floor injury
Neonatal
Operative Delivery Fetal Complications
Vacuum
Scalp lacerations
Cephalohematoma
Subgaleal hemorrhage (rare but serious)
Jaundice
Forceps
Facial nerve palsy
Skull fractures (rare)
Ocular injury (rare)
Intrauterine Fetal Demise
ACOG defines fetal demise as a fetus that dies in the uterus
Used in clinical and diagnostic settings before delivery
Describes the clinical event of fetal death before delivery
Does not specify gestational age
Intrauterine Stillbirth
ACOG defines stillbirth as the delivery of a fetus that shows no signs of life
Used after delivery when the fetus is born without life
After 20 weeks gestation
Used more as a vital statistics/public health term
Stillbirth Causes
Most common is placental insufficiency/placental dysfunction
20-40% remain unexplained
Maternal → hypertension, preeclampsia, diabetes, thrombophilias, lupus
Infection → listeria, syphilis, parvovirus B19, CMV, chorioamnionitis
Fetal → genetic abnormalities, congenital malformations, severe growth restriction
Umbilical cord events → true knot, prolapse, hyper-coiling
Stillbirth Evaluation
Review genetic, medical and obstetric history
Determine if consanguinity
Encourage autopsy
Photos of fetus and any abnormalities
Full-body skeletal x-rays
Full-body MRI
Look for dysmorphic features
Obtain cord blood for chromosomal DNA analysis
Obtain fetal serum for infectious disease studies
Obtain fetal tissue sample for cell culture
Obtain parental bloods for chromosome analysis
Communicate final autopsy results
Provide follow-up counseling
Induced Abortion
The termination of a pregnancy medically or operatively before fetal viability (definition of viability varies from state to state)
Elective voluntary – interruption of pregnancy at the request of the mother
Therapeutic – interruption of pregnancy for the purpose of safeguarding the health of the mother or fetus incompatible with life
Performed first and second trimester
Must be aware of state laws
Techniques
Mechanical
D & E: suction or curettage
Medical – up to 9 weeks (varies, but the larger the size the more pain and cramping and possibility for incomplete abortion)
Pre-abortion work up
U/S – assure dates correspond with uterine size
Labs – ABO/Rh typing
Administer Rhogam in Rh (-) moms
Careful patient counseling should be performed
Medication Induced Abortion
Early pregnancy, approved up to 10 weeks gestation
Mifepristone + Misoprostol (gold standard)
Mifepristone 200 mg PO followed 24-48 hours later by misoprostol 800 mcg buccal, vaginal, or sublingual
Causes decidual breakdown, uterine contractions, cervical softening
Expected symptoms
Cramping
Heavy bleeding
Passage of clots
Nausea
Fever
Diarrhea
Misoprostol-only regimen (when mifepristone is unavailable)
800 mcg vaginal/buccal repeated every 3-4 hours (up to 3-4 doses)
Slightly lower efficacy than combination
Prescribers must complete a one-time prescriber agreement form under the REMS program (Risk Evaluation and Mitigation Strategy)
Some states restrict or ban prescribing mifepristone
Need to follow up to confirm termination with bHCG and vaginal US
Medication Induced Abortion Contraindications
Confirmed or suspected ectopic pregnancy
Chronic steroid use (mifepristone blocks glucocorticoid receptors)
Could maybe use misoprostol only regimen
Bleeding disorder
Anticoagulation
IUD in place (must remove first)
Surgical Induced Abortion
Vacuum aspiration (manual or electric) up to 14-16 weeks
Cervical dilation and then suction device removes products of conception
Takes 5-10 minutes
Have local anesthesia with possible sedation
Dilation and evacuation (D&E)
Cervical preparation (misoprostol or osmotic dilators) and instrumental removal of fetal and placental tissue
Done in second trimester (14-24 weeks)
Complications of Induced Abortion
Hemorrhage
Infection
Retained tissue
Ongoing pregnancy
Uterine perforation (procedural)
Asherman syndrome (rare: scar tissue forms in uterus)
Therapeutic Induced Abortion
Pregnancy significantly endangers maternal life or major organ function
Therapeutic abortion ≠ elective abortion
Therapeutic Induced Abortion: Maternal Indications
Severe maternal medical disease
Severe cardiac disease (ex: pulmonary HTN)
Advanced cardiomyopathy
Severe renal failure
Severe pulmonary disease
Certain cancers requiring urgent treatment
Uncontrolled severe autoimmune disease
Life-threatening obstetric complications → pre-viable
Severe preeclampsia
HELLP syndrome
Placental abruption
Chorioamnionitis
PPROM with infection
Uterine rupture
Uncontrolled hemorrhage
Psychiatric conditions
Severe psychiatric illness with high risk of self-harm
Suicidal ideation directly related to pregnancy
Therapeutic Induced Abortion: Fetal Indications
Lethal fetal anomalies
Anencephaly
Bilateral renal agenesis
Severe skeletal dysplasia incompatible with life
Certain lethal genetic syndromes
Severe hydrops fetalis with poor prognosis
Severe chromosomal abnormalities → trisomy 13, trisomy 18, certain triploidy cases
Severe early growth restriction with non-viability
Rape or incest (depending on legal/ethical frameworks)
Substance Abuse in Pregnancy
A medical condition, not a moral issue
Pregnancy is a critical opportunity for treatment
Substance use includes:
Tobacco
Alcohol
Opioids (heroin, prescription opioids, fentanyl)
Cocaine
Methamphetamine
Cannabis
Benzodiazepines
Poly-substance use (very common)
Substance Abuse in Pregnancy Maternal Risks
Poor prenatal care
Malnutrition
Intimate partner violence (IPV)
Infections (HIV, hepatitis C)
Placental abruption (especially cocaine)
Preterm labor
Overdose (leading cause of maternal mortality in some states)
Substance Abuse in Pregnancy Screening
UNIVERSALLY SCREEN
Urine toxicology should be consented
Not required
Be aware of the laws in your state
Substance Abuse in Pregnancy Management
Do NOT abruptly stop certain substances without supervision
Social work involvement
Mental health care
Teratology
The study of abnormal development and congenital malformations (birth defects) and the agents that cause them
Teratogen is any agent that can cause abnormal fetal development
Ex: smoking, alcohol, drugs, medications, infections, radiation, hyperthermia
Effect depends on timing, dose, route, and length of teratogen
Timing
“All-or-none” exposure in weeks 0-2: either have pregnancy loss or no effect at all
Most sensitive during organogenesis → weeks 3-8 (when we start to be worried about malformations)
Dose matters (higher dose = higher risk)
Chronic exposure → more severe effects
Genetic susceptibility matters
Some organs are more vulnerable than others
Tobacco and Pregnancy
Most common
Pathophysiology
Nicotine → vasoconstriction → placental insufficiency
Carbon monoxide replaces oxygen in the blood, leading to fetal hypoxia
Fetal/newborn effects
IUGR
Low birth weight
Placental abruption
Preterm birth
Stillbirth
SIDS
Quitting in the 1st trimester reduces the risk of low birth weight to nearly that of a non-smoker
Stopping at any state of pregnancy improves oxygen delivery, increases fetal growth, and reduces complications
Management
Behavioral counseling
Nicotine replacement therapy
Alcohol and Pregnancy
Pathophysiology
ETOH crosses placenta: fetal blood ETOH ~ maternal ETOH
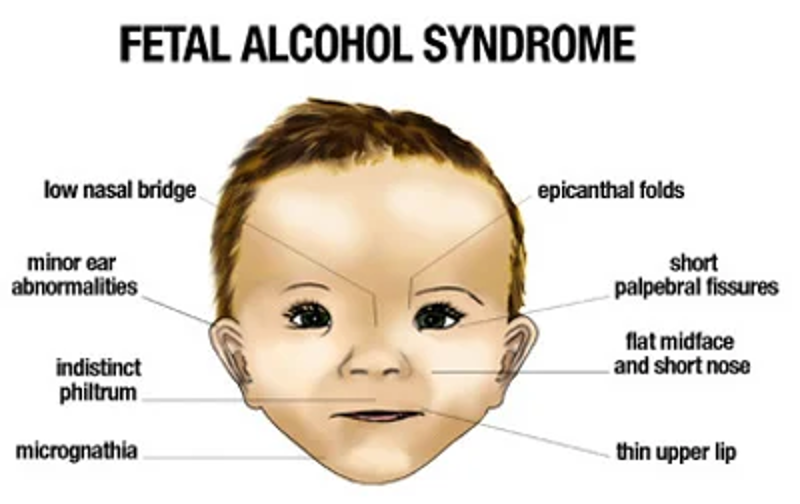
Fetal alcohol spectrum disorder (FASD)
No known amount where you could get it or you could not
Facial anomalies
Growth restriction
Microcephaly
Intellectual disability
Behavioral problems
One of the most common preventable causes of birth defects and childhood disabilities
Management
Behavioral therapy
Inpatient detox if severe dependence
Breastfeeding:
Avoid heavy use
Recommended to wait 3-4 hours after a single drink before breastfeeding
If ”buzzed”: alcohol is in the breastmilk
Cannabis
Data is evolving on this
Can actually worsen nausea
THC crosses placenta and enters the fetal bloodstream → binds to cannabinoid receptors in the fetal brain which are critical for neural growth & brain development
Not associated with major structural anomalies
Associated with
Lower birth weight
Neurodevelopmental concerns
Attention problems
Breastfeeding discouraged
THC is stored in fat and remains in breast milk for days to weeks after use, which can cause delayed motor development for the infant
Opioids
Heroin, Oxycodone, Fentanyl
Cross the placenta and enter the fetal bloodstream
Risks during pregnancy
Preterm birth
IUGR
Stillbirth (if overdose)
Neonatal abstinence syndrome (NAS)
Withdrawal symptoms after birth (irritability, high-pitch cry, tremors, poor feeding, diarrhea)
Preferred treatment: medication-assisted treatment (MAT)
Methadone
Buprenorphine
Do NOT detox abruptly → increases relapse and overdose risk
Breastfeeding reduces NAS severity in opioid-exposed infants
Breastfeeding encouraged if mom is on methadone or buprenorphine and not using illicit opioids
Cocaine
Intense vasoconstriction
Crosses the placenta and fetal blood-brain barrier
Risks
Placental abruption
Preterm birth
Stroke
IUGR
Cocaine overdose is a medical emergency
Ice baths, cooling blanket, sedation with a benzodiazepine and BP control (avoid beta blockers: may worsen hTN by causing unopposed alpha-adrenergic vasoconstriction)
Breastfeeding contraindicated if actively using – major cardiovascular changes in neonates
Methamphetamine
Similar to cocaine risks: growth restriction, preterm birth, neurodevelopmental concerns
Breastfeeding contraindicated if actively using
Benzodiazepines
Possible neonatal withdrawal
Floppy infant syndrome (rare)
Sedation
Teratogenic Medications
Retinoids vitamin A derivatives (Accutane) → absolute contraindication
Can cause cleft palate, microtia/anotia, cardiac defects, CNS abnormalities, thymic hypoplasia
Patients on Accutane need to sign up for iPLEDGE program
Anti-epileptics (Valproate, Carbamazepine)
Neural tube defects
Use lowest effective dose and take folic acid 4mg daily
Antibiotics
Tetracyclines → permanent tooth discoloration and bone growth inhibition
Fluoroquinolone → cartilage toxicity
Trimethoprim → neural tube defects in 1st trimester
Sulfonamides (near term) → displaces bilirubin from albumin which can cause increased risk of kernicterus
Aminoglycosides → ototoxicity
Chloramphenicol → gray baby syndrome
Nitrofurantoin → avoid near term due to risk of hemolysis in G6PD deficiency
Warfarin → use heparin in pregnancy
ACE inhibitors (specifically 2nd/3rd trimester)
Infections (TORCH)
Radiation → high dose exposure causes microcephaly and intellectual disability
Chemotherapy dependent on gestational age
Methotrexate contraindicated → folate antagonist, causes severe malformations
Psychiatric medications
Paroxetine (Paxil) → slight increased risk of cardiac defects in 1st trimester
Lithium → Ebstein anomaly (cardiac anomaly)