15. Surgery of the Elbow 1
1/70
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
71 Terms
denotes a joint but has also been defined as degenerative disease of a joint
definition of arthrosis
inflammation affecting several joints
define polyarthritis
noninflammatory degenerative joint disease (DJD) characterized by articular cartilage degeneration, marginal bone hypertrophy (osteophytosis) and synovial membrane changes
define osteoarthritis/osteoarthrosis
result of DJD or inflammatory diseases...joint is fused after new bone production
define ankylosis
joints lined w/ synovial membrane...allow relatively free movement
define synovial joints
connected w/ fibrous tissue allowing for little/no movement in places like skull and tooth sockets
define fibrous joints
connected w/ cartilage allowing for little/no movement in places like mandibular symphysis and growth plates
define cartilaginous joints
use of endoscope to examine/treat joints
define arthroscopy
surgical exposure of a joint
define arthrotomy
define revision of a joint structure
define arthroplasty
surgical tx. for joint fusion
define arthrodesis
abnormal development of tissues, organs, or cells
define dysplasia (frequently dx as hip or elbow dysplasia)
canine elbow dysplasia
what is the leading cause of forelimb lameness in dogs
polygenetic train w/ both hereditary and environmental influence
what is involved in breed disposition to canine elbow dysplasia
breeding of these dogs should be STRONGLY discouraged
canine elbow dysplasia is a hereditary condition so....
1. OCD
2. fragmented coronoid process (FCP)
3. medial compartment disease (MCD)
4. ununited anconeal process
what other conditions are considered forms of elbow dysplasia
incomplete ossification of humeral condyle
what additional developmental disease of the canine elbow can cause similar C/s or lead to fracture of a humeral condyle
hereditary
strong evidence of ____ component in etiology of elbow dysplasia
1. loss of elbow ROM shows evidence of DJD...in immature large dogs can indicate presence of elbow dysplasia
2. RAD positioning is essential for dx. of subtle lesions
3. both elbows need RADs
4. sx. removal of bone and cartilage pieces usually improves limb function
important considerations for tx. of elbow dysplasia
1. complete or partial separation of small portion of medial coronoid process of ulna leading to lameness and DJD
2. disease process (often in large dogs) that starts when animal is immature having C/s appearing around 5-7 months of age
what are some characteristics of fragmented coronoid process (FCP)
1. walk with shortened steps, decreased ROM, and pain on hyperextension of elbow
2. symmetrical or asymmetrical mm. atrophy
3. joint effusion and periarticular soft tissue swelling...felt when dog is standing
4. crepitation if advanced OA is present....manipulation painful
PE findings associated with fragmented coronoid process (FCP)
pain on hyperextension of elbow
what is often the earliest sign of FCP
shoulder not flexed and extended during elbow manipulation
when performing a PE, what is key in order to prevent mistaking shoulder pain for elbow pain
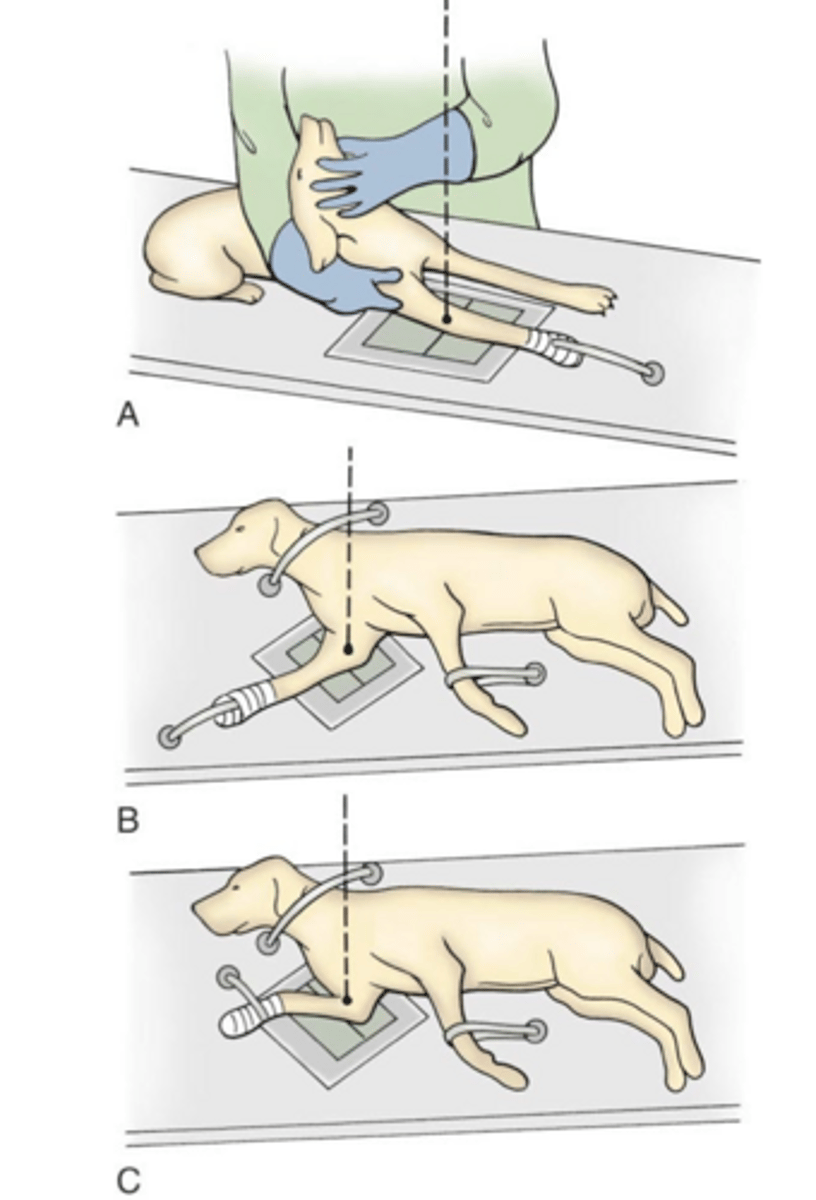
1. craniocaudal...as shown in A
2. standard lateral...as shown in B
3. flexed lateral...as shown in C
what positioning is involved in RADs for FCP
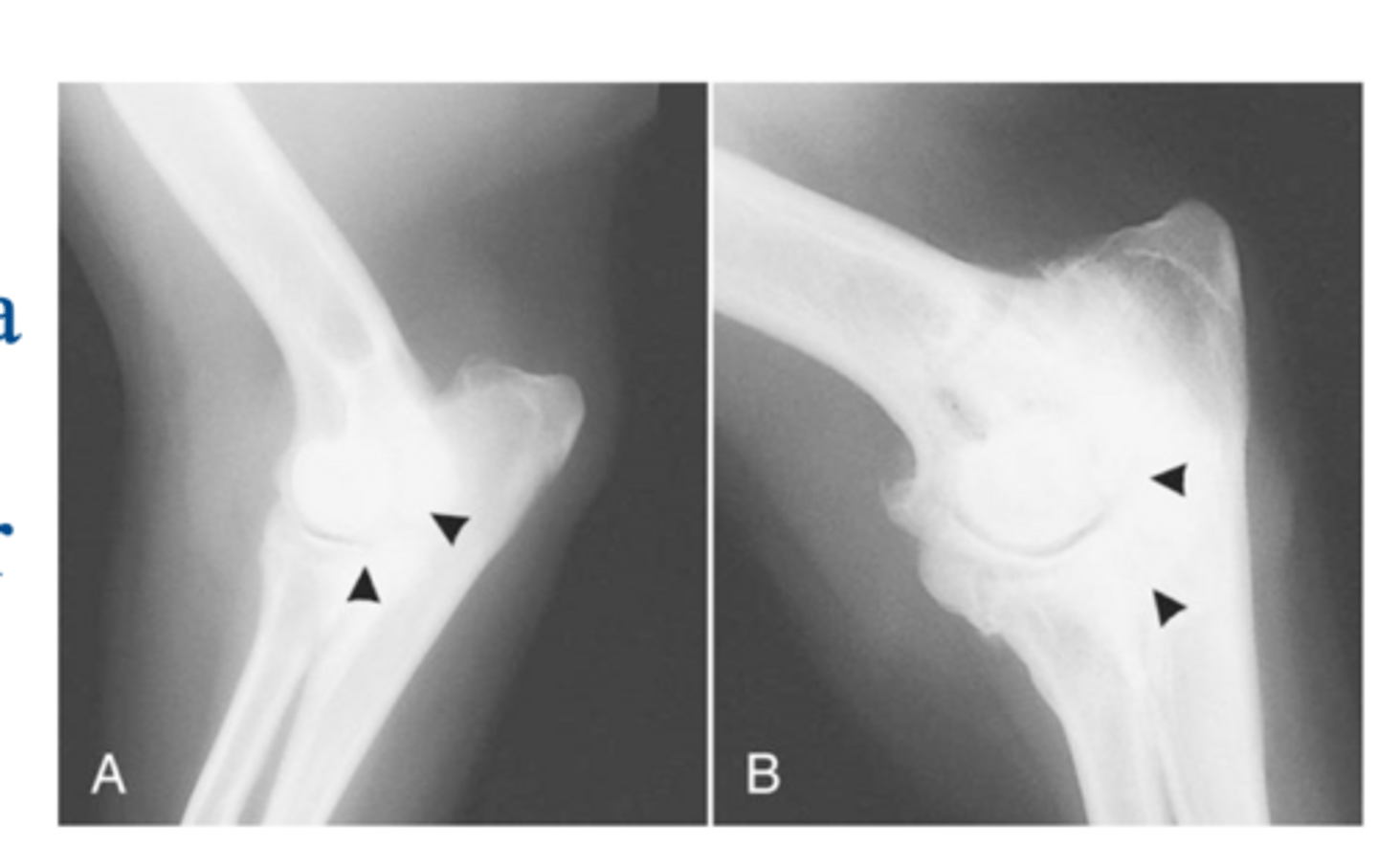
sclerosis of distal aspect of trochlear notch...visible loss of fine trabecular pattern & increased opacity
what is the earliest radiographic signs of FCP
blunting of medial coronoid process (MCP)
what is another early RAD finding during FCP
1. visible fragments rarely seen as changes are often subtle...occult elbow dysplasia even in presence of significant arthrosis
2. osteophytes w/ coronoid and anconeal processes
3. dx. made by presence of osteoarthritis
4. joint incongruence but can have high rates of false +/- for <3mm
key considerations for diagnostic imaging of FCP
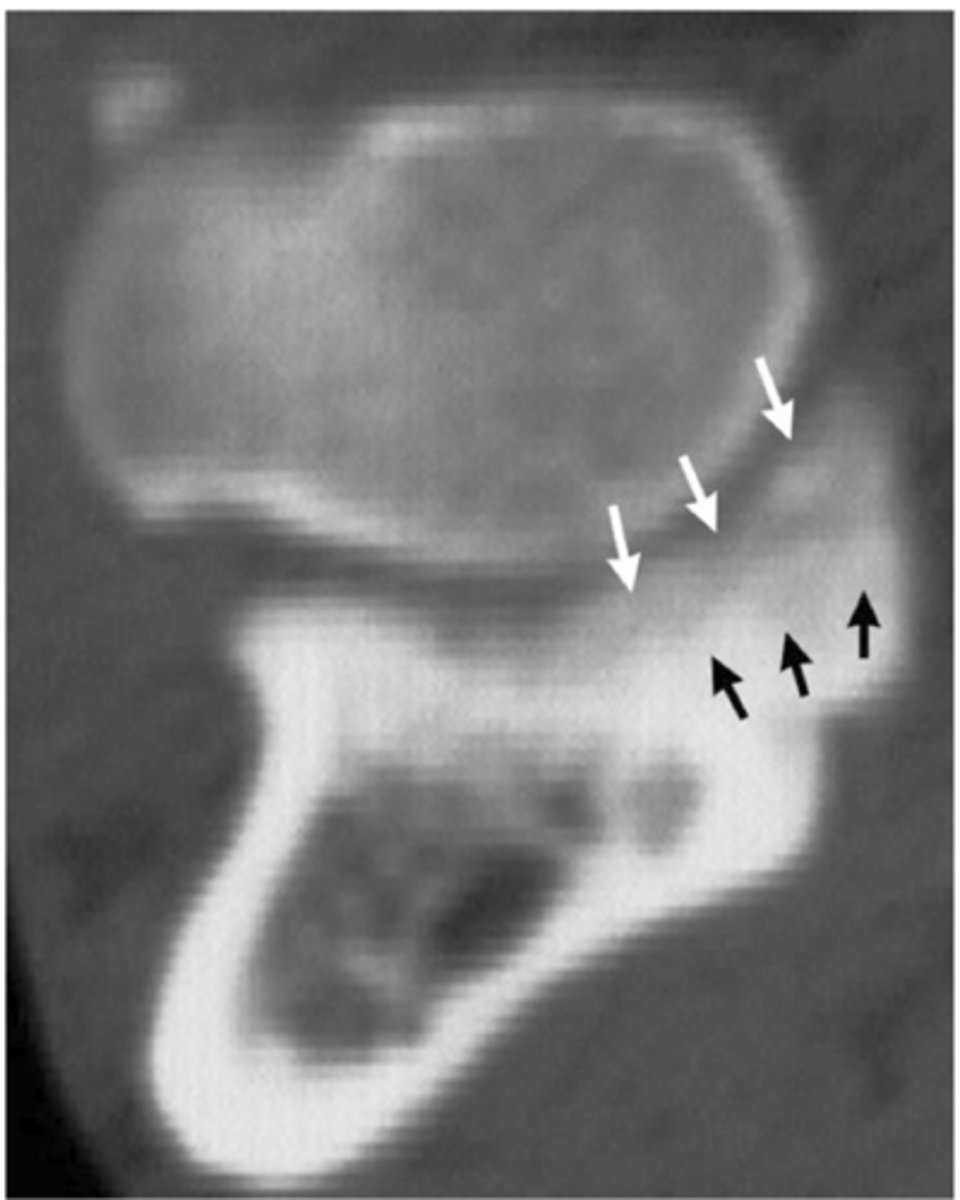
1. more accurate for identifying FCP than RADs
2. advantage over arthroscopy to dx. incomplete fragmentation og medial coronoid that doesn't reach cartilage surface
significance of FCP- computed tomography (CT)
CT showing osteomalacia of medial coronoid process associated with FCP
what is shown here
arthroscopy...allow direct visualization of cartilage surface
what is the most valuable tool for dx. FCP
1. strong evidence of hereditary component...FCP and OCD
2. always take RAD of both elbows due to high frequency of bilateral disease
3. sx. removal of bone and cartilage pieces may improve function of limb
4. sx. treatment will NOT alter progression of DJD/OA
5. dog may require medical therapy aft surgery if elbow is incongruent
6. dogs with OA of elbow will usually function well as pets but may not be working or competitive sporting dogs
what is some of the important information for clients with dogs that have elbow dysplasia
young dogs with intermittent or chronic lameness
what kind of FCP dog is the best candidate for surgery
arthroscopy or open arthrotomy
the basis of FCP tx. uses ____ for fragment removal
1. superior visualization and magnification of joint
2. less invasive
3. lower postoperative morbidity
4. provides greater opportunity for topical tx. of osteoarthritis lesions
what are the advantages of arthroscopic tx. FCP over open surgery
subtotal coronoidectomy
if arthroscopy or arthrotomy fails to demonstrate a fragment in FCP sx. a _____ can be performed if suspicious of incomplete fragment of coronoid
release of biceps insertion on ulna
what can be described as a treatment for FCP which can decrease transarticular forces btwn distal medial humeral condyle and medial coronoid process
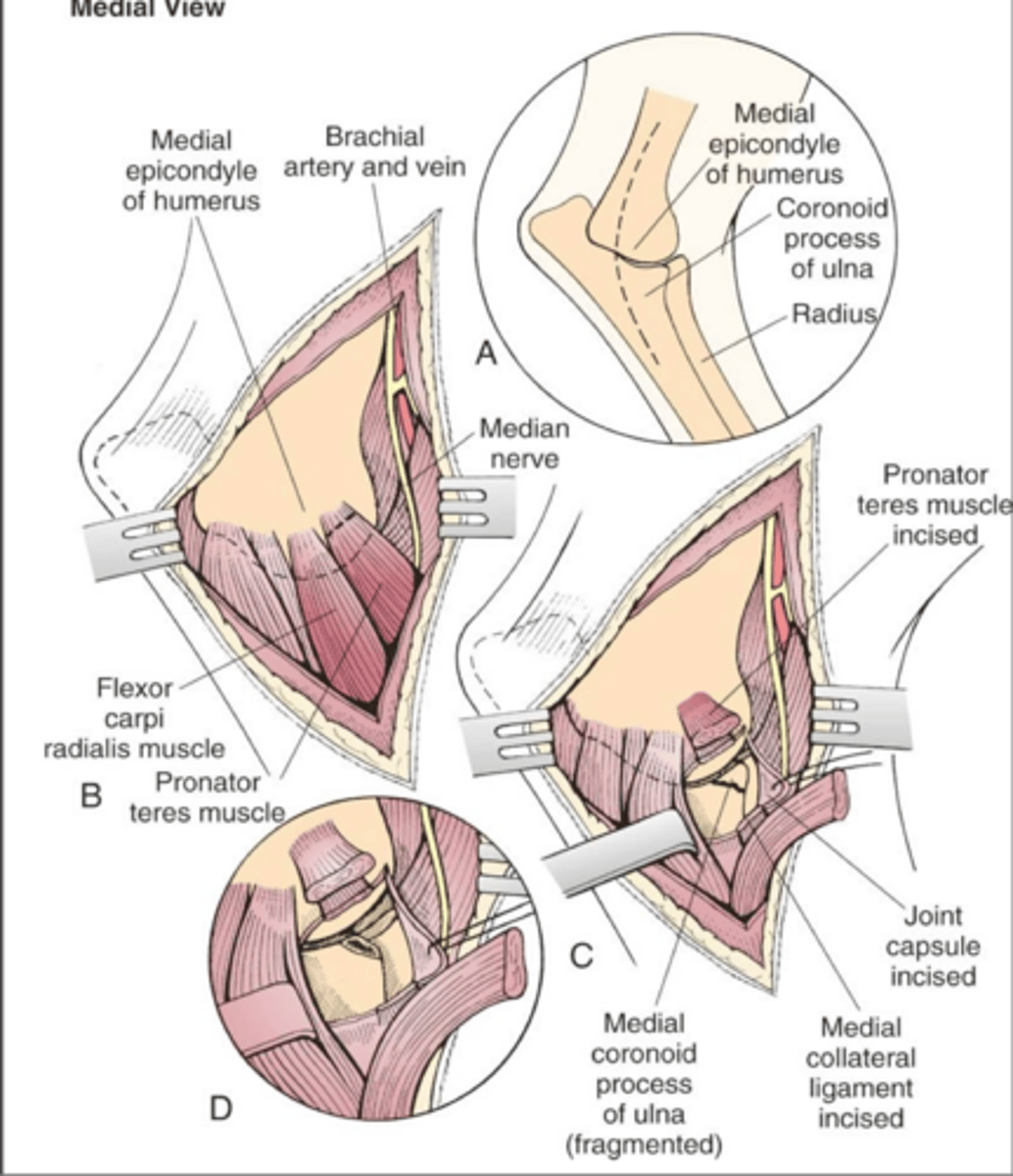
1. tenotomy of pronator teres m. and incising medial collateral ligament
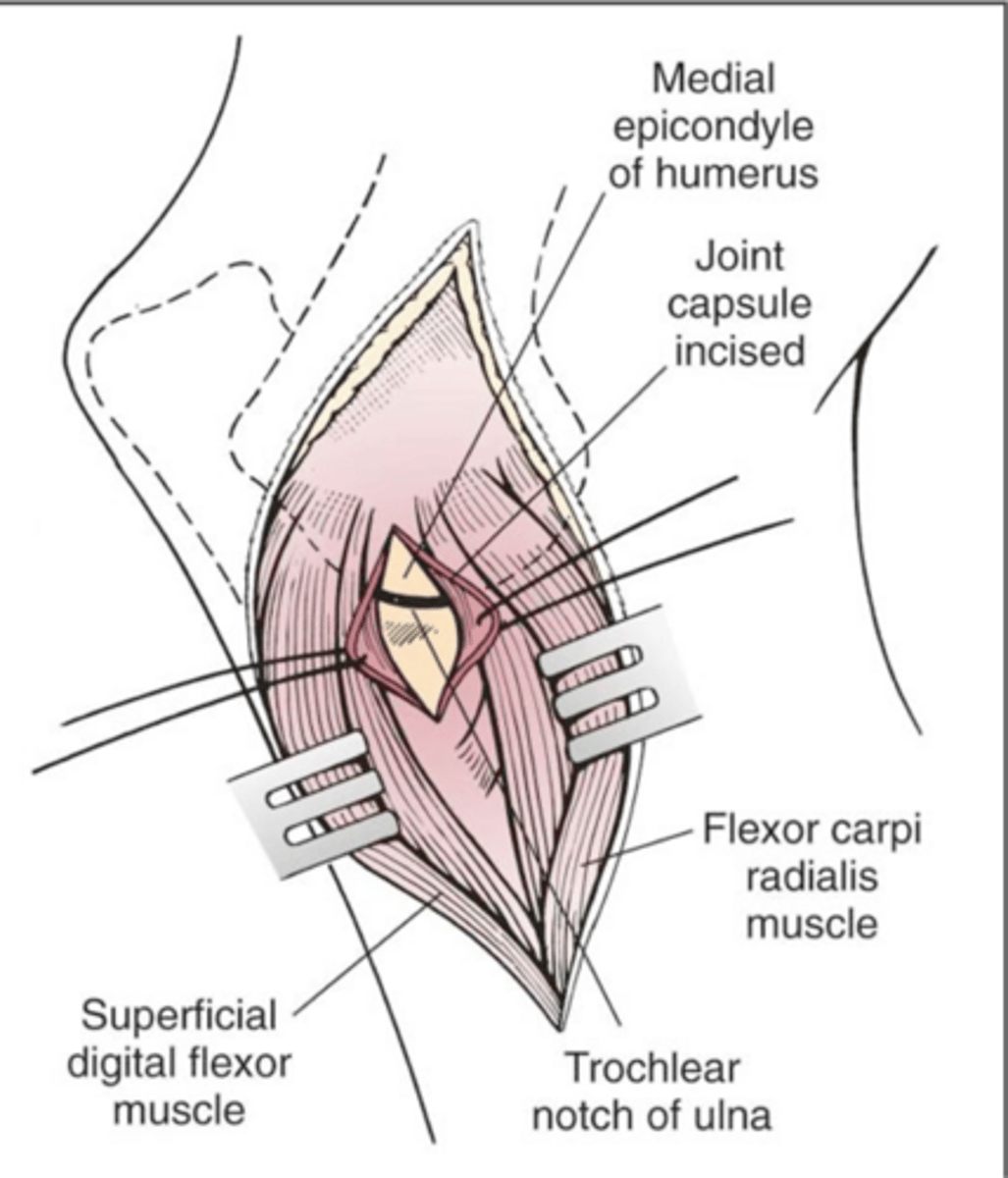
2. muscle-splitting technique...limits exposure
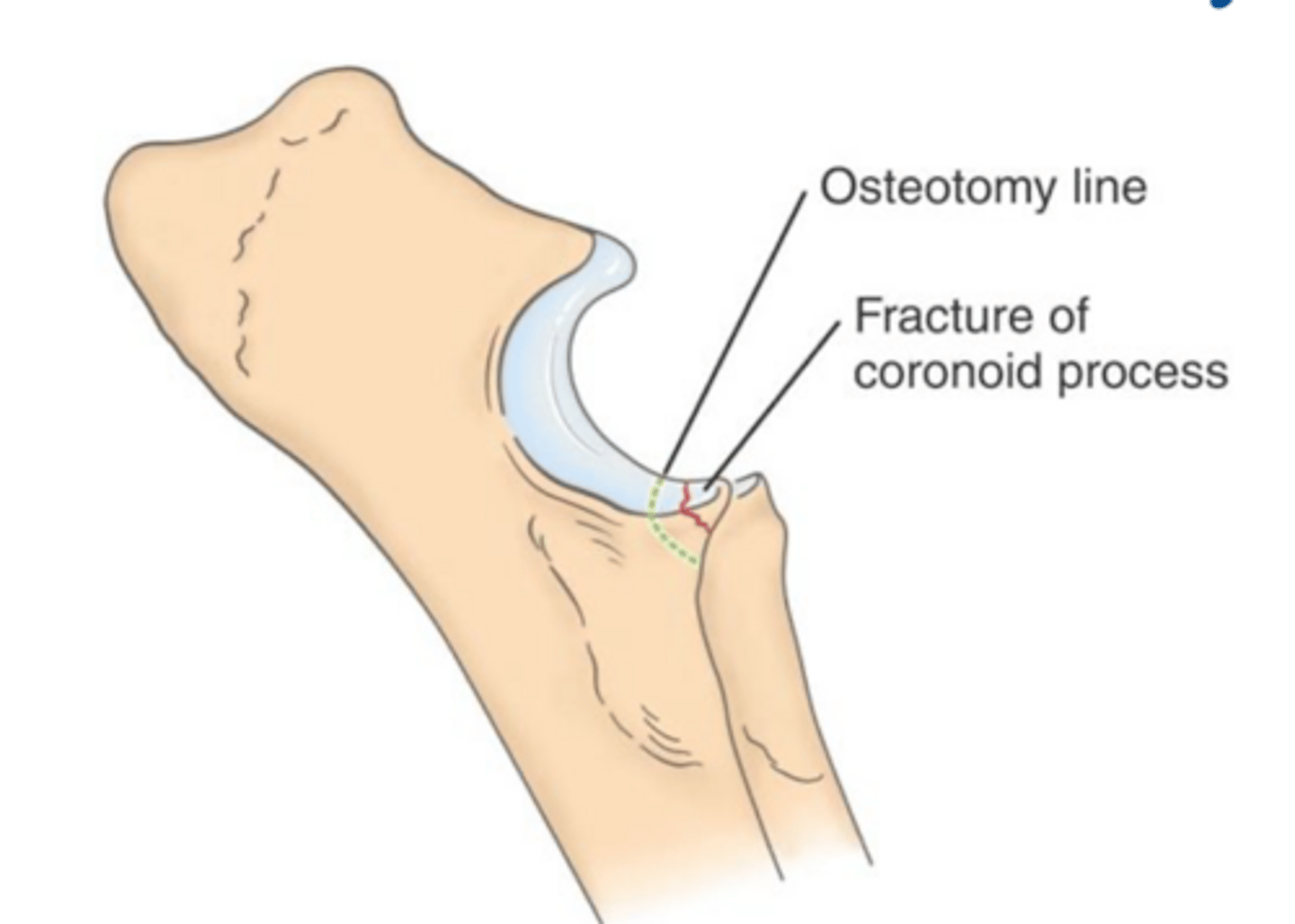
3. osteotomy of medial epicondyle provides best exposure but req lag screws
what are the techniques for open sx. of FCP to expose the medial coronoid process
transection of pronator teres muscle
what method of open FCP exposure is shown here
muscle splitting approach
what method of open FCP exposure is shown here
elevation of coronoid above level of radial head
how can we describe the condition of radial-ulnar incongruence (RUI)
radial-ulnar incongruence (RUI)
what is suggested as a cause of fragmentation of MCP and medial compartment disease
asynchronous growth between radius and ulna
______ in radial-ulnar incongruence (RUI) can cause increased forces across medial component and lead to bone fragmentation and cartilage damage
1. walk with shortened steps, decreased ROM, and pain on hyperextension of elbow
2. symmetrical or asymmetrical mm. atrophy
3. joint effusion and periarticular soft tissue swelling...felt when dog is standing
4. crepitation if advanced OA is present....manipulation painful
PE findings associated with radial ulnar incongruence
pain on hyperextension of elbow
what is often the earliest sign of radial ulnar incongruence
shoulder not flexed and extended during elbow manipulation
when performing a PE, what is key in order to prevent mistaking shoulder pain for elbow pain
plain film RADs or CT
what diagnostic modality do we use in radial ulnar incongruence to assess incongruence of the joint
proximal
in radial ulnar incongruence MCP will appear (proximal/distal) to the radial head
routine medial-lateral RADs
what view is inaccurate for dx. of mild incongruity in radial ulnar incongruence
flexed
radial ulnar incongruence is more accurately evaluated in (extended/flexed) lateral RAD views
CT
what is the more accurate way to evaluate incongruence in radial ulnar incongruence other than RADs
restoring normal congruence btwn proximal articular surfaces of radius and ulna by SHORTENING ULNA OR LENGTHENING RADIUS
proximal or distal ulnar segmental osteotomy
what does surgical tx. of radial ulnar incongruence involve
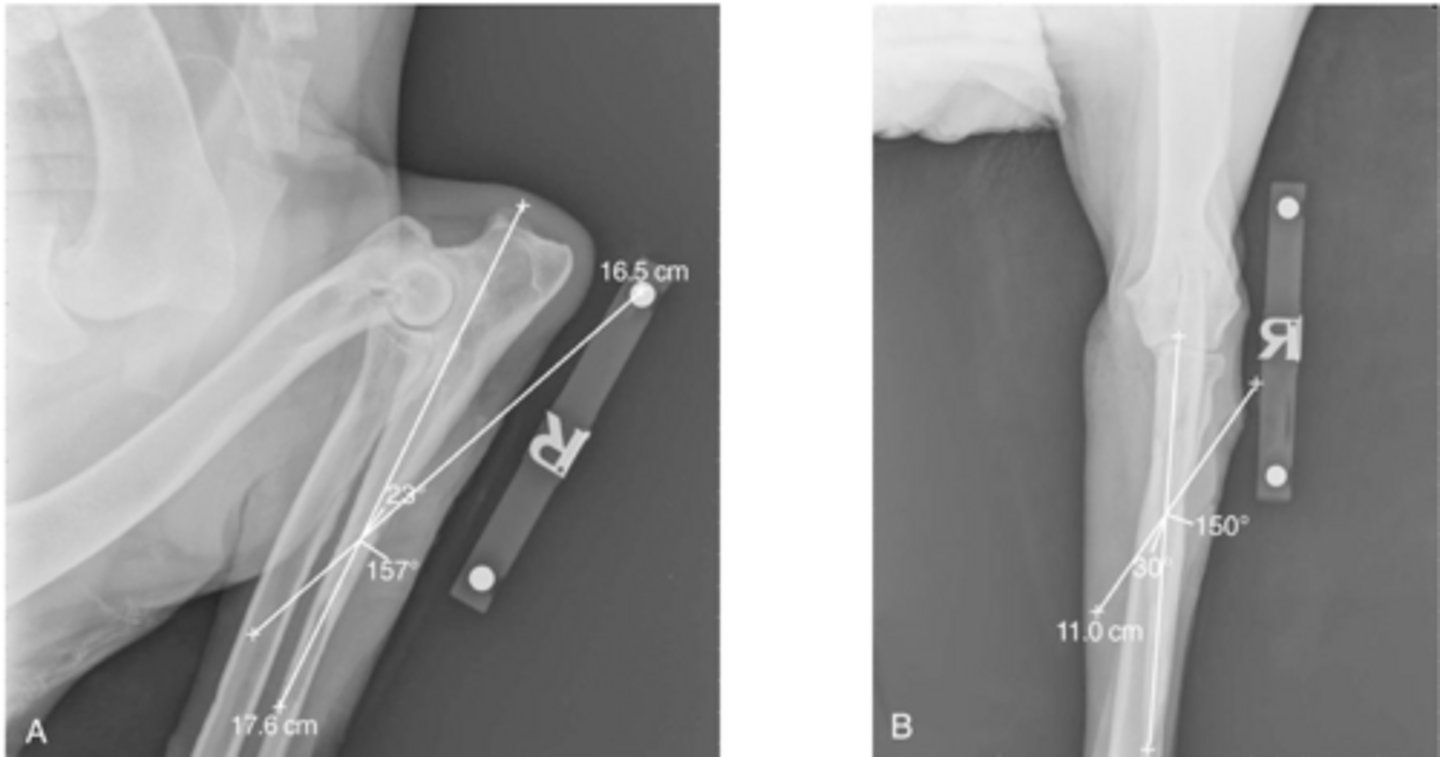
1. segmental osteotomy in proximal 1/3 of ulna removing about 1/2cm of bone
2. angle of osteotomy is caudal proximal to craniodorsal and craniolateral to caudomedial
what are the characteristics of a PROXIMAL ulnar segmental osteotomy to correct radial ulnar incongruence
1. 3 cm incision over lateral distal 1/3 of ulna ending at distal ulnar physis
2. expose the diaphysis of the ulna and isolate with Hohman retractors
3. remove 5mm length section of ulna
what are the characteristics of a DISTAL ulnar segmental osteotomy to correct radial ulnar incongruence
leading to significant hemorrhage
elevation of interosseous lig. of ulna aids in distal migration of ulna in distal ulnar segmental osteotomy but it runs the risk of...
mediolateral and craniocaudal RADs of osteotomy lines for PROXIMAL ulnar osteotomy
what is shown here
moderate to severe cartilage erosion on medial aspect of canine elbow joint
what does medial compartment disease (MCD) refer to
1. medial portion of coronoid process
2. medial distal aspect of humeral condyle
3. medial most portion of radial head...in some cases
what regions are commonly affected by medial compartment disease (MCD)
mechanical overload or incongruity of elbow joint
though the etiology of medial compartment disease (MCD) is unknown, it is most likely caused by...
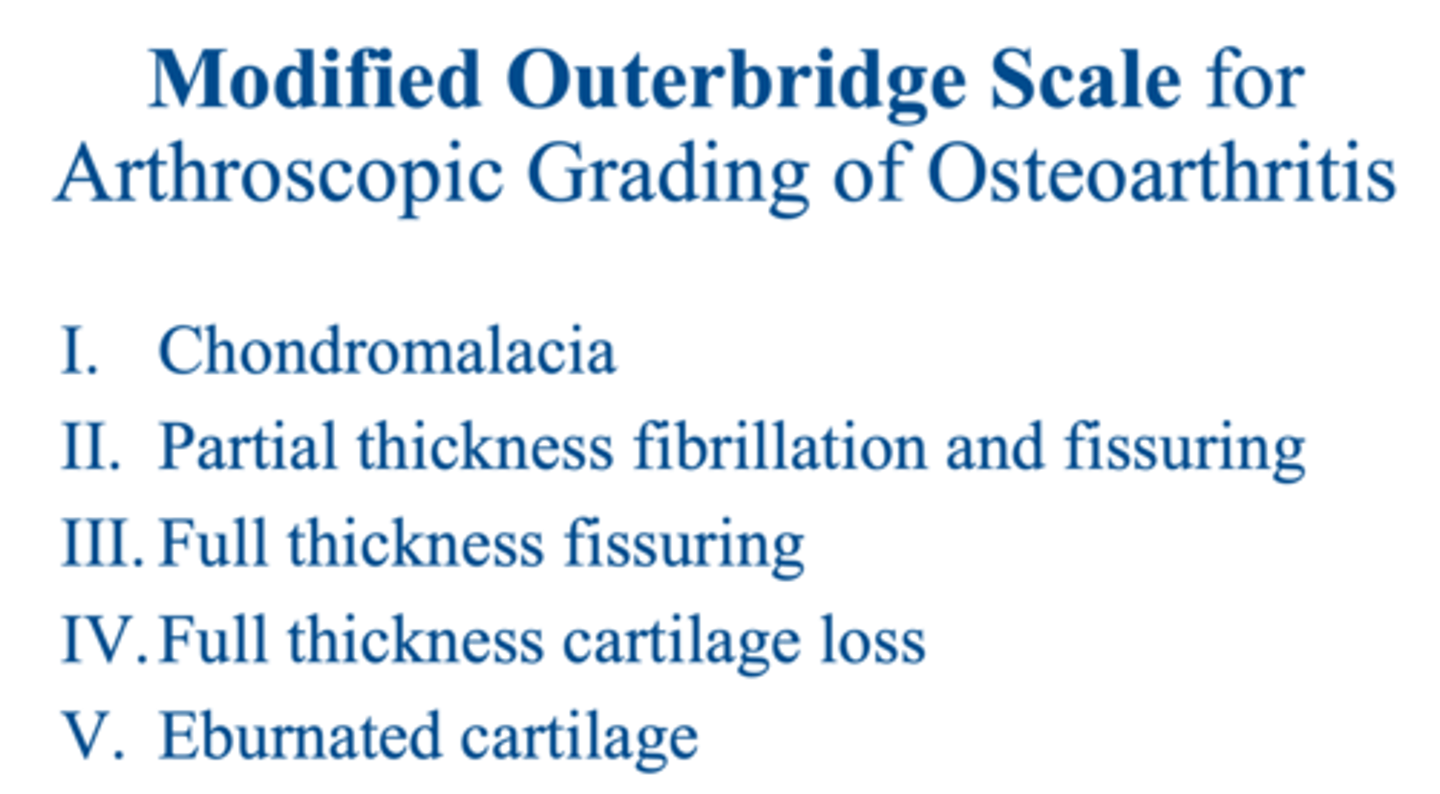
modified outerbridge scale
how do we grade severity of cartilage loss in medial compartment disease (MCD) cases
1. large breed dogs usually affected but can be dx. in any size dog
2. age of onset and disease process is unknown but can be dx. anywhere from 6 months old-several years old
signalment of medial compartment disease (MCD)
1. walk with shortened steps, decreased ROM
2. symmetrical or asymmetrical mm. atrophy
3. joint effusion and periarticular soft tissue swelling...felt when dog is standing
4. manipulation painful
5. bilateral lameness of forelimbs
what are some notable PE findings associated with medial compartment disease (MCD)
severe cartilage damage may be present w/ minimal RAD changes
medial compartment disease (MCD) is dx. by radiographic signs of DJD but but it is important to note that...
arthroscopy
what is the most definitive tool to dx. medial compartment disease (MCD) as it enables direct visualization of the cartilage and is a less invasive exam that is far superior to open surgery
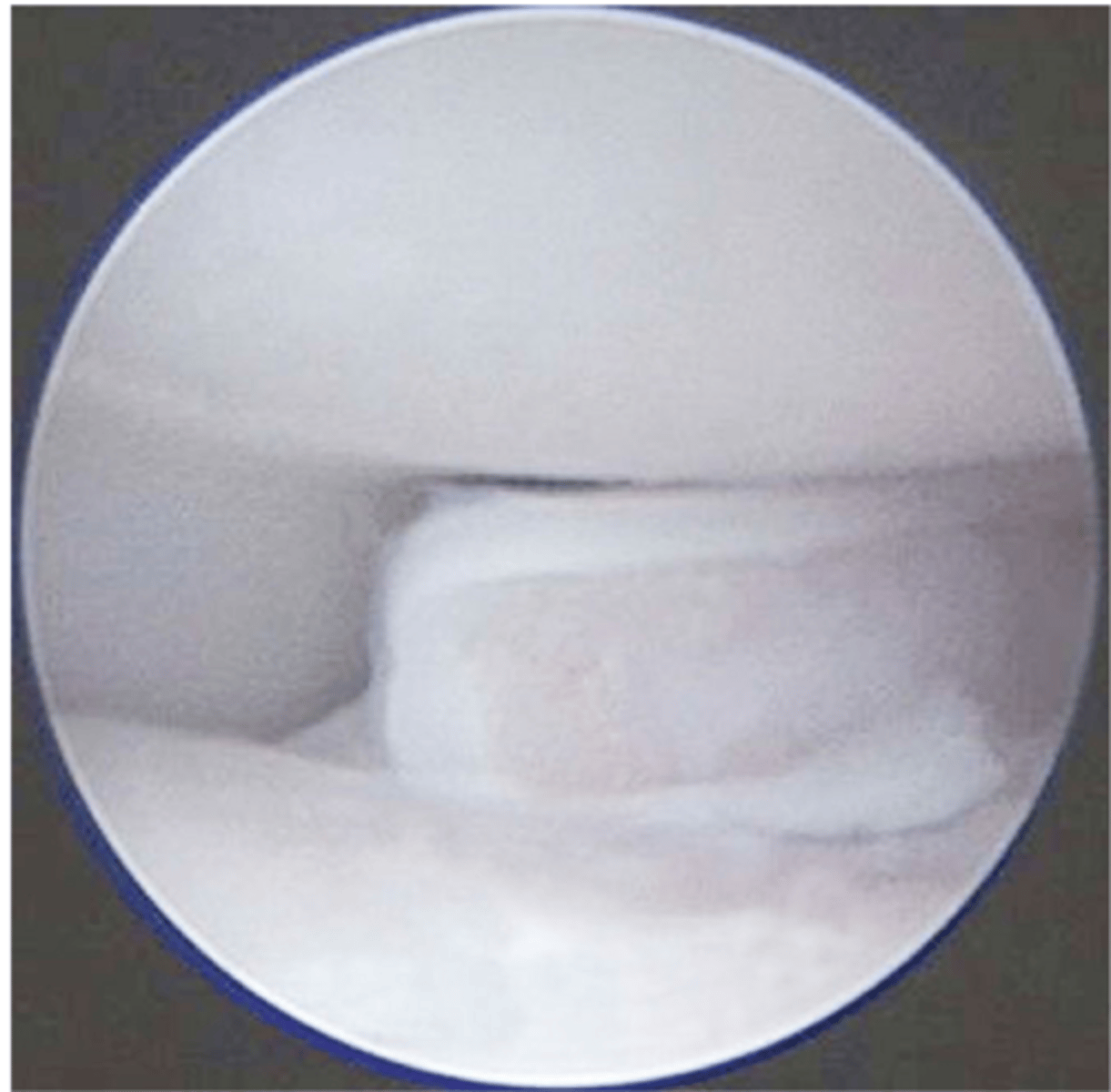
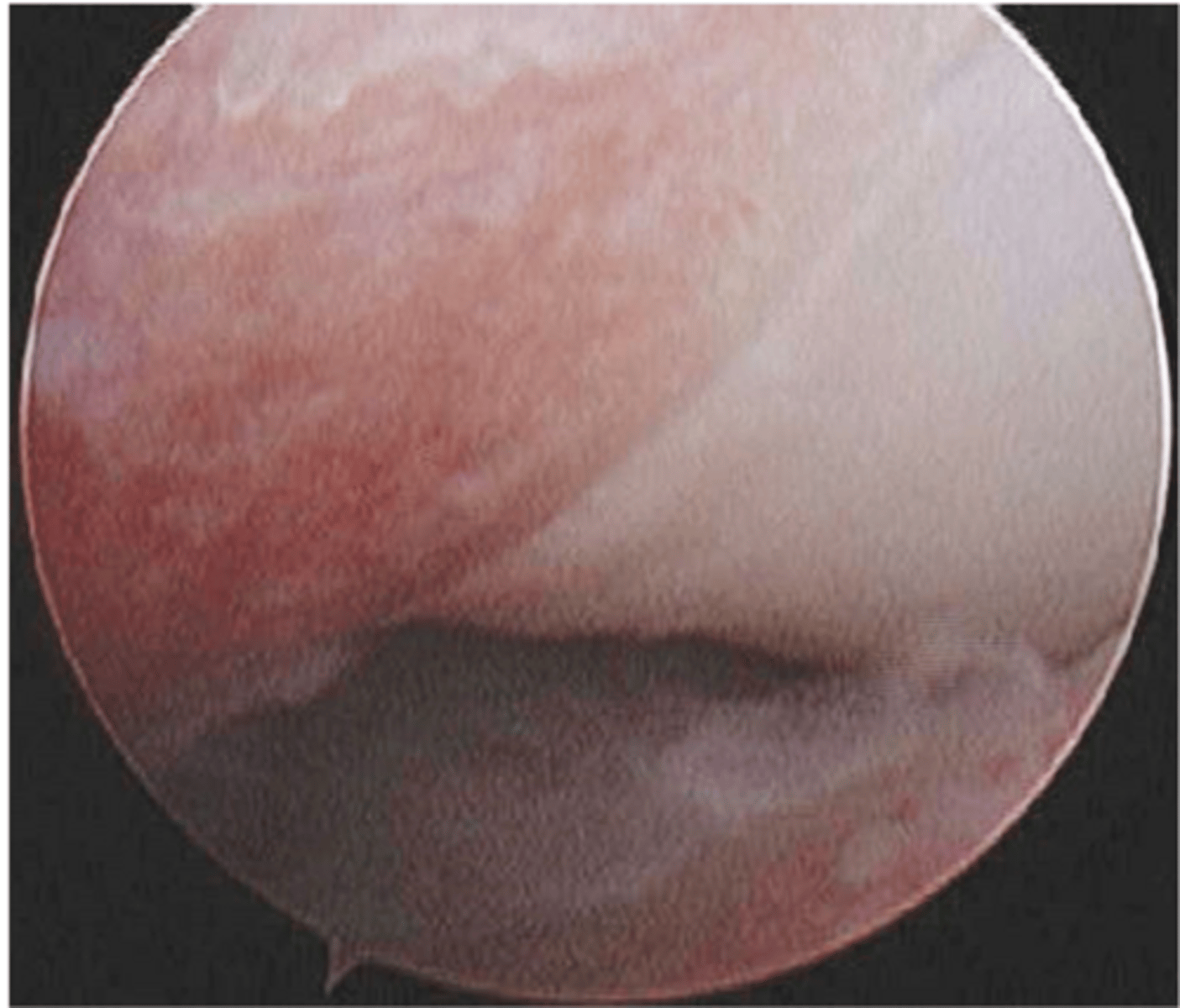
arthroscopic view of MCD w/ full thickness (grade IV) cartilage damage
what is shown here
questionable
though many patients w/ MCD also have FCP, fragment removal alone is (questionable/encouraged)
create channels for revascularization of arthritic lesion from bone marrow...may aid in recruiting stem cells
what is the goal of microfracture and abrasion arthroplasty in MCD sx.
mechanical forces that led to cartilage erosion also prevent healing of cartilage lesion
why is microfracture and abrasion arthroplasty in MCD sx. likely of limited benefit
1. decrease pain and joint inflammation by decreasing stimulation of nerve endings in subchondral bone
2. removal of coronoid...subtotal coronoidectomy
3. decreasing transarticular load via procedure like segmental ulnar osteotomy
4. total elbow replacement
what are some other surgical tx. options for MCD other than microfracture and abrasion arthroplasty
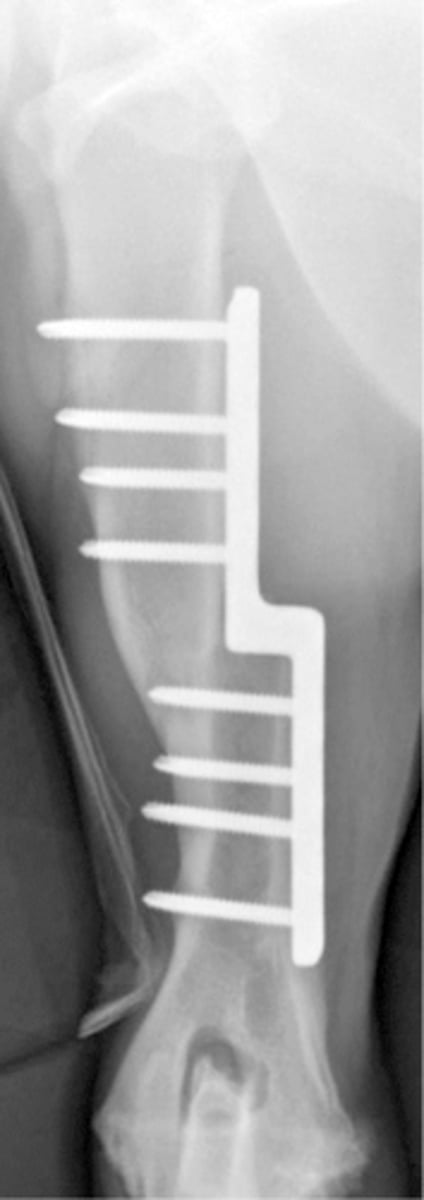
post-op RAD of sliding humeral osteotomy to tx. MCD
what is shown here
biceps exerts significant proximal forces on radius and ulna and release can decrease transarticular forces and aid in healing
why can release of biceps insertion on ulna be a beneficial sx. tx. of MCD
most of the procedures have NOT been evaluated for efficacy
in terms of most MCD procedures and their efficacy...