EN 9/10: PHARMACOLOGICAL MANAGEMENT OF DIABETES
1/33
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
34 Terms
Diabetes facts
~830 Million people worldwide have diabetes
~40 Million in the United States
~100,000 deaths in US
1/3rd of diabetics are unaware of their disease
90% have Type 2 diabetes: Symptoms = no at the beginning
Leading cause of blindness in adults → retinopathy (lots of glucose at back of eye)
Twice as likely to develop heart disease
Diabetes = Obesity / Obesity = Diabetes ?
Chronic Complications of Diabetes mellitus
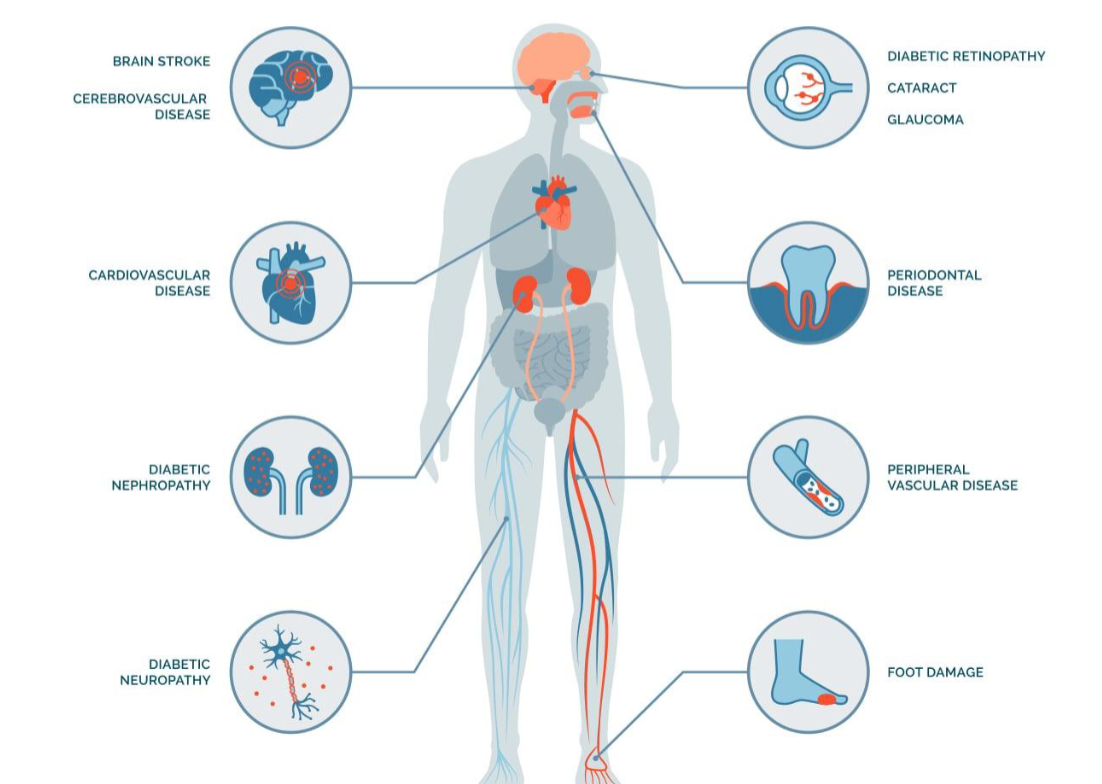
foot ulcers
can lead to gangrene + eventually amputation
diabetic retinopathy
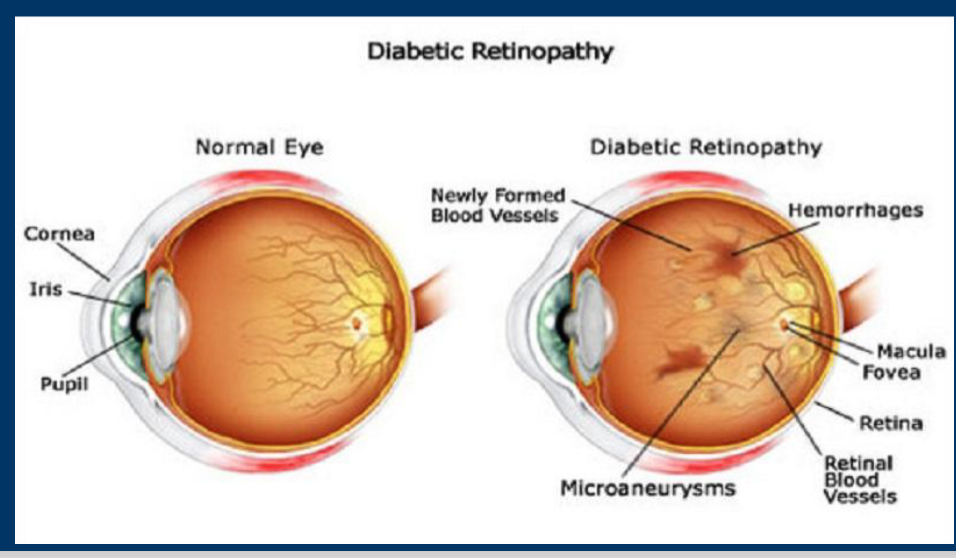
hemmorhages and microaneruysms
Opportunistic Infections of diabetes

Lipodystrophy of Diabetes
when you inject insulin to the same place over and over
can add more fat to one place and take away the fat from another

Oral Manifestations of Diabetes
periodontal disease - poorly controlled diabetes, suppuration = pus
Acute Pseudomembranous Candidiasis, not same appearance as albicans
Oral candidiasis is associated with an increase in:
• Increased salivary glucose
• Xerostomia
• Impaired immune response
• Opportunistic infections
• Poor wound healinglichen planus - tx by steroids
parotid enlargement (extraoral) - affects facial nerve can → face pain
severe xerostomia
Goals of Management
Lifestyle changes (workout, eat better, etc)
Deal aggressively with comorbidities (retinopathy, neuropathy)
Cardiovascular health and risk factors
Maintain HbA1c levels consistently
Metformin…To prescribe or not to prescribe?
Shorten the duration of uncontrolled Diabetes
Lengthen life expectancy
Manage the Disease or the Syndrome?
METABOLIC SYNDROME characterized by high levels of blood
glucose resulting from-
1.Defect in insulin production/ secretion
2.Defect in insulin action/ Glucose uptake
3.Both
Chronic hyperglycemia with disturbances of carbohydrate, fat and protein metabolism
Concerns: Long–term damage, system dysfunction and failure of
various organs due to gluconeogenesis can lead to Incidental / Emergent hypoglycemia in the dental environment
gluconeogenesis
creation of new glucose from fats and amino acids
Types of Diabetes
Type 1 Diabetes mellitus - immune condition
Type 2 Diabetes mellitus - 95% pt
Gestational Diabetes - no history of diabetes + no familial link, primigravida (preggo for the 1st time)
Prediabetes - elevated glucose lvls
Other types:
LADA (Latent Autoimmune Diabetes in Adults- Type 1.5)
MODY (Maturity onset diabetes of youth- Rare)
Monogenic Diabetes Mellitus (linked to chromosomal abnormalities)
What is Diabetes insipidus?
a pt lacks ADH from posterior pituitary so they constantly pee
treated w diuretics due to paradoxical effect
Gestational diabetes
A form of glucose intolerance during pregnancy.
More frequent among African Americans, Hispanic/Latino Americans, Southeast Asians
Obese women with a family history of diabetes
Normalize maternal blood glucose levels to avoid complications in the infant.
After pregnancy, 5-10% have type 2 diabetes.
Women with GD have a 20-50% chance of developing diabetes in the next 5-10 years.
LGA Babies(Large for Gestational Age)
extra glucose goes to baby and they gain weight
cannot be born vaginally due to cephalous being too big for mothers pelvis
Other types of DM
Other specific types of diabetes result from specific genetic conditions
Maturity-onset diabetes of youth
Surgery
Drugs
Malnutrition
Infections
Such types of diabetes may account for 1% to 5% of all diagnosed cases of diabetes.
Drug induced Diabetes Mellitus
Atypical Antipsychotics
Beta-blockers (-olol)
Calcium Channel Blockers (-dipin)
Corticosteroids (-sone)
Fluoroquinolones (-floxacin)
Niacin
Phenothiazines
Protease Inhibitors (-navir)
Thiazide Diuretics
Furosemide
Lithium/ Alcohol/ Opioids/ Rodenticides
Pharmacological Management of Diabetes Mellitus: ABCs

a. diet
Appropriate nutrition
Dietary treatment should aim at:
Ensuring weight control
Providing nutritional requirements
Allowing good glycemic control
Correct blood lipid abnormalities
Monitoring daily intake
Decreasing salt intake
Classification of Hypoglycemic agents: Biguanides
Reduce hepatic glucose production and increase insulin sensitivity.
do not require functioning pancreas
e.g., Metformin
Classification of Hypoglycemic agents: Sulfonylureas
Stimulate insulin secretion from pancreatic beta cells.
require functioning pancreas
e.g., Glipizide, Glimepiride
Classification of Hypoglycemic agents: Meglitinides
Stimulate rapid, short-acting insulin release
require functioning pancreas
e.g., Repaglinide, Nateglinide
Classification of Hypoglycemic agents: Thiazolidinediones (TZDs)
Enhance insulin sensitivity in muscle and adipose tissue.
do not require functioning pancreas
e.g., Pioglitazone, Rosiglitazone
Classification of Hypoglycemic agents: DPP-4 Inhibitors
Increase insulin release and reduce glucagon levels by inhibiting the DPP-4 enzyme.
Sitagliptin, Linagliptin
Classification of Hypoglycemic agents: SGLT2 Inhibitors
Reduce glucose reabsorption in the kidneys, leading to increased glucose excretion in urine.
Dapagliflozin, Empagliflozin
Classification of Hypoglycemic agents: GLP-1 Receptor Agonists
Mimic incretin hormones to boost insulin secretion and reduce glucagon
release
Semaglutide, Liraglutide
Classification of Hypoglycemic agents:
Slow carbohydrate digestion in the gut.
Acarbose, Miglitol
ways to give Insulin
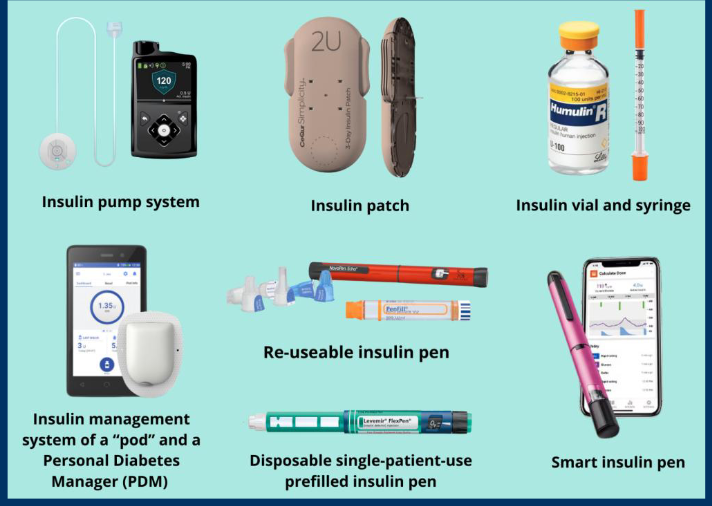
types of insulin
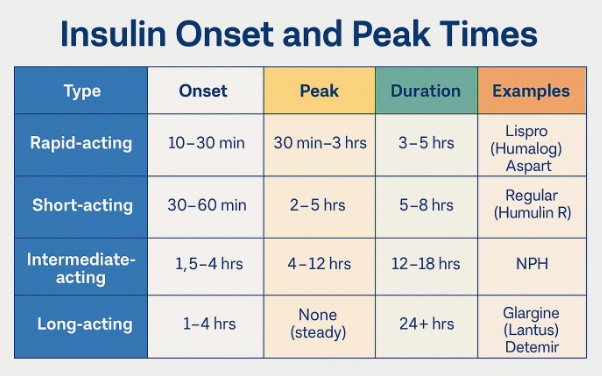
know brands too
Combination oral agents is indicated in
Newly diagnosed symptomatic patients with HbA1c >10
Patients who are not reaching targets after 3 months on monotherapy
Consider intermediate-acting / long-acting insulin
Insulin dose can be increased until target FPG is achieved. (sliding scale method to determine insulin requirements in units)
C. Insulin Therapy: When to use?
Short-term use: (hospitalized or something)
Acute illness, surgery, stress and emergencies
Pregnancy
Breast-feeding
Insulin used as initial therapy in type 2 diabetes
In emergency hyperglycemia
Severe metabolic decompensation (diabetic ketoacidosis, hyperosmolar non-ketotic coma, lactic acidosis, severe hypertriglyceridemia)
drug of choice for type 1 diabetes
insulin
ADA:SUMMARY OF GENERAL MANAGEMENT
Assess Glycemic control
Refer patients with signs of undiagnosed diabetes to a physician for diagnosis and treatment
Obtain a consult with the patient's physician if systemic complications are present
Assess the use of medications for oral complications
Use a glucometer to avert dental chair emergencies
Aggressively treat acute oral infections
Schedule patients for frequent recall visits to monitor and treat oral complications
Maintain optimal oral hygiene and diet
Support and follow up patients in smoking-cessation programs
metformin/ glucophage max daily dose
the maximum recommended dose is typically 2000 mg per day
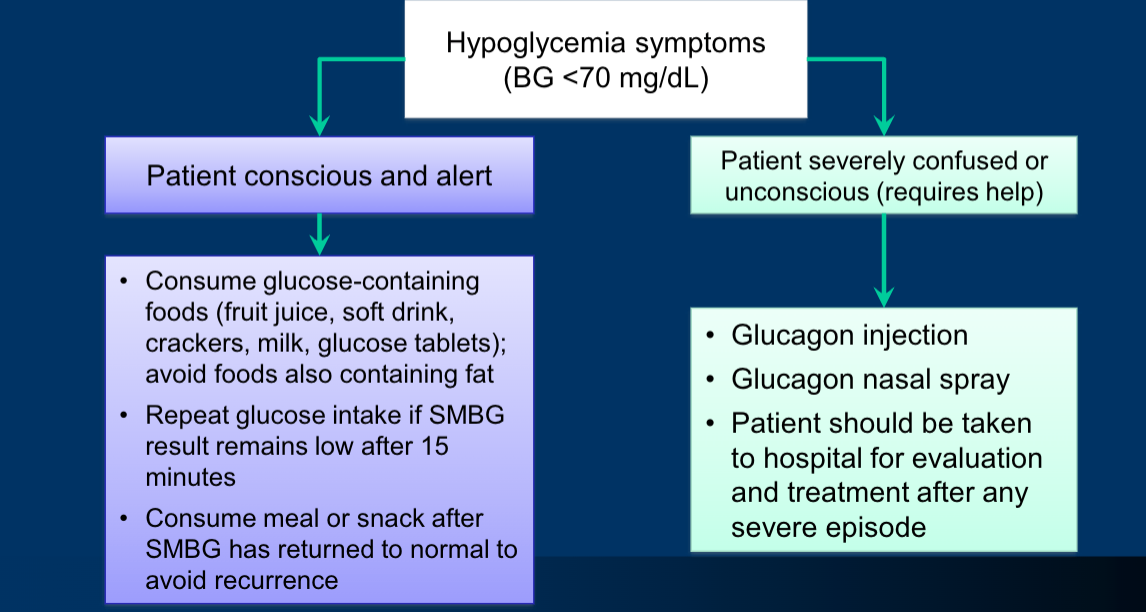
Treatment of Hypoglycemia