Vet tech prep power pages: surgical nursing review
1/271
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
272 Terms
The kidney is resoponsible for
regulating water and electrolyte balance in the body
the kidney maintains
acid-base homeostasis
the kidney aids in retaining
protein and glucose in the body
the kidney excretes
waste and toxins
the kidney plays a role in many
endocrine functions by secreting hormones
renal refers to the
kidneys
acid (kidney)
a substance that releases hydrogen ions in solution (pH <7).
base (kidney)
a substance that accepts hydrogen ions in solution (pH >7).
Nephron
functional unit of the kidney
renin
hormone secreted by the kidney;
-mediates extracellular volume and arterial vasoconstriction (regulates blood pressure) via the renin-angiotensin system
Aldosterone stimulates
active sodium reabsorption
antidiuretic hormone (ADH) stimulates
passive water reabsorption
the kidney is made up of
nephrons
The nephron is the
functional unit of the kidney
The nephron is made up of
the glomerulus
the glomerulus is surrounded by
Bowman's capsule and its tubule
The tubule is sectioned into the
proximal tubule, the medullary loop of henle, and the distal tubule which empties into the collecting duct.
Filtration in the kidneys happens through the
glomerular capillaries.
the filtration inside the glomerular capillaries is driven by
hydrostatic pressure as a direct result of arterial pressure.
Glomerular Filtration Rate (GFR)
the rate at which filtration through the glomerular capillaries occurs
The loop of henle is resposible for
concentrating the urine
what is resorbed at the loop of henle
sodium and chloride
The final urine concentration is dependent upon the
amount of antidiuretic hormone secreted by the pituitary gland
The proximal tubule resorbs
all glucose and amino acids, and most bicarbonate, phosphate, and water.
Renin increases the production of
Angiotensin II
Renin is released in response to
intravascular volume drops (dehydration, blood loss)
renin release causes then causes aldosterone release from
the adrenal cortex
renin release also causes increased release of
ADH from the posterior pituitary causing increased thirst, and constriction of the efferent arteriole to maintain GFR. In fluid overload, the opposite occurs.
Aldosterone causes
sodium and water resorption in the distal tubule and collecting duct
in the distal tubule and collecting duct
sodium is exchanged for potassium and hydrogen
what is released when sodium is low in the blood
aldosterone
examples of sodium loss
Vomiting or loss of gastric acids
sodium loss leads to
alkalosis
Antidiuretic hormone makes the
distal tube and collecting duct more permeable to water, which increases urine concentration
When antidiuretic hormone (ADH) is present
the urine is concentrated
When antidiuretic hormone (ADH)is not present
Nerve impulses from the hypothalamus stimulate
the pituitary to make ADH when osmotic blood pressure rises.
Vitamin D (calcitriol) is produced by the
to help promote calcium absorption from the intestine
the kidney also produces erythropoietin which
stimulates production of red blood cells.
Kidney values on a blood panel
BUN and creatinine
Amylase is excreted through
the kidneys
if renal function is impaired, amylase
rises
important factors on kidney function besides BUN/creatine is
UA and electrolyte values
How many cranial nerves are there?
12
cranial nerve diagram
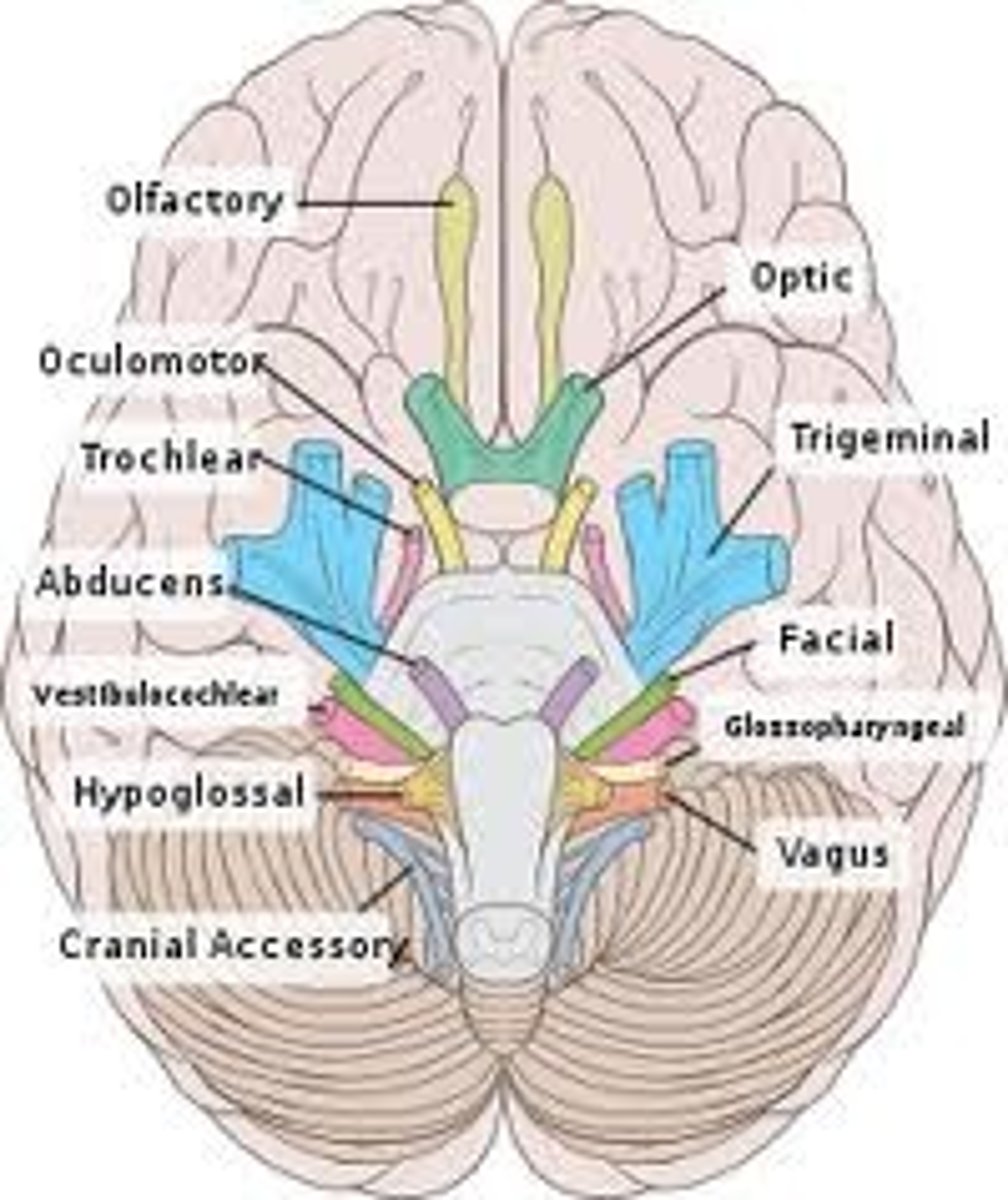
CN 1
Olfactory nerve
CN 1- olfactory
Mediates the sense of smell, observed when the pet sniffs around its environment
CN 2
Optic
CN 2- Optic
Carries visual signals from retina to occipital lobe of brain, observed as the pet tracks an object with its eyes. It also causes pupil constriction.
The Menace response
is the waving of the hand at the dog's eye to see if it blinks (this nerve provides the vision; the blink is due to cranial nerve VII)
CN III
oculomotor nerve
CN III - Oculomotor Nerve
• Provides motor to most of the extraocular muscles (dorsal, ventral, and medial rectus) and for pupil constriction o Observing pupillary constriction in PLR
CN IV (4)
trochlear nerve
CN IV (4)- Trochlear Nerve
Provides motor function to the dorsal oblique extraocular muscle and rolls globe medially
CN V (5)
Trigeminal Nerve - Maxillary, Mandibular, and Ophthalmic Branches
CN V (5)- Trigeminal Nerve - Maxillary, Mandibular, and Ophthalmic Branches
• Provides motor to muscles of mastication (chewing muscles) and sensory to eyelids, cornea, tongue, nasal mucosa and mouth.
CN VI (6)
abducens nerve
CN VI (6)- Abducens Nerve
• Provides motor function to the lateral rectus extraocular muscle and retractor bulb
CN VI (6)- Abducens Nerve is tested by
touching the globe and observing for retraction (also tests V for sensory) Responsible for physiologic nystagmus when turning head (also involves III, IV, and VIII)
CN VII (7) facial nerve
• Provides motor to muscles of facial expression (eyelids,ears,lips) and sensory to medial pinna(ear flap). Also taste to rostral tongue
CN VII (7)
facial nerve
CN VII (7) facial nerve helps with
tear production (schirmer tear test)
CN VII (7) facial nerve- Palpebral response
-motor for the blink reflex when touching medial canthus (also tests V for sensory)
can observe for facial paralysis by
CN VII (7) facial nerve
symptoms: deviation of nose to one side or droopy lips
CN VIII (8)
vestibulocochlear nerve
CN VIII (8) -vestibulocochlear nerve
Sensory for hearing and head position
A head tilt or nystagmus may suggest dysfunction of
CN VIII (8)- Vestibulocochlear Nerve (vestibular disease or inner ear disease)
CN IX (9)
Glossopharyngeal nerve
CN IX (9)- Glossopharyngeal Nerve
•Innervates the pharynx for swallowing (with X).
-Also innervates some salivary glands and provides taste innervation from caudal tongue
examine the CN IX (9) - Glossopharyngeal Nerve by
eliciting a gag reflex and observing for dysphagia (difficulty swallowing)
CN X (10)
vagus nerve
CN X (10) - Vagus Nerve
•Innervates the larynx, esophagus, and pharynx. Also provides parasympathetic innervation to the heart and viscera
CN X (10) - Vagus Nerve is tested by
a gag reflex along with CN IX (9)
CN XI (11)
spinal accessory nerve
CN XI (11) spinal accessory nerve
•Innervates cranial cervical (neck) muscles
CN XII (12)
hypoglossal nerve
CN XII (12) hypoglossal nerve
• Motor to the tongue (causes tongue movement)
GDV
Gastric Dilatation Volvulus (Bloat)
GDV is a condition most prevalent in
dogs
GDV mortality rate
15-30%
Is GDV an emergency?
yes patients are typically in critical condition with shock at presentation, requiring aggressive resuscitation and immediate supportive care and monitoring
definitive GDV treatment includes
surgical decompression and derotation of the stomach followed by gastropexy to prevent recurrence.
GDV is most common in
large breed, deep chested dogs. Great dane is most common breed.
When antidiuretic hormone (ADH)is not present
the tubule is not very permeable to water so the urine is dilute
GDV is when the
-stomach rotates counterclockwise when viewing from cranial to caudal in dorsal recumbency
-Also can be stated that stomach rotates clockwise when viewed caudal to cranial
GDV can result in
-venous compression, congestion, and local compromise of perfusion to the stomach, resulting in necrosis
-tearing of short gastric vessels connecting the stomach and spleen
GDV leads to hypovolemic shock because
Air accumulates in stomach, eventually impeding venous return to the heart via the vena cava and resulting in hypovolemic shock
GDV can lead to
-global tissue ischemia and systemic inflammatory response
○ Inflammatory mediators and myocardial ischemia can lead to arrhythmias
GDV happens more in
-large to giant breeds
-deep chested dogs
-Great Dane, German Shepherd,
Rottweiler, Irish Wolfhound, etc
great danes have what percent likelihood of developing GDV
37%
Other predisposing factors for GDV
○ Related to a dog that had a GDV
○ Anxious dogs
○ Very fast eaters
Clinical signs of GDV
● Restless/nervous pacing
● Painful ● Non-productive retching/vomiting
● Abdominal distension
● Increased respiratory rate
● Signs consistent with shock/cardiovascular collapse
○ Tachycardia, weak pulses, pale mucous membranes, prolonged CRT
○ Depressed to comatose mentation
We diagnose GDV by
-ECG- arrythmias common, VPC most likely
-blood gas- Metabolic acidosis (lactic acidosis) +/- respiratory compensation:, May have hypercapnia from gastric distention and impaired ventilation
-radiographs
treatment of GDV includes first stabilizing the patient:
● Place two large-bore cephalic catheters (avoid saphenous since caudal venous return is poor)
● Shock dose crystalloid fluid therapy (80-90 ml/kg in fractions until resuscitation achieved) ○ Patient's large size often requires use of pressure bags for rapid administration of fluids
● Monitor blood pressure and ECG ● Lactate levels may provide some insight as to prognosis
Treatment of GDV includes decompressing the stomach:
1. Orogastric tube
a. Pros: more effective emptying
b. Cons: requires heavy sedation, tube might not pass, possible esophageal trauma/rupture
2. Trocarization
a. Pros: more rapid intervention, does not require sedation
b. Cons: limited decompression, risk of lacerating gastric wall, puncturing spleen
c. Trocarize at point of maximum tympany, can't be sure if spleen is on the left or right
Treatment of GDV inlcludes: Surgey:
● Goal is to fully decompress and reposition stomach, evaluate viability of stomach and resect any necrotic tissue. Also assess spleen, determine if splenectomy is indicated (rarely necessary)
. ● Perform gastropexy to prevent recurrence. ○ Incisional, circumcostal, belt-loop, incorporating, tube.
survival rate of GDV
Reported survival 75-90% with surgery and post-operative care
Negative prognosis indicators of GDV
○ Lactate > 6 mmol/L
○ Need for gastric resection/splenectomy
○ Long onset of signs to time of presentation (5 or 6 hours)
○ Recumbency at presentation
If a patient has GDV and a gastropexy is performed, the recurrence of GDV is
less than 4%
If a patient has GDV and a gastropexy is NOT performed, the recurrence of GDV is
recurrence is 50%