Electrophys Final Questions
1/61
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
62 Terms
Why do you need electrodes for electrophysiological measurement?
To capture electrical activity
Where do you place inverting, non-inverting, ground electrodes (1-channel recording)? (Mark it in the following diagram?
Inverting= negative; non inverting= positive; ground=neutral

Based on 10-20 electrode nomenclature, what are A1, A2, M1, M2, Fz, Fpz, Cz?
A1-LE lobe
A2-RE lobe
M1-L Mastoid
M2- R Mastoid
Fz- Upper Forehead
Fpz- Mid-forehead
Cz: Vertex (top of head)
What are the recommended impedances differences between electrodes? Why is it essential to have such a low impedance differences between electrodes?
Absolute electrode impedance should be below 5 kΩ
Inter-electrode impedance differences must be ≤ 2 kΩ
Low matched impedance is essential so differential amplification can cancel shared noise (common mode rejection). If impedances differ too much, noise leaks in and the ABR waveform degrades
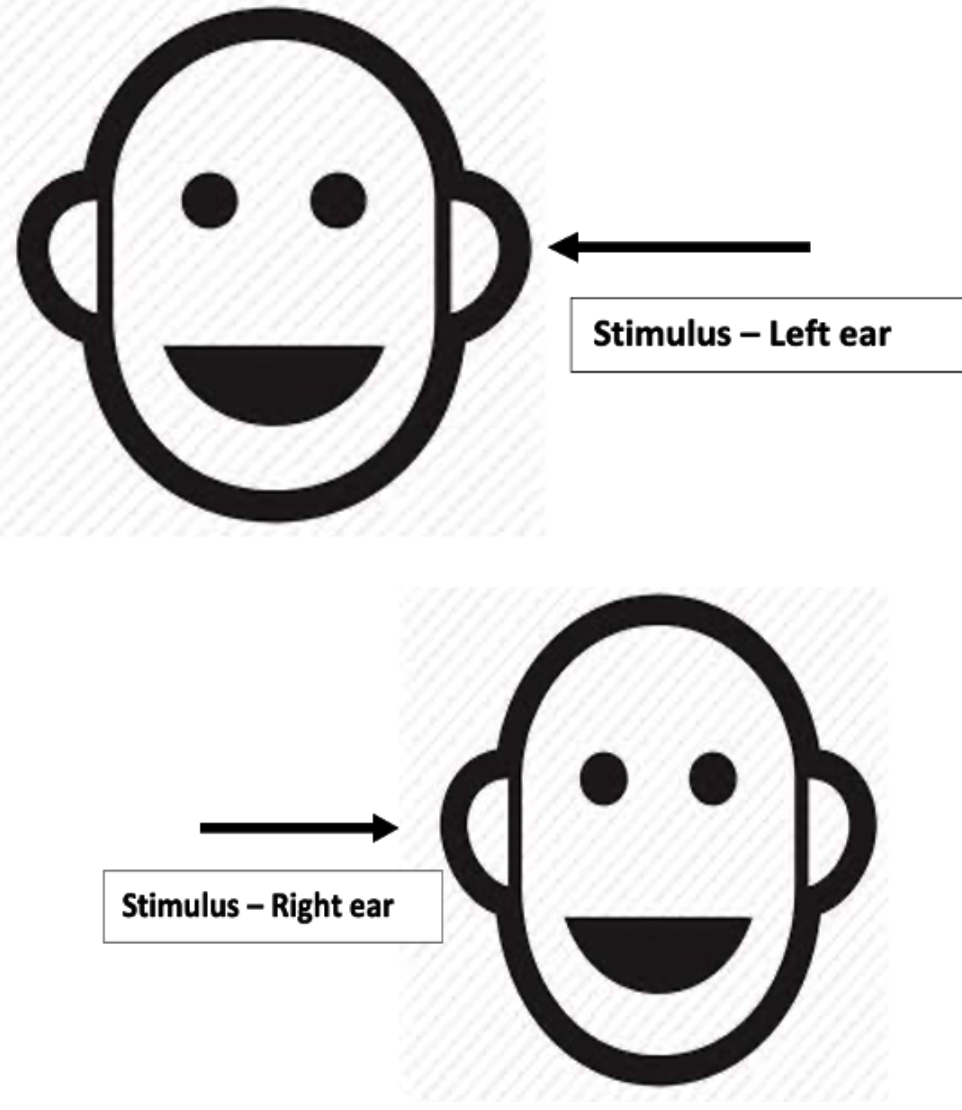
Where do you place inverting, non-inverting, ground electrodes (1-Channel recording) when stimulating the right ear?
Non-inverting (positive): high forehead (Fz or FCz)
Inverting (negative): right mastoid or earlobe (M2 or A2)
Ground: anywhere neural, usually left mastoid/earlobe (M1/A1) or cheek
What are ipsi/contra channels? What are the advantages of recording 2 channels (ipsi & contra) than 1-channel (ipsi alone)?
ipsi channel: forhead (+) to same ear (-).
Best for Wave 1 & early waves (closest to generator).
Contralateral channel: Forehead (+) to opposite ear (-)
Best for wave IV-V separation (closer to their generators)
Advantages of 2 channels: (Gives strong early waves + clean late waves at the same time→ easier interpretation)
better wave I- II on ipsi
Clearer wave IV- V on contra
More accurate wave V identification
What are the differences in ABR response morphology between vertical and horizontal montage recorded ABR?
Vertical montage (forehead→mastoid):
Stronger wave V
Better later waves
Used for ABR (focus on later peaks)
Horizontal montage
Larger wave 1 & early peaks
Later waves smaller or may disappear
Used for EcochG (focus on early cochlea/nerve responses)
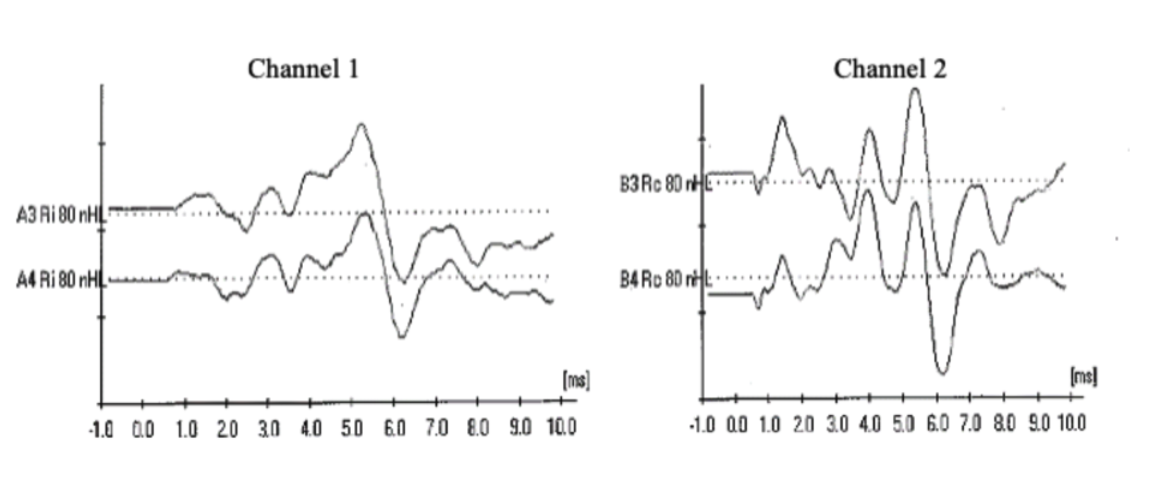
You are recording from a two-channel set-up (ipsi in the first channel, contra in the second). You are stimulating the right ear at 80dB nHL. Why would you be concerned if you recorded the following waves?
Waveforms are inverted (caused from electrode montage error-pos and neg switched)
Channel 1 is IPSI and Channel 2 is Contra. Contra cant have a wave I bigger than ipsi bc ipsi means you are stimming same ear and wave will arrive sooner than stimulating contra.
Why does EP equipment have to perform numerous signal processing (differential amplification, filtering, artifact rejection, averaging) when recording ABR?
1. bc ABR signal is extremely small
2.Differential amplification reduces common mode noise (subtraction between electrodes) : anything common to both electrodes (like electrical interference or muscle noise) is subtracted out
3.Filtering removes unwanted frequencies: HF filters remove slow EEG waves, LF filters remove hf muscle noise, notch filters remove electrical line noise (60 Hz)
4.Artifact rejection removes big bursts of noise (movement or electrical spikes can create artifacts
5.Averaging extracts the ABR from the noise (averaging thousands of sweeps)
What is differential amplification (common-mode rejection)? What is the assumption of differential amplification?
CMR: to eliminate the common noise, subtract pos-neg
If the difference is too big, noise may appear different (leading to high impedance)
Assumption of differential amplification: similar impedances at all sites (less than 5 kOhms total; less than 2 kOhms b/t electrodes)
Why is it a bad idea to place the non-inverting and inverting electrodes right next to each other?
Placing the non-inverting and inverting electrodes next to each other causes the ABR signal to cancel out-because the two electrodes pick up nearly identical activity - destroying the differential voltage that the amplifier needs to extract the ABR
How are the filter settings different between ABR and LLR?
ABR: 30-3k Hz
LLR: 0-30 Hz
What are your low-pass and high-pass filter settings for testing infants/children using the click and tone burst?
TB: HPF: 30-100Hz, LPF: 1500-3000Hz (30often preferred for infants)
Click: HPF: 100-150Hz, LPF: 1500-3000Hz (best morphology waves I-V)
Why do you need to average thousands of trials to measure discernible ABRs?
bc ABR is tiny compared to the background noise, requiring averaging to enhance the signal-to-noise ratio.
Explain the determinants of the number of averages for measuring electrophysiological responses
depends on:
1. Amplitude of EPs (intensity effects)/Fmp helps determine sweeps required
SNR >3; A+B= signal; A-B= noise
Background noise
Discuss maturational changes of ABR? what are the physiological bases for these changes?
Maturational changes in ABR include increased wave amplitudes and decreased latencies as the auditory system matures. Physiologically, these changes are attributed to myelination of auditory pathways and synaptic development in the central auditory system.
Infants have longer latencies
Interpeak latencies are longer
wave i matures first, (wave V is slowest to mature)
Latency gradually shortens until 18-24 months then has similar adult values
What are the physiological bases for these changes?
Incomplete myelination in newborns
Immature synapses take longer to process
Smaller axon diameter in infants-slower transmission speed
Delayed brainstem pathway maturation
ABR changes due to changes in body temperature. What are the changes to the ABR response metrics with hypothermia, hyperthermia ?
hypothermia (low temp)
Neural conduction slows down
Synaptic transmission is less efficient
Ion channel activity decreases
hyperthermia (high temp)
Neurons fire faster
Synapses transit quicker
Ion channel kinetics speed up
Does patient state affect ABR responses? (being awake vs asleep)
No meaningful impact but muscle movement or tension while being awake does create more noise and can make it harder to read ABR waves (the noise level is impacted)
What are Early Hearing Detection and Intervention (EHDI) 1-3-6 guidelines?
<1 mo screening
<3 mo diagnose
<6 mo intervention
When is the better time to perform the newborn hearing screening?
In the first 48 hours after birth, as close to discharge time as possible
Discuss JCIH’s recommended hearing screening protocol.
For well babies
Two-stage screening and re-screening with either OAE or Automated ABR before discharge from hospital.
If the baby does not pass initial OAE/AABR screening, then rescreening should be done using OAE/AABR (only a single repeat screening)
If not passed in either ear– referred for diagnostic evaluation
For NICU babies
AABR only
What is the recommended screening test for infants visiting NICU? Why?
ABR bc fewer false positives
ANSD more prevalent w/ NICU population
Does passing a hearing screening performed either by OAE or by ABR indicate a hearing threshold within normal limits? Comment on this statement?
OAE is not freq specific, is not mild loss specific and cannot be used to diagnose ANSD while ABR can provide more detailed information about hearing thresholds and may help identify specific types of hearing loss.
Comment on the frequency and place specificity in context to the use of ABR to obtain audiogram-like information.
ABR follows the cochlea’s tonotopic map, so high frequencies appear earlier and low frequencies later. Tone-bursts improve frequency targeting, but there’s still spread of excitation, so ABR isn’t fully place-specific. Because of this, ABR thresholds reflect a general cochlear region—not a single frequency—and give estimated audiogram-like thresholds.
Regarding Pediatric ABR:
List the primary purpose of ABR in this population.
To estimate frequency-specific hearing sensitivity when behavioral testing can’t be done
Closest to audiogram like info; to best fit HAs
Regarding Pediatric ABR:
List the advantages of performing ABR in this population for this purpose.
Px can be asleep
Can be done on children who are not developmentally ready for behavioral audiometry
Can provide ear-specific and frequency-specific estimates
Allows for early diagnosis
Regarding Pediatric ABR:
List limitations/compromises in performing ABR in this population.
Low frequency and click may not be very similar
testing in time sensitive and requires infants to be asleep and quiet
Stim must be short to keep neural synchrony which reduces true freq specificity
In context to ABR test protocol to obtain audiogram-like information in an infant. Explain with adequate justification for each choice-
a)the choice of stimuli
b)the electrode config
c) number of averages
e) filter settings
a) the choice of stimuli click (rule of ANSD) and TB/NBChirp: 500, HF, fill in
b) the electrode configuration 2-channel
c) stimulus repetition rate 39.9 rep/sec
d) number of averages depends
e) filter settings 30-1500 Hz, 30-3k for CM, gain: 100k-150k
Why do we need to have different correction factors to estimate hearing thresholds across TB frequencies?
Because each frequency behaves differently in the cochlea and in the ABR recording, a single correction factor would be inaccurate, so each TB frequency needs its own.
LFs have greater distance
McCreery et al., (2015) provided Frequency dependent ABR threshold correction factors as a function of the degree of hearing loss. Why?
ABR thresholds are closer to behavioral for hearing impaired (>60dBHL no correction factor 1k-4k)
Example:
TB (20 ms) Normal thresh: 10 dB; HI thresh: 70 dB
Audio (200ms) Normal thresh: 0 dB; HI thresh: 70 dB
ABR thresholds tend to overestimate behavioral thresholds (elevated threshold when hearing is normal) in normal-hearing individuals and underestimate (better hearing than the behavioral threshold) behavioral thresholds in individuals with hearing loss. What is the proposed psychoacoustic reason behind this? Explain
It is due to differences in temporal integration between normal-hearing ears and ears with cochlear hearing loss.
Normal hearing: Strong temporal integration → behavioral thresholds better than ABR → ABR overestimates threshold.
Hearing loss: Weakened temporal integration + increased spread of excitation → ABR looks better than behavioral → ABR underestimates threshold.
While recording ABR on a 3-week infant, you looked for a wave V at ~5.5ms (mean wave V latency among NH adults). Is it a problem? Why?
3- week infant won’t have adult like wave V latencies and will be later than 5.5 ms (1-2ms later) because of immature auditory systems, synaptic delay and reduced neural synchrony
Latency should be longer (6.5ms)
using adult norms will lead to misinterpretation of normal infant responses as abnormal
What is the advantage of BC ABR over immittance evaluation in pediatric diagnostics test battery?
May not be sufficient to determine degree or rule out SNHL with flat tymp
ABR directly tells you whether the cochlea and neural pathway can respond, even when there is conductive component to the HL
Why do infants have greater IA for BC compared to adults?
Because skull is not fully fused so vibrations do not transmit as effectively
Discuss the differences in BC oscillator placement between infants Vs adults.
May be placed higher on the temporal skull when no mastoid space
Use velcroband
List some of the limitations of BC-ABR.
BC-ABR has Reduced output/ dynamic range (50 @500, 50-60 @2k-4k–vibrotactile), more artifact, poorer wave morphology, requires very precise placement, takes longer to record, has limited frequency range, and may produce vibrotactile responses.
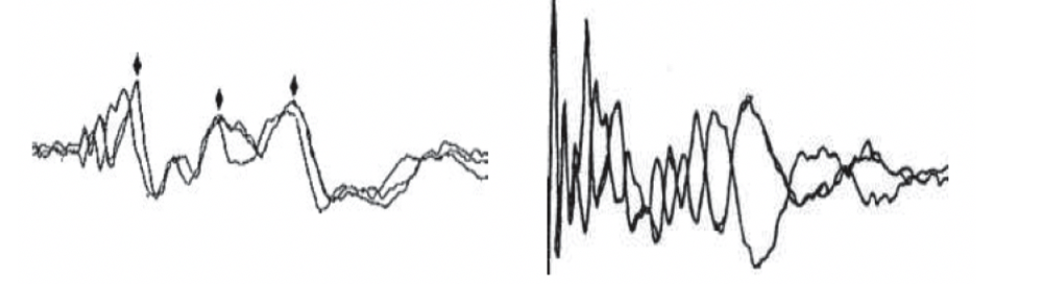
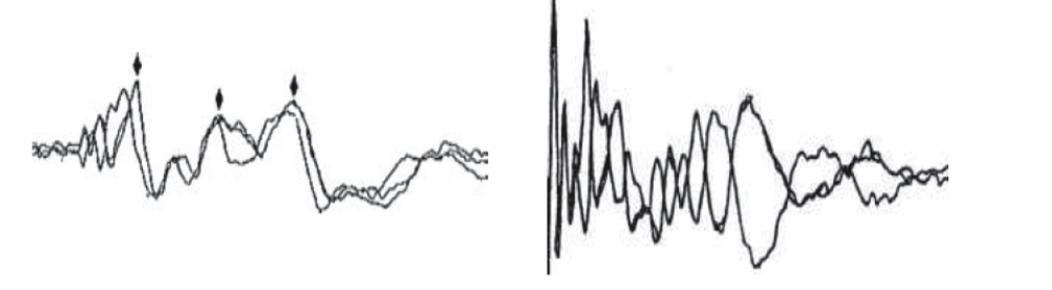
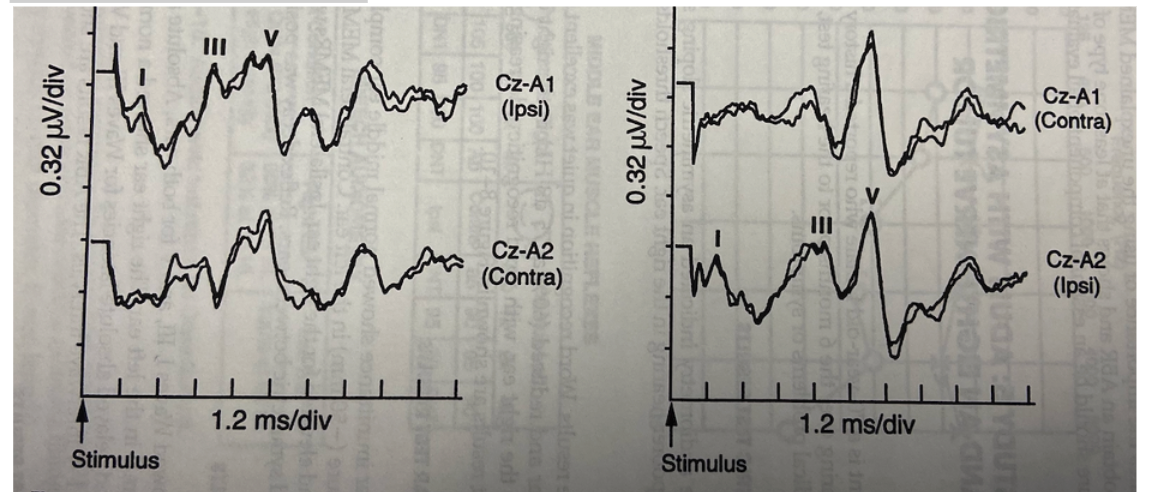
Explain the following two waveforms (left panel and right panel separately) with respect to neural synchrony and cochlear microphonics. Please note that the two overlapped waveforms are recorded at 80 dB nHL for click stimulus with opposite polarity. The entire time window of the waveforms is 10ms.
First one is WNL- EP consistent (CM invert, neural responses do not)
Second one is ANSD- graphs are reflections after using opposite polarity, CMs only
Why is it important to carefully examine the initial 3-4ms recording when you observe no measurable wave V (particularly when you suspect ANSD)?
When Wave V is absent, you need to look closely at the early portion of the recording to check whether Wave I (or cochlear microphonic/early neural activity) is still present (CM= cochlea’s electrical “echo” of the sound, generated by outer hair cells. It is used to help diagnose ANSD when cochlear function is normal but neural responses are absent)
If Wave V is absent, but an early response exists, the problem is neural synchrony, not cochlear function
What is it? What additional testing do you do to confirm this?
ANSD is:
Normal cochlear (OHC) function
Absent or severely abnormal ABR beyond the earliest components
Neural desynchrony at or beyond the IHC–synapse–auditory nerve level
Testing?
OAE testing
AR
Repeating ABR with polarity changes
Evaluate wave I using high-intensity clicks
What is your ABR protocol to rule out ANSD?
High-level click ABR (80–90 dB).
Record rarefaction and condensation separately.
Look for CM in the first 2–3 ms (polarity reversal).
Check for absent or abnormal neural waves (I–V).
Blocked-tube test to verify CM is real.
Run OAEs (should be present).
Check acoustic reflexes (usually absent).
What are the classic audiological test battery findings among individuals with ANSD?
OAEs: Present
CM: Present (polarity-reversing)
ABR: Absent or severely abnormal Wave V
Acoustic Reflexes: Absent
Tympanometry: Normal
Speech perception: Disproportionately poor
Behavioral thresholds: Variable and unpredictable
Using latency-intensity function (LIF) how would you distinguish between conductive, cochlear, and retrocochlear lesions?
Conductive HL (ABR LIF Pattern)
Sound is delayed getting to the cochlea → equal latency rightward shift at all levels.
Normal slope, normal interpeak latencies.
Cochlear HL
OHC damage reduces synchrony at soft levels → steeper LIF slope.
Wave V prolonged at low levels, but near-normal at high levels (recruitment pattern).
Retrocochlear HL
Latencies worse than expected for the audiogram.
Distorted/irregular LIF, prolonged interpeaks (especially I-III), poor waveform morphology.
What is the difference in the LIF (latency intensity function) for mild (35 dB) conductive hearing loss as compared to a normal sloping to moderate hearing loss of cochlear hearing origin?
Conductive = parallel rightward shift, normal slope,
Cochlear = steep slope, abnormal low intensity latencies, near-normal high-intensity latencies—a recruiting pattern.
Conductive (~35 dB): Wave V at 80 dB is still late
Cochlear (sloping moderate): Wave V at 80 dB becomes normal or almost normal
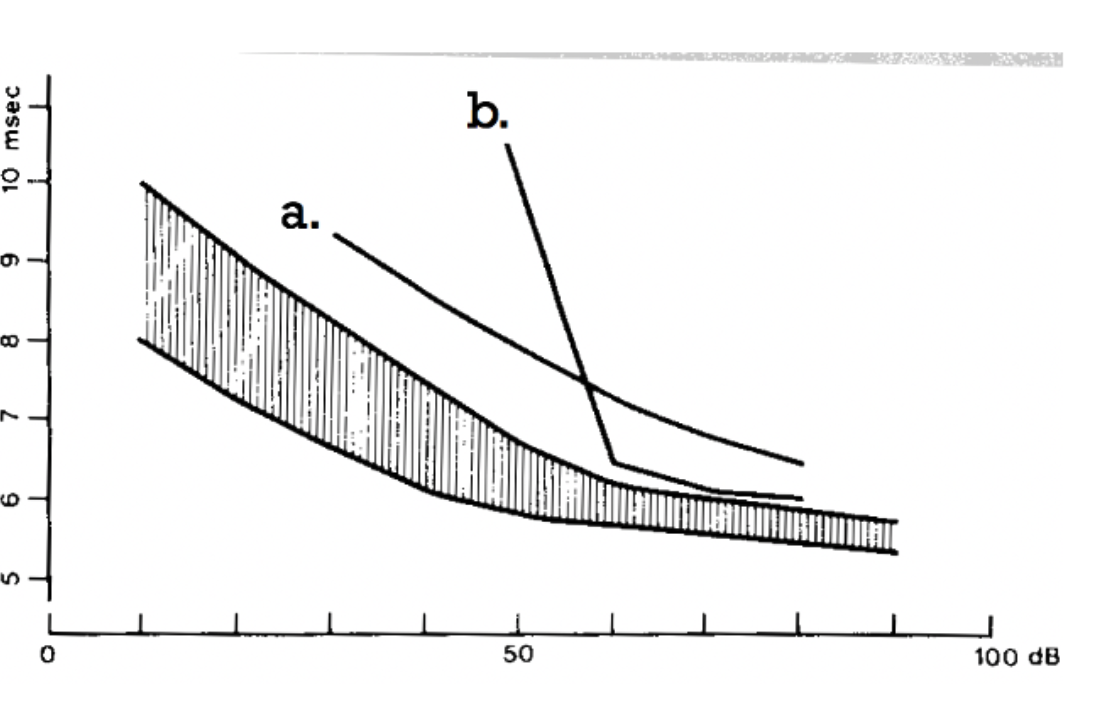
What is the most likely type of hearing loss for the following two (a & b) latency-intensity functions? What made you arrive at that conclusion?
A = conductive HL - because it is parallel with normal slope compared to the normal range
B = sensorineural HL- because steep slope, shifts most at high intensity
In a pediatric case, what does conductive hearing loss do to the Wave V absolute latency at high intensity?
A conductive loss causes a uniform delay, This is why the latency-intensity function for conductive loss appears parallel and shifted to the right even at high intensities
WV latency is increased,
the degree of delay matches the size of the air-bone gap, and the latency–intensity slope remains normal.
Discuss the relationship between ABR wave V latency Change and the Degree of cochlear hearing loss.
Relationships present but not perfectly predictable.
In general, WV latency increases as the degree of cochlear HL increases, (especially > 50 dB). The exact amount of change depends on degree and configuration.
This happens because damage to the outer hair cells reduces cochlear amplification, causing poorer neural synchrony at lower effective sensation levels.
At high intensities (90 dB nHL), WV latency often increases by about 0.1 ms for every 10 dB of threshold elevation in the high-frequency region. However, sloping high-frequency losses produce greater Wave V latency shifts than flat cochlear losses (reduced contribution from the basal regions of the cochlea).
Discuss the findings from Lewis et al (2015) study measuring the ABR changes at equal SL and equal SPL between normal hearing and mild to moderate cochlear hearing loss.
At equal SPL: Wave V latency looks normal in mild–moderate cochlear loss because high levels override OHC damage.
At equal SL: Cochlear-loss listeners show shorter latencies due to recruitment and faster neural firing at higher effective intensities.
Give examples of parameter settings (or other aspects in ABR testing) designed to maximize the recording of Wave I in adult testing.
Use vertical ipsi montage (high forehead to ipsi mastoid/earlobe)
Record 2 channels (ipsi and contra)
Use high intensity stimulus
Use rarefaction polarity
11-21/s moderate repetition rate
Good low-impedance electrodes
100-3000Hz filters
Inserts instead of speakers or headphones
What does a pathology in the mid-to-upper brainstem do to the ipsilateral Wave I ?
No effect (W1 happens before pathology)
Regarding Adult ABR:
List the primary purpose of ABR in this population.
Hearing screening
Estimation of hearing thresholds
Neuro-otologic applications- determine site of lesion & intraoperative monitoring
Regarding Adult ABR:
List the advantages of performing ABR in this population for this purpose.
Noninvasive way to assess auditory nerve and brainstem timing (ABR lets you look at interpeak latencies and tells you where the abnormal neural conduction is)
Can detect neural dysfunction even when hearing thresholds are normal
Useful when imaging is not immediately available or contraindicated
Quick test
Regarding Adult ABR:
List limitations/compromises in performing ABR in this population for this purpose.
Not very sensitive to small tumors (<1cm.)
MRI is still the gold standard
ABR changes are subtle
Hearing loss can make interpretation harder
Only assess the auditory pathway up to the midbrain
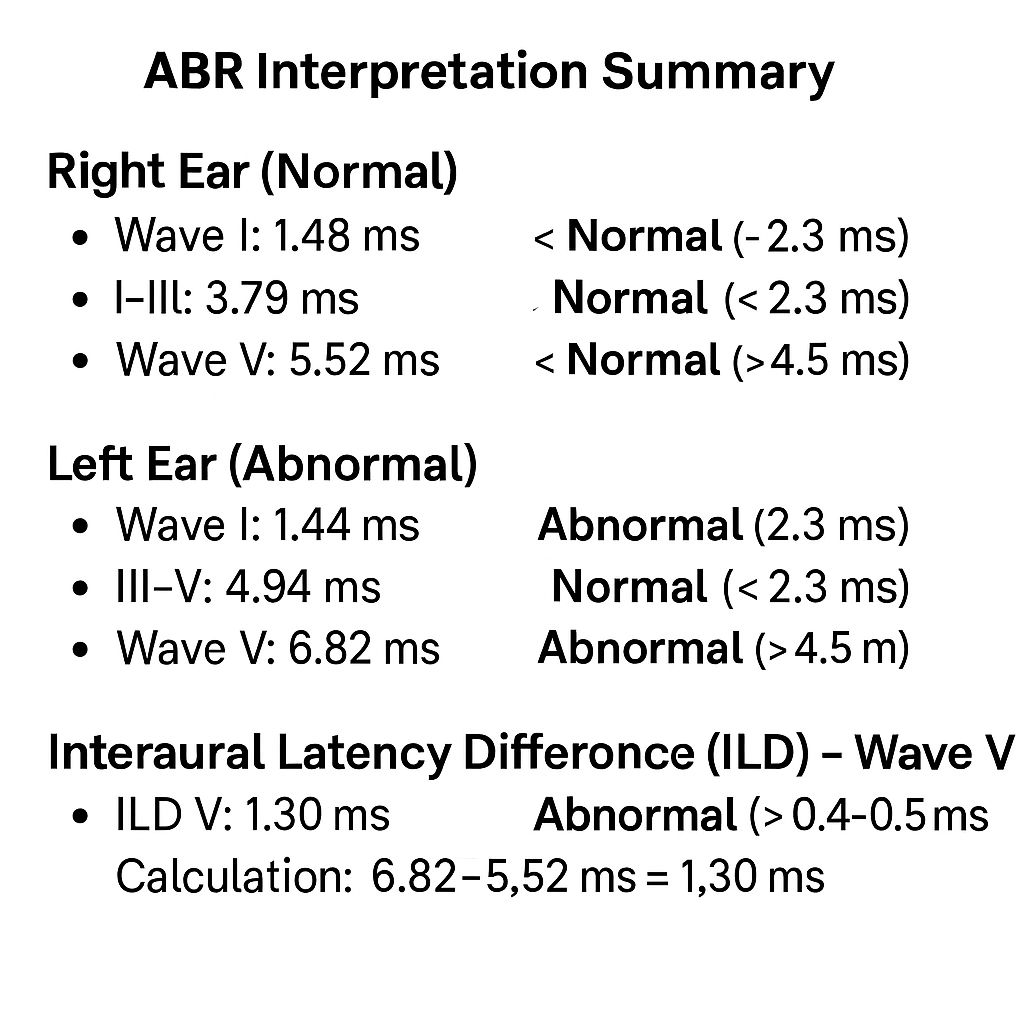
. Tricky question - Assume you are assessing an adult with ABR. You find the following:
Wave V in right ear was 7 msec =
Wave V in left ear was 5.64 msec =
The I-V IPL in right ear was 3.99 msec =
The I-V IPL in the left ear was 4.1 msec =
Wave V in right ear was 7 msec = delay
Wave V in left ear was 5.64 msec = WNL
The I-V IPL in right ear was 3.99 msec = WNL
The I-V IPL in the left ear was 4.1 msec = WNL
Tricky question - Assume you are assessing an adult with ABR. You find the following:
Wave V in right ear was 7 msec =
Wave V in left ear was 5.64 msec =
The I-V IPL in right ear was 3.99 msec =
The I-V IPL in the left ear was 4.1 msec =
What is your interpretation of these results (what is your conclusion regarding the ABR)?
A likely conductive pathology in the right ear there is no evidence of retrocochlear involvement
Prolonged absolute Wave V latency in the right ear
Normal I–V interpeak latencies bilaterally
Large interaural Wave V latency difference
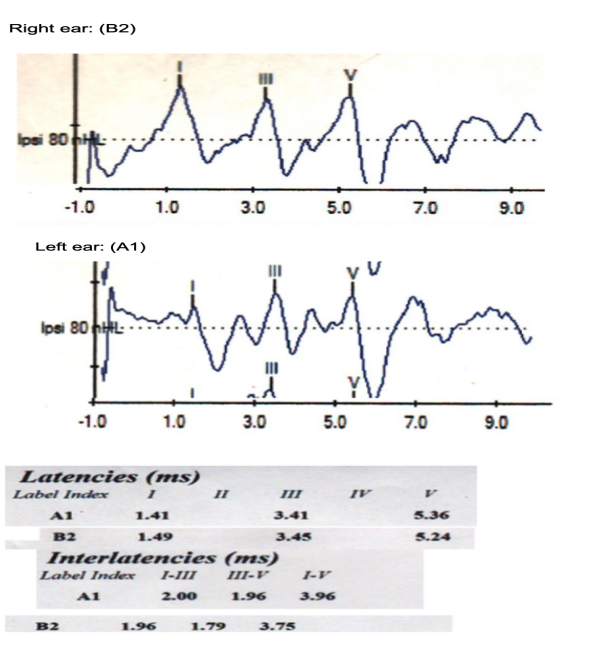
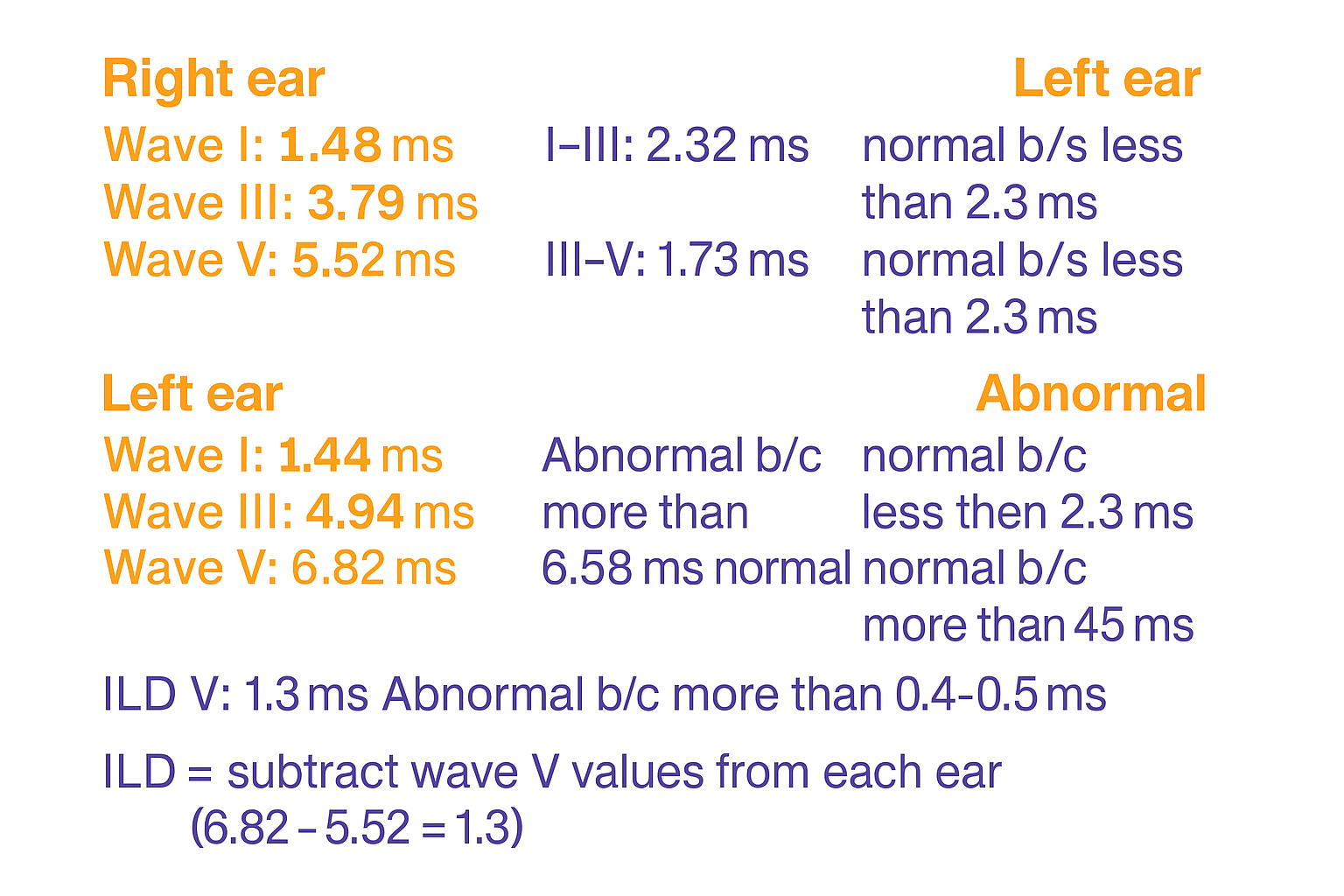
Review the left and right ABR waveform and latency indices obtained from a 31-yr female to assess neurological status.
Provide the ABR interpretation of the data for both ears and what are the reasons behind your interpretation.
FYI:
Normative adult values:
Wave I: ~1.5 ms
Wave III: ~3.5 ms
Wave V: ~5.5 ms
I–III IPL: ~2.3–2.4 ms
III–V IPL: ~2.2–2.3 ms
I–V IPL: ~4.4–4.5 ms
Both A1 (left) and B2 (right) ABRs are normal.
There is normal auditory nerve and brainstem conduction bilaterally, with no evidence of retrocochlear pathology.
The slightly “early” absolute latencies are simply individual variation, what matters in neurodiagnostic ABR is whether interpeak latencies are prolonged or interaural differences exceed norms, and none of that is happening here.
FYI:
Normative adult values:
Wave I: ~1.5 ms
Wave III: ~3.5 ms
Wave V: ~5.5 ms
I–III IPL: ~2.3–2.4 ms
III–V IPL: ~2.2–2.3 ms
I–V IPL: ~4.4–4.5 ms
Review the following information and the ABR waveform to answer the following questions
CASE GJ: GJ is a 42-year-old female with hearing within normal limits in both ears. Word recognition scores is excellent 100% for both ears. Tympanometry WNL. She complains of tinnitus in each ear, worse in the right ear.
Provide interpretation of the following ABR obtained on this patient. What are the reasons behind your interpretation?
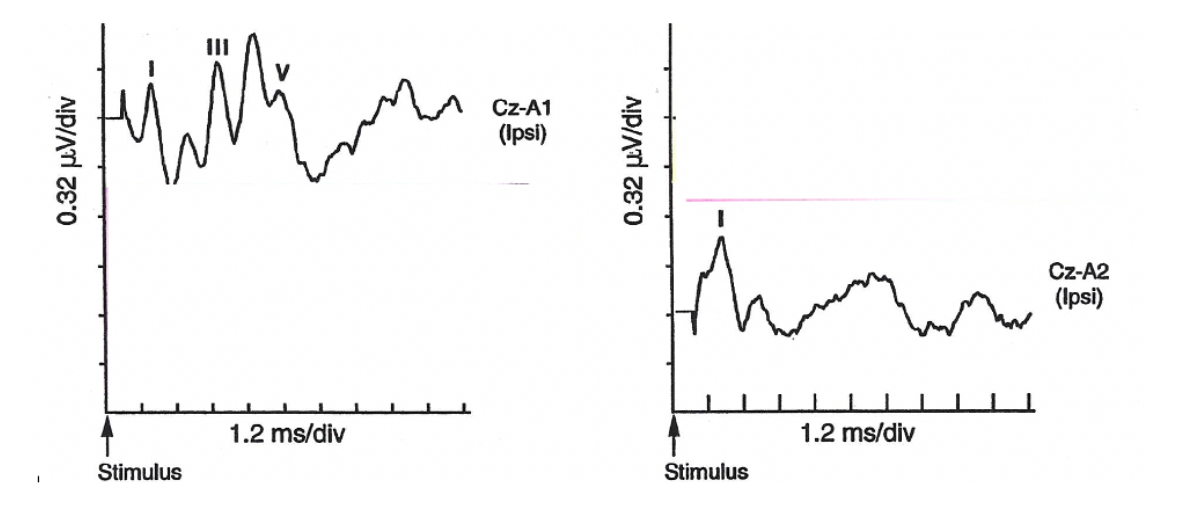
The ABR responses (80 dBnHL) below were obtained from a 56-year-old male with normal hearing in the left ear and gradually worsening mild high-frequency sensory-neural hearing loss in the right ear.
I: Discuss the ABR test findings for each ear.
II: If any of the findings are abnormal, discuss the possible site of the lesion.
i: Discuss the ABR findings for each ear.
LE: WNL
RE: WI present, WV absent
II: If any of the findings are abnormal, discuss the possible site of the lesion.
Site of lesion is beyond the distal auditory nerve since a mild HF SMHL would not explain the absence of wave III and V = retrocochlear issue
Present wave I + absent III & V = strong red flag for retrocochlear involvement
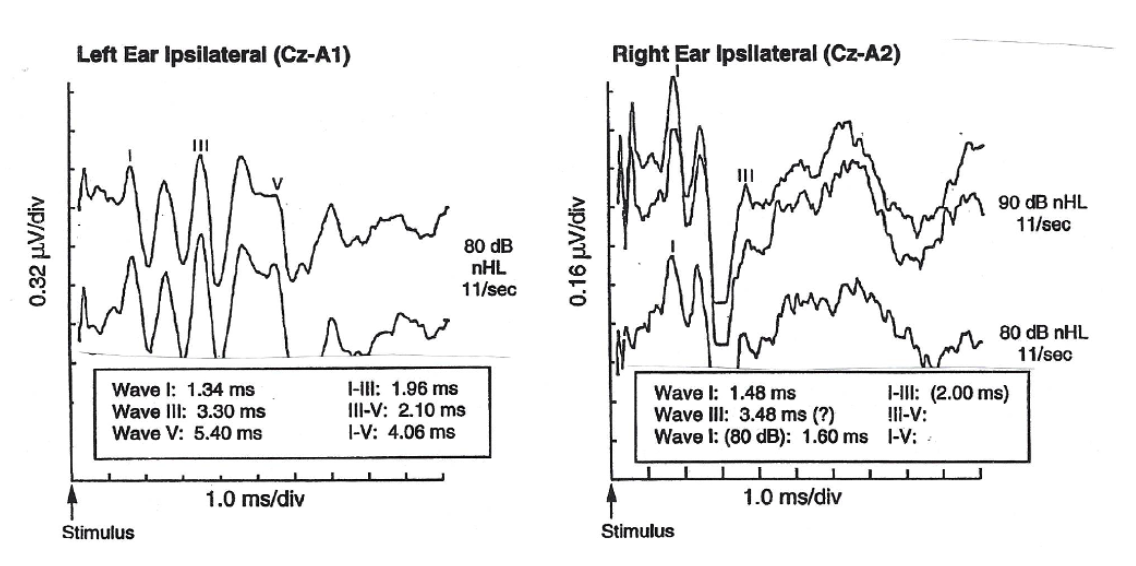
The ABR responses below were obtained from a 42year old female.
I. Is ABR in right ear completely WNL? why?
II. Describe the findings (findings only) for the Left ear?
III. What are the TWO DIFFERENT explanations for the LEFT EAR findings?
I. Is ABR in right ear completely WNL? why?
Yes, all latencies WNL
II. Describe the findings (findings only) for the Left ear?
WV late latency, other waves absent
III. What are the TWO DIFFERENT explanations for the LEFT EAR findings?
-CN8 Tumor
-Conductive HL
The ABR responses (80 dBnHL) below were obtained from a 32-year-old female with a diagnosis of multiple sclerosis.
A. Is ABR in LEFT EAR completely WNL?
B. Is ABR in RIGHT EAR completely WNL?
C. IF either of the above was not WNL, provide one specific finding that supports this.
A. Is ABR in LEFT EAR completely WNL? YES
B. Is ABR in RIGHT EAR completely WNL? NO
C. IF either of the above was not WNL, provide one specific finding that supports this.
WV absent
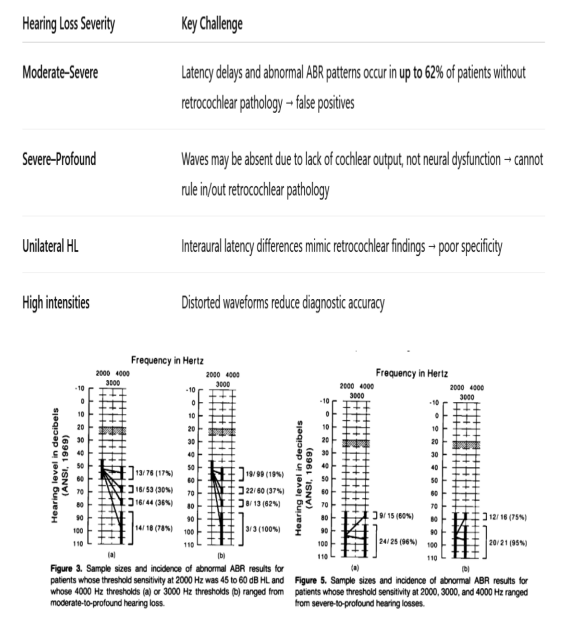
You are referred to two patients for neuro-diagnostics ABR evaluation with unilateral hearing loss – a) Moderate to severe hearing loss b) Severe to profound hearing loss.
What are your challenges in interpreting the neuro-diagnostics ABR for the above patients?
Discuss your answers based on the findings of Bauch and Olsen (1986) study.
Bauch & Olsen demonstrated that as cochlear hearing loss increases, ABR becomes less reliable as a neurodiagnostic tool because cochlear factors cause “abnormal” ABRs even when the auditory nerve and brainstem are normal.
This makes interpretation particularly challenging in unilateral, asymmetric, or moderate-to-profound hearing loss.
Provide two limitations in performing ABR for neurodiagnostic applications among adults compared to MRI? (2)
ABR can miss small tumors
ABR findings are indirect and influenced by other factors like:
Cochlear HL
Age
Noise in the recording
Anatomical variability