Oral Path Ex 1
1/256
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
257 Terms
total lack of tooth development (don’t say partial!)
anodontia
lack of developmenent of many teeth (6+ teeth)
oligodontia
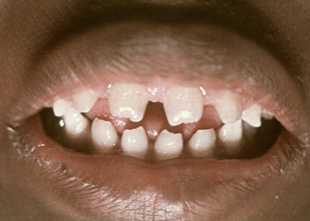
missing 1-5 teeth; ectodermal dysplasia
hypodontia
development of an increased number of teeth (supernumerary); cleidocranial dysplasia and gardenr syndrome
hyperdontia

inherited condition in which 2 or more ectodermally derived structure fail to develop (e.g skin, hair nail, teeth, sweat glands); AD, AR, X-linked; decreased # of teeth, Per > Dec
hypohydrotic ectodermal dysplasia

most commonly occurs max incisors
mesiodens

accessory 4th molar
distomolar

situated lingually or buccally to a molar
paramolar
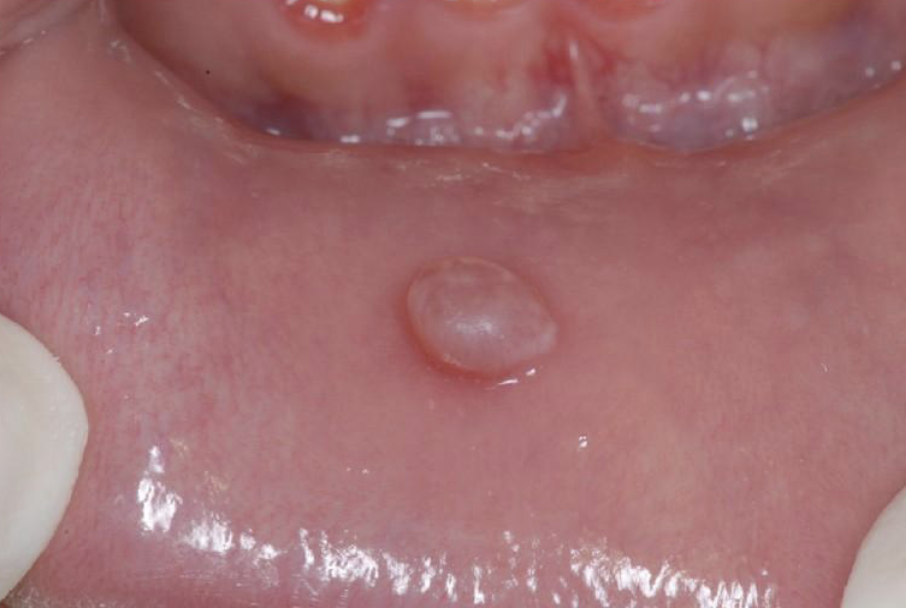
teeth present at birth
natal teeth
present within the first 30 days
neonatal
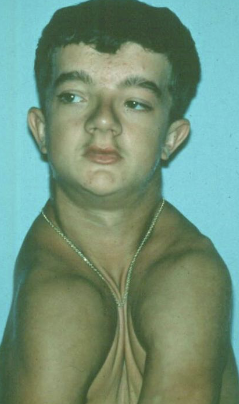
syndrome characterized by dental and clavicle abnormalities, AD inheritance, prolonged retention of deciduous teeth, numerous unerupted permanent and supernumerary teeth
cleidocranial dysplasia
AD syndrome with clinical features of colorectal (adenoma) poly that can become malignant (100% if untx), multiple osteoma, 20% have supernumerary teeth. pigmentation ocular fundus (90%)
gardner syndrome

gardner syndrome
Which of the following clinical/ oral manifestations is correctly matched with its associated syndrome?
missing clavicles - cleidocranial dysplasia

found in gardner syndrome (20%) and cleidocranial dysplasia (more common)
hyperdontia (supernumerary teeth)

small tooth size, often associated with hypodontia, small lateral incisor = peg lateral
microdontia
microdontia is associated with __ and __
down syndrome and hypopituitarisim (dwarfisim)
large teeth, isolated is more common, usually incisors and canines (can be bilateral)
macrodontia
generalized macrodontia is rare but may be associated with which systemic conditions?
pituitary gigantism, hemifacial hyperplasia, otodental syndrome (globodontia), XXY males (klinefelter)

single enlarged/ double/ jointed tooth in which the tooth count is normal (NO MISSING TEETH); one tooth bud tried to divide
gemination

defined as a single/ enlarged/ double/ joined tooth in which the tooth count reveals a MISSING tooth; two buds tried to join
fusion
union of two teeth by cementum alone
concrescence
2 teeth joined
fusion
one tooth trying to split
gemination

accessory cusp on palatal surface of ML cusp of maxillary molars
cusp of carabelli
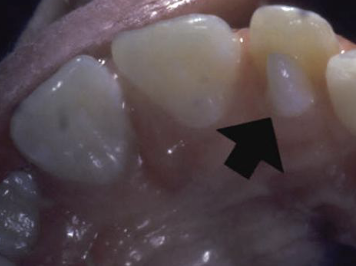
accessory cusp of lingual incisor, usually, max lat incisor, 91% in max, usually has pulp tissue inside
talon cusp
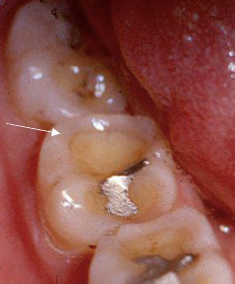
elongated “cusp” extending from central occlusal surface, mand premolars/ maybe molars, usually has pulp tissue, occlusal trauma is a problem
dens evaginatus (occlusal pearl)

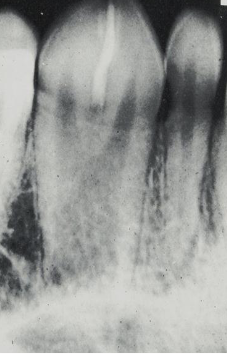
deep surface enamel invagination of the crown or root “tooth within tooth”; can be coronal (most frequent) or radicular
dens invaginatus “dens in dente”
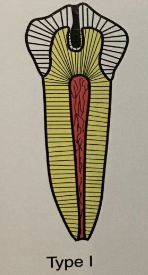
“dens in dente” type I
invagination is confined to the crown
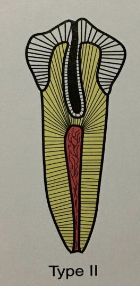
“dens in dente” type II
invagination extends below the CEJ
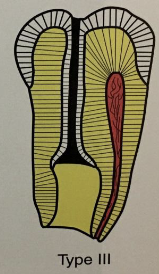
“dens in dente” type III
invagination may extend through the root

prominent marginal ridges on max incisors (esp centrals), associated w/ dens evaginatus, usually bilateral, most common in asians
shovel shaped teeth

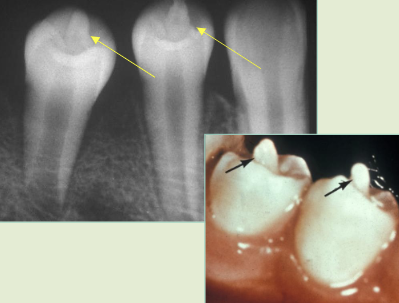
enamel nodules at furcation of multi-rooted teeth, most common in max molars, may have pulp tissue usually without dentin
enamel pearl

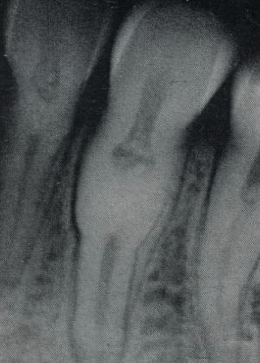
enlargement of the body and pulp chamber, most common in mand molars/ premolars, no tx necessary
taurodontism

from traume or infection of tooth bud as root is forming, tooth vital, usually 3rd problems, no problem with tooth unless endo is needed
dilaceration

mostly affect mandibular molars followed by 2nd premolars, can be caused by local factors or systemic factors
hypercementosis
Local factors of hypercementosis (localized)
abnormal occlusal trauma, adjacent inflammation, unopposed teeth (super eruption), repair of vital root fracture
Systemic factors of hypercementosis (generalized)
acromeagaly and pituitary gigantism, arthritis, calcinosis, paget disease of bone, rhumatic fever, thyroid goiter, gardner syndrome, vit A deficiency

increase number of roots, both dec & perm, most commonly affect man 3rd molar > cuspids and bicuspids, no tx but detection important if endo needed
supernumerary root
Which feature correctly matches its diagnosis?
enlarged pulp chamber -taurodontism
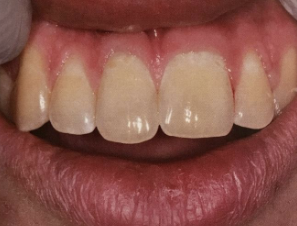
AD, AR, X-linked; both deciduous and permanent dentition are diffusely involved, affects enamel (soft, thin, easily damaged, susceptible to decay), dentin is exposed
amelogenesis imperfecta (AI)
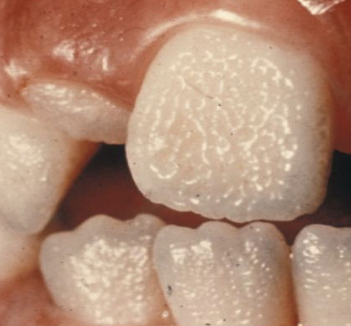
Types of AI
hypoplastic (pitted), hypomaturation/ hypocalcification (snowcapped) AI with taurodontism

what type of AI
hypomaturation (snowcapped)
what type of AI?
hypoplastic (pitted)
Clinical appearance of AI
yellow-brown to white pitted lesions, open bite, loss of contact
types of enamel dysplasia (ED)
hypoplasia and hypomineralization
thickness deficit, quantitative defect (incomplete enamel matrix formation )
hypoplasia ED
mineral deficit, qualitative defect
hypomineraliszation ED
hypomineralization ED can be classified as either
hypomaturation (amelogenin-rich) or hypocalcification (amelogenin- poor)
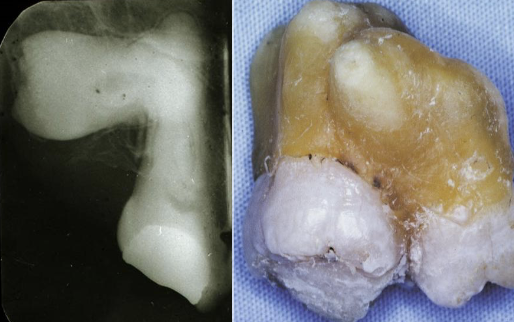
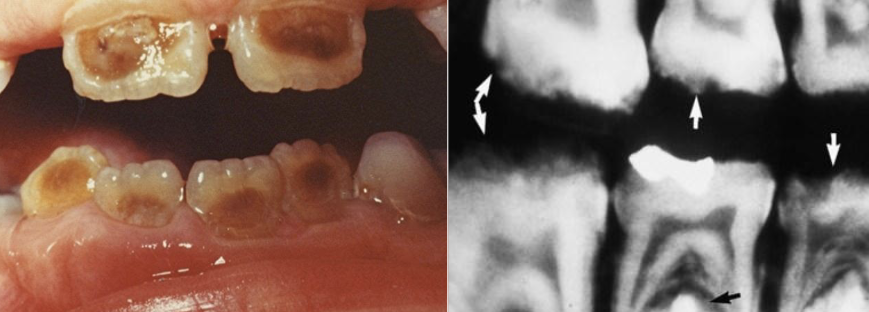
a hereditary condition of dentin in the absence of any systemic disease (opalescent dentin), AD, genetic mutation is DIFFERENT from osteogenesis imperfecta
dentinogenesis imperfects (DGI)
DGI-I clinical presentation
ostoegenesis imperfecta (for boards), opalescent teeth, BONE FRACTURES
DGI-II clinical presentation
isolated opalescent teeth, most common
DGI-III
isolated opalescent teeth, large pulp = shell teeth, pulp exposure, PA radiolucencies
DGI-I witkop classification
dentinogenesis imperfecta
DGI-II witkop classification
hereditary opalescent teeth
DGI-III witkop classification
brandywine

affects both dentition, steel-grey/ translucent/ opalescent crowns, brittle enamel
DGI

DGI radiographic presentation
bulbous crown, cervical constriction, pulp obliteration varies, expanded pulp = shell teeth
hereditary condition affecting dentin, AD, both dentitions affected, 2-types (coronal and radicular)
dentin dysplasia (DD)

DD-II
coronal dentin dysplasia

DD-I
radicular dentin dysplasia

4 types, normal clinical crown, short roots, periapical radiolucencies, chevron pulp chambers
DD-I

have a blue-amber-brown translucence, bulbous crown, cervical constriction, thin roots, normal length, early obliteration of pulp
DD-II primary teeth
have a normal color clinically, pulp chamber is enlarged = thistle tube or flame shaped, pulp stone, normal root
DD-II permanent teeth
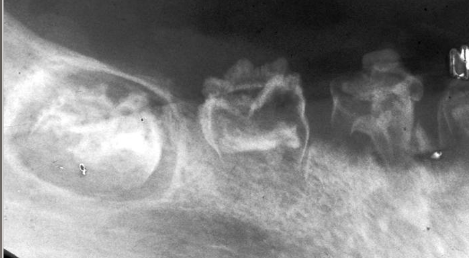
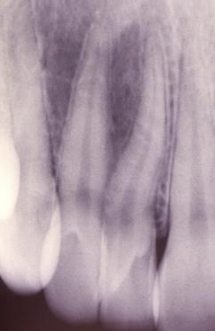
nonhereditary developmental anomaly, most common in max ant teeth, usually involves one quadrant, very large pulps with minimal dentin and enamel
regional odontodysplasia “ghost teeth”
Which feature correctly matches its diagnosis?
opalescent dentin - dentinogenesis imperfecta

tooth-tooth
attrition

tooth-abrasive (mechanical)
abrasion
chemical
erosion

occlusal stress
abfraction
common in apical/ mid root; associated with cysts, tumors, ortho, excessive occlusal stress, reimplantation of avulsed tooth
external resorption

rare, injury to pulpal tissue (trauma)
internal resorption

internal resorption affecting crown
pink tooth of mummery

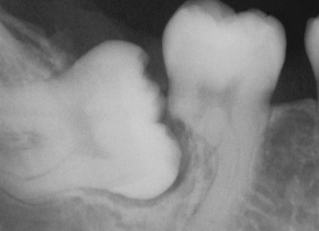
obstructed by a physical barrier, lack of eruptive force = embedded, rarely occurs in deciduous teeth
impaction localized disturbance in eruption

cessation of eruption after emergence, fusion of cementum with bone, unknown pathogenesis
ankylosis localized disturbance in eruption

enamel can be white, yellow, brown, and or have different degrees of hypoplasia; most commonly in bicuspid because of their relation ship with the deciduous molars; causes fever, PA inflammatory disease of overlying deciduous tooth, trauma
turner’s hypoplasia

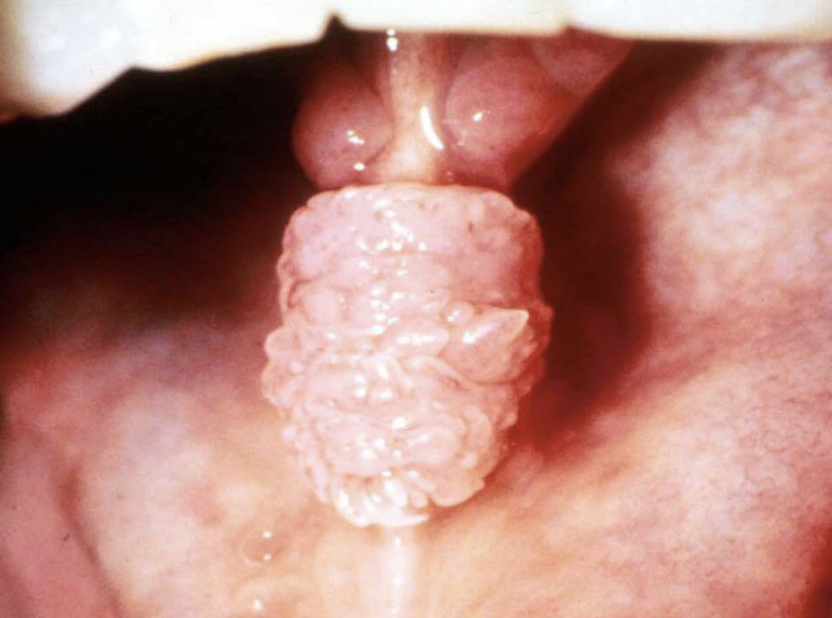
intra-oral presentation of congenital syphilis;1st molars develop irregular nodules of enamel on occlusal surface
mulberry molars
intra-oral presentation of congenital syphilis; “screwdriver” incisor
hutchinson’s incisor
H & N effects of congenital syphilis
mental degeneration, cartilage, septal destruction of nose (saddle nose), blindness, deafness (CN 8)

ingestion of excess amount of fluoride, retention of amelogenin protein in enamel, hypomineralization creating chalky white areas, must be bilateral symmetrical distribution with previous exposure to Fl
fluorosis, mottled enamel

pulp death after RCT or trauma, age (gets darker with time), tooth is brittle, rx post and crown
non-vital tooth

rare, injury to pulpal tissue
internal resorption

from use during tooth development; may also discolor skin, sclera, thyroid; RX for acne, cystic fibrosis, RA
tetracycline staining

What is the cause?
tooth-tooth contact
which feature correctly matches its diagnosis
discolored enamel defect - turner’s hypoplasia
All of the following are local factors causing hypercementosis EXCEPT
paget disease
A single enlarged tooth in which the tooth count is normal and tooth bud tried to divide
gemination

what is the dx?
dense invaginatus
Which of the following is not a hereditary condition?
regional odontodysplasia

what is the diagnosis?
regional odontodysplasia
most common teeth to express turner’s hypoplasia
bicuspids

what is the cause of this lesion
trauma to the pulp
which medication can cause bluish staining of teeth?
tetracycline
which is NOT a feature of congenital syphillis?
5th nerve deafness (it’s 8th)
Base of Lesion : flat base
sessile

Base of Lesion : between sessile and pedunculated
polypoid
Base of Lesion : stalk like
pedunculated

Surface Texture : wrinkled
corrugated

Surface Texture : a cleft or groove, normal or otherwise, show prominent depth
fissure

Surface Texture : resembling small projection or elevation found in clusters
papillary