MLS Exam #3 (M)
1/516
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
517 Terms
What is an essential tremor characterized by? Who is it usually seen in?
Most common movement disorder that usually presents as a b/l postural tremor of the hands followed by a tremor w/ action/movement (can also affect head, voice, & other areas); often seen in young people w/ a family hx
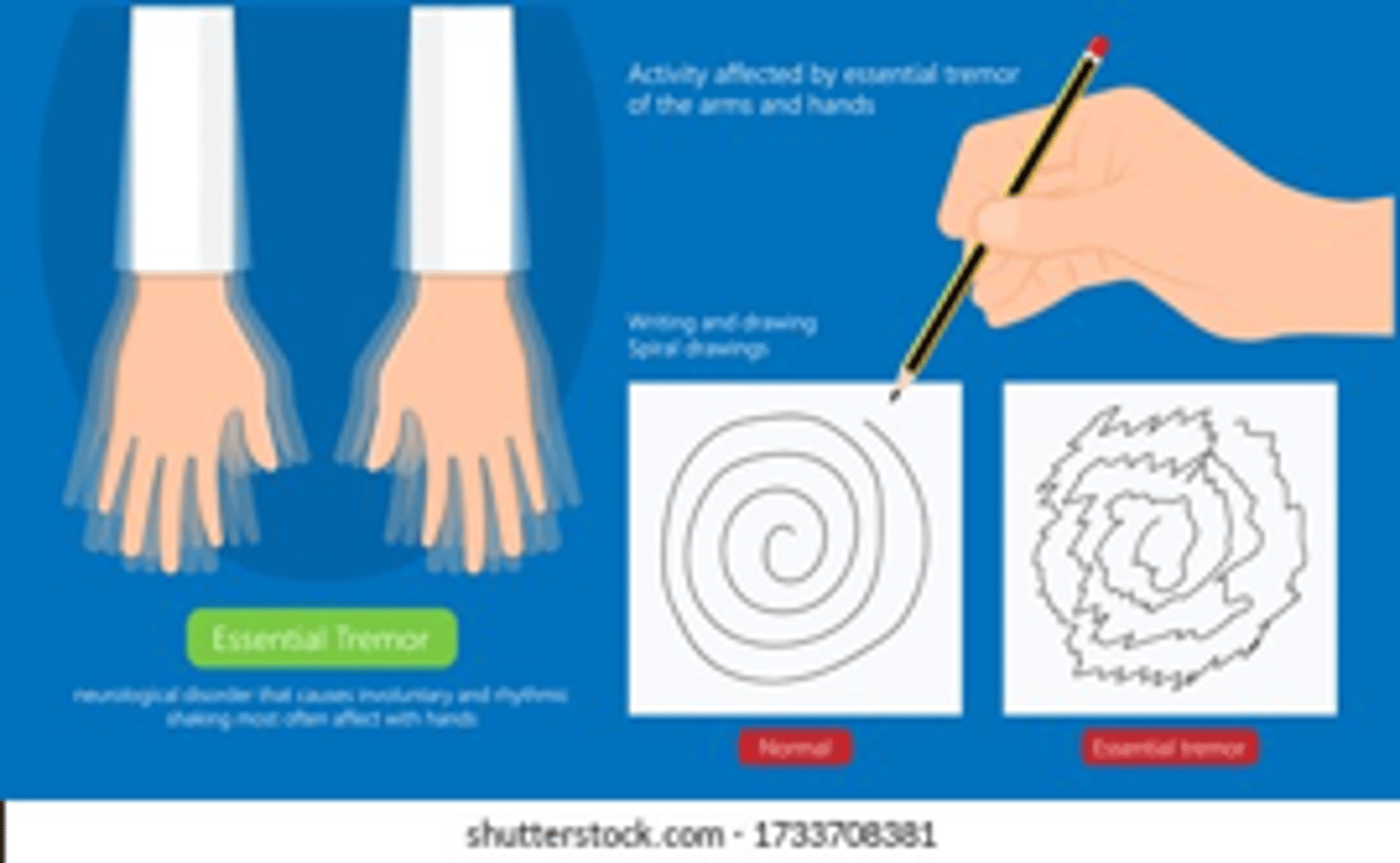
What will be seen on physical exam in a patient with essential tremor? What is a particular lab test we should in patients w/ this condition?
Tremor w/ the arms suspended against gravity that is exacerbated by goal-directed activity; thyroid function tests
If an essential tremor is serious enough to warrant pharmacologic therapy, which 2 agents are first-line treatment options?
Propranolol (beta-blocker) or primidone (barbiturate - CNS depressant)
What are some contraindications to propranolol & primidone, respectively?
Propranolol: lung pathologies (asthma, COPD, etc.), bradycardia, conduction block, diabetes
Primidone: porphyria, severe respiratory depression, alcoholism, drug dependence
What is the most common surgical treatment for essential tremor?
Deep brain stimulation (DBS) - very effective
What is Parkinson disorder (PD), & what is it caused by?
Progressive disorder caused by dopamine deficiency due to neurodegeneration in the substantia nigra
Is the cause of neurodegeneration as seen in PD known?
No - is thought to be a combination of genetic & environmental factors tho
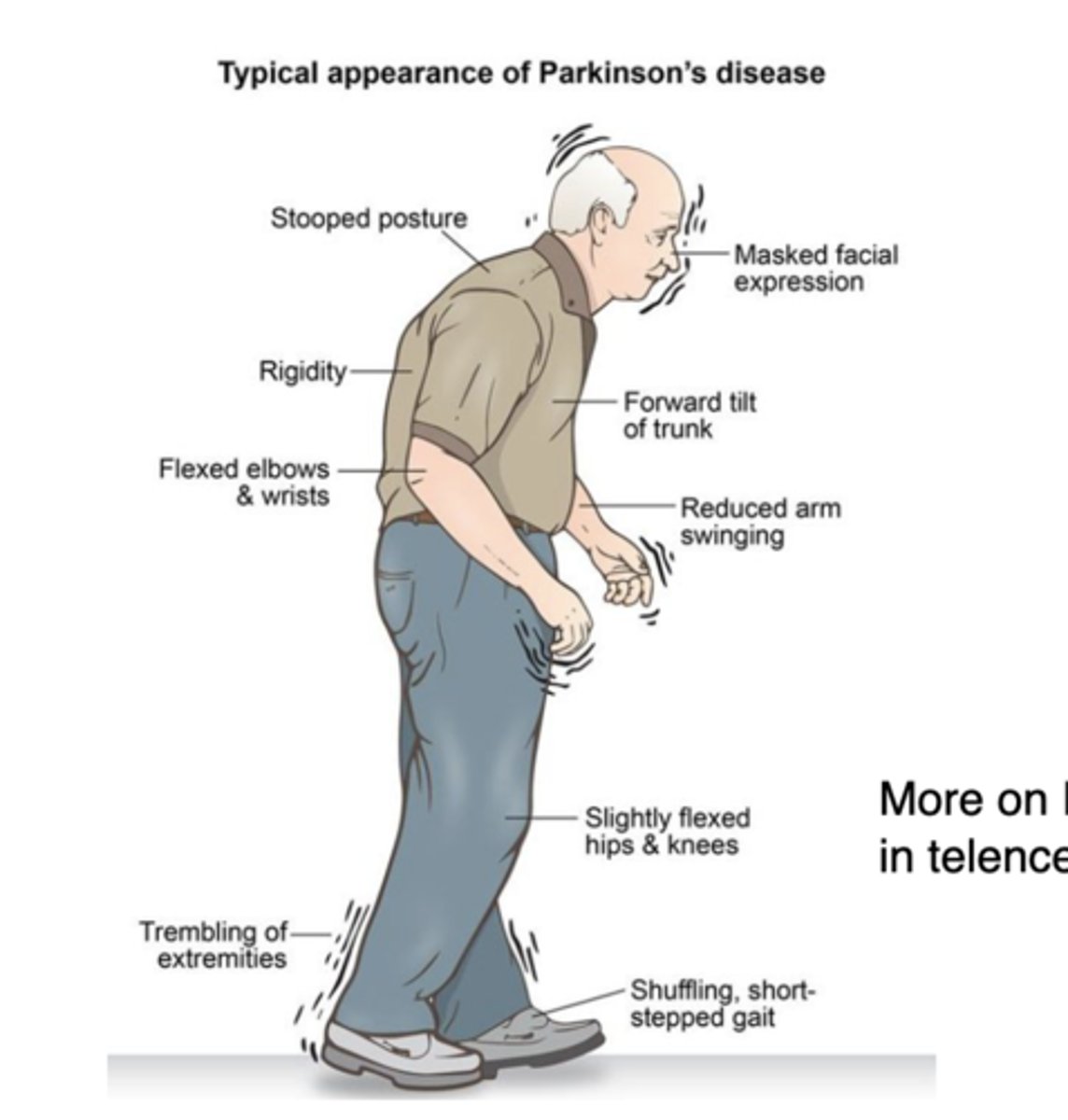
What are some of the s/sxs of PD?
Unilateral resting hand tremor ("pill-rolling"), progressive bradykinesia, rigidity, dystonia, gait difficulty (shuffling, short stride & flexed), masked facies, ipsilateral ↓ arm swing
What are the 3 cardinal signs of PD (2 of which must be met to make a clinical diagnosis)?
1) Resting tremor
2) Rigidity
3) Bradykinesia
Do we normally need to perform imaging/labwork to make a diagnosis of PD?
Not for patients w/ a typical presentation (may still be done to r/o things like a mass, stroke, etc.)
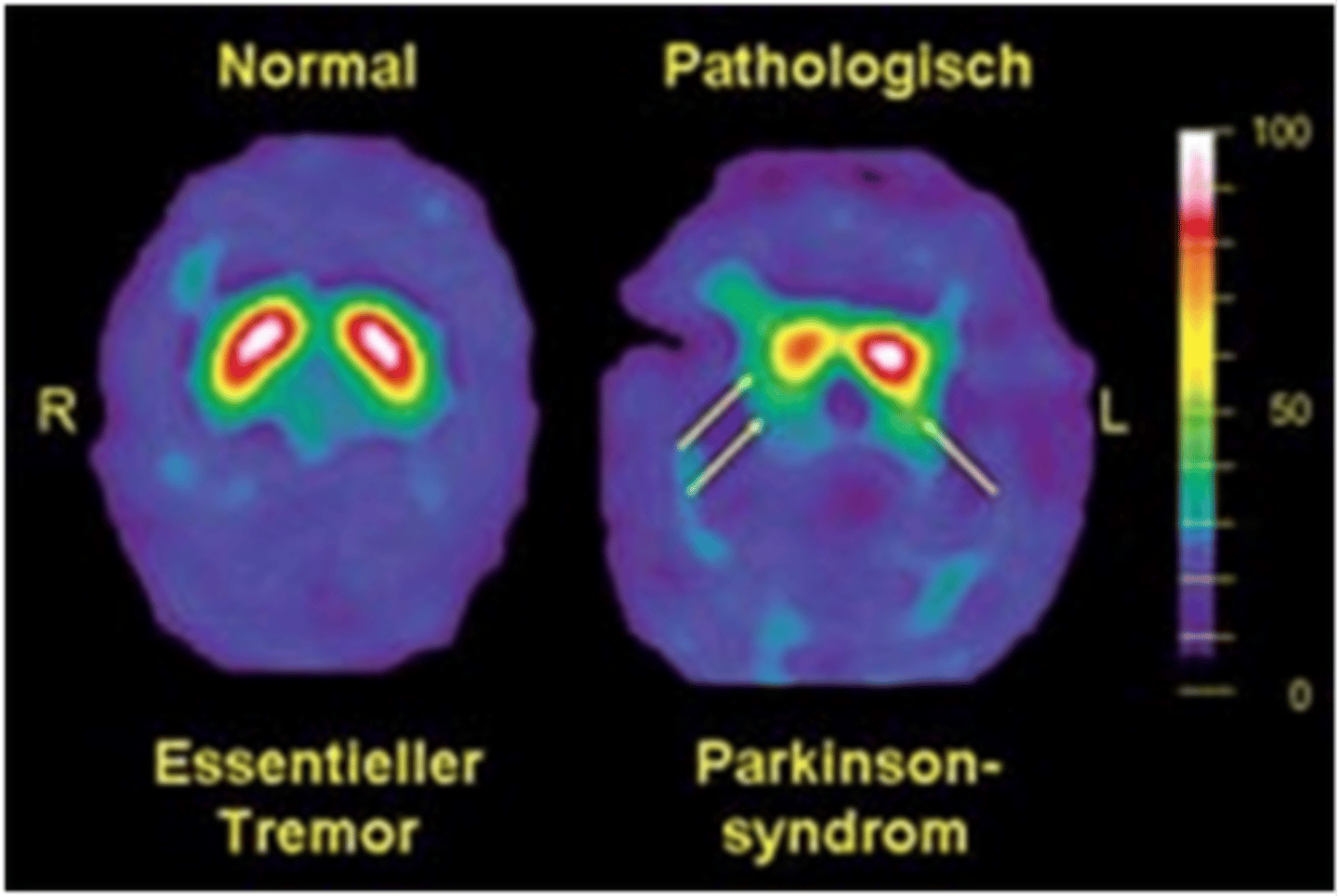
What are dopamine transporter (DaT) & single-photon emission computed tomography (SPECT) scans used for?
Nuclear scans that can help diagnose cases of uncertain parkinsonism (usually only used in big research centers)
What is the gold-standard medication to treat the motor sxs of PD? How long will this med (& most anti-PD meds for that matter) be effective for?
Levodopa paired w/ carbidopa; usually ~4-6 years, but after that they won't be as effective & disease unfortunately progresses
What are a few dopamine agonists that may be used to treat PD? What is a unique side effect of these meds?
Pramipexole, ropinirole, rotigotine; impulse control issues (excessive gambling, hypersexuality, etc.)
What are 2 monoamine oxidase (MAO)-B inhibitors that may be used to treat PD?
Selegiline, rasagiline
What is the most common surgical technique used to treat PD?
Deep brain stimulation (DBS)
What are 2 medications/drug classes that can worsen PD sxs due to their dopamine-antagonist activity?
Metoclopramide; neuroleptics (antipsychotics)
In general, what are extrapyramidal side effects (EPSEs)? What drug classes are they commonly associated w/?
Drug-induced movement disorders; centrally-acting dopamine receptor antagonists (such as 1st-gen antipsychotics haloperidol & phenothiazine neuroleptics)
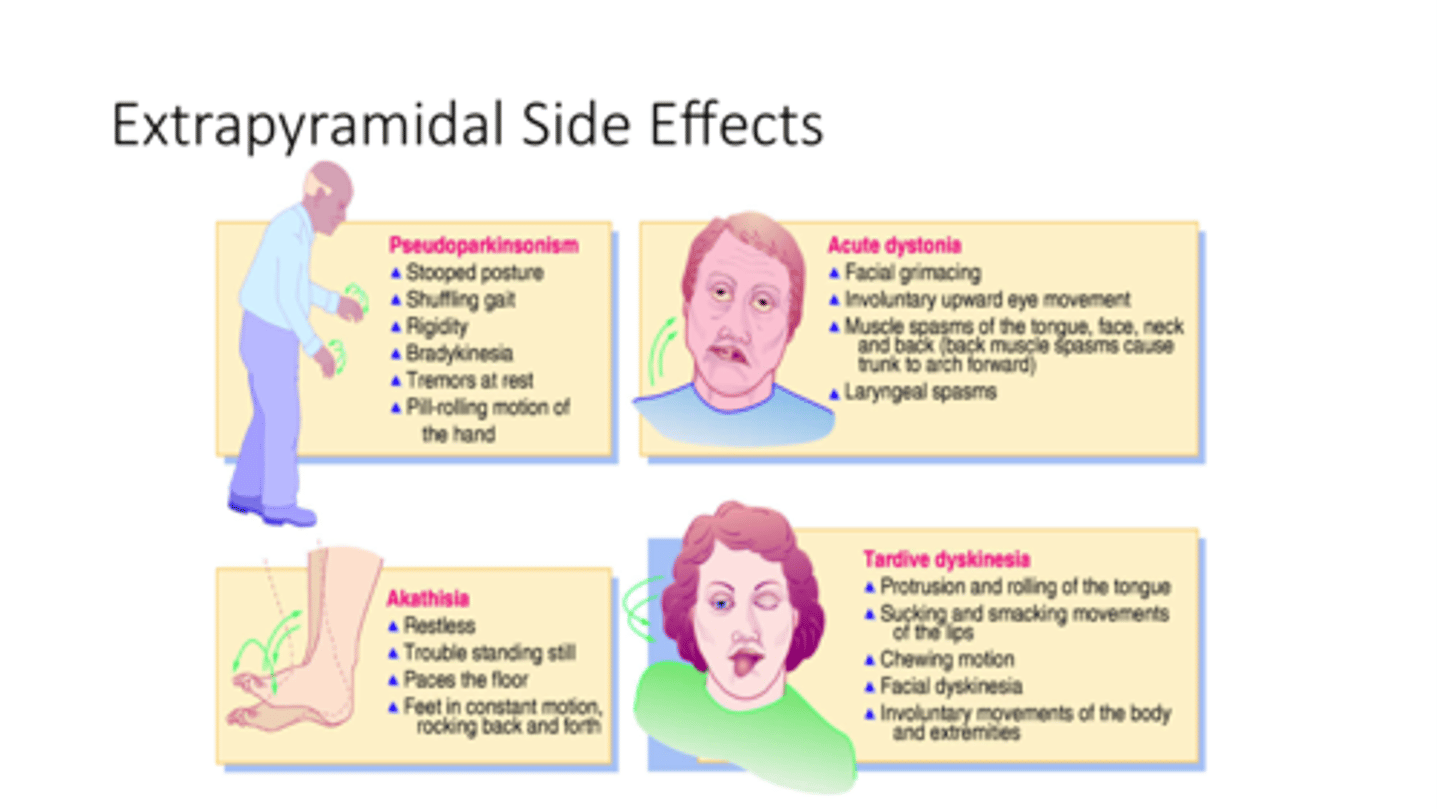
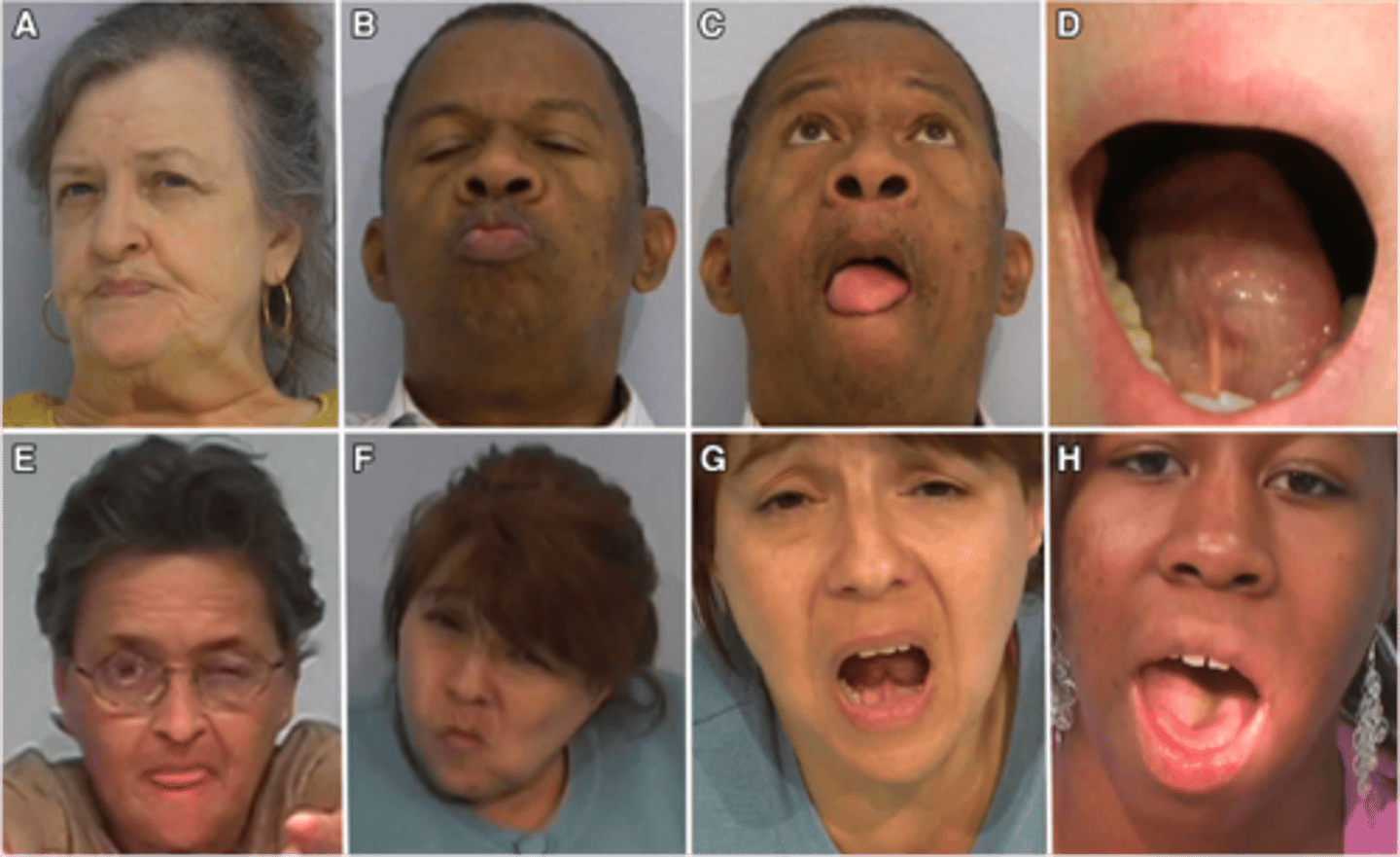
What is tardive dyskinesia, & what is it often associated with?
Iatrogenic movement disorder causing involuntary, repetitive movements of the mouth, tongue, face, trunk, & limbs; neuroleptic (antipsychotic) use
What is an acute dystonic reaction, & what is it often associated with?
Involuntary muscle contractions resulting in abnormal posturing or repetitive movements; associated w/ meds
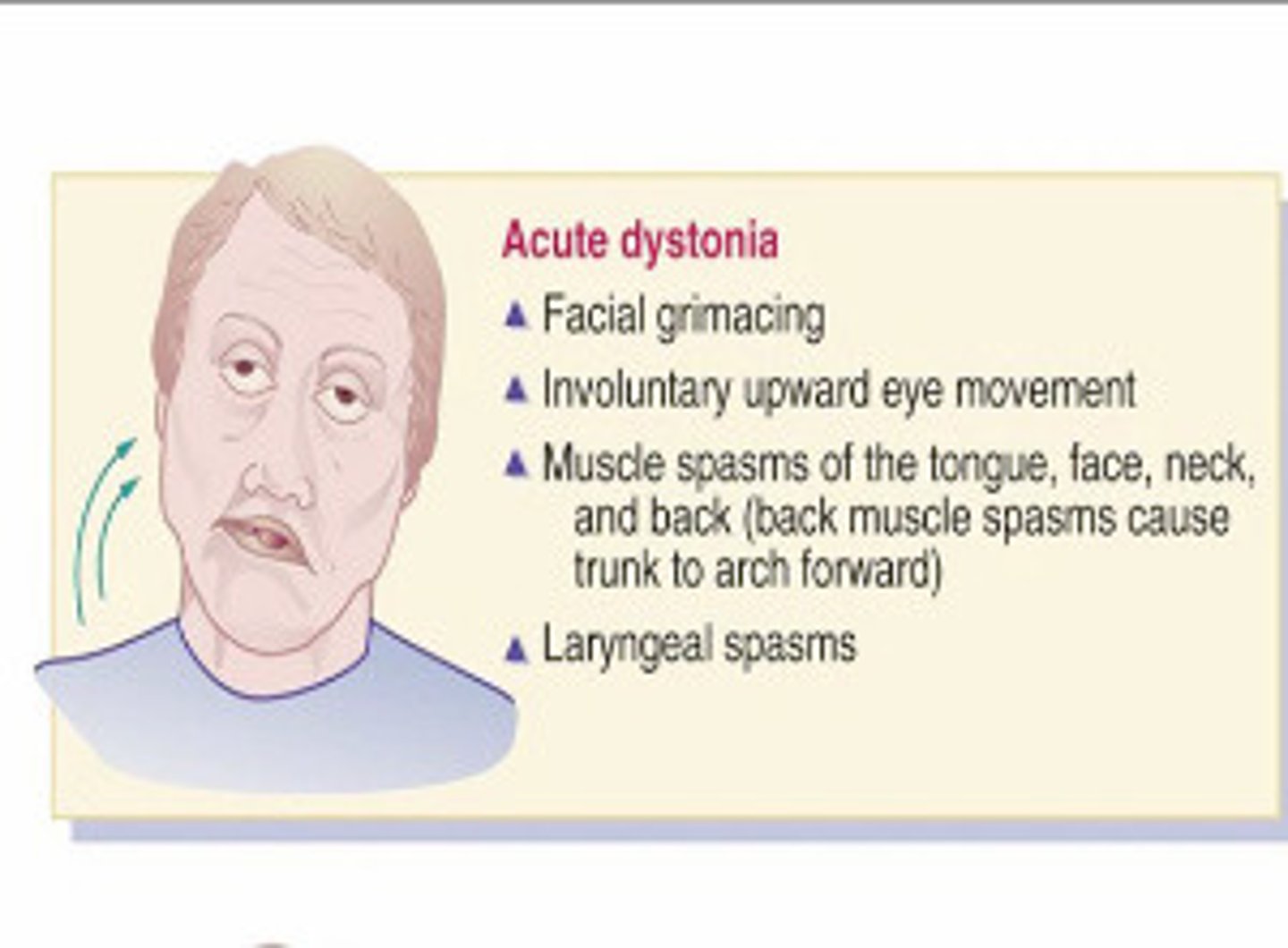
What is a medication that can be given in an acute dystonic reaction that rapidly-reverses the effect?
Diphenhydramine
What is dystonia (ex. torticollis)? What is our first-line treatment?
Involuntary maintained contraction of the agonist & antagonist muscles causing abnormal posturing, twisting/repetitive movements, or tremulous; botulinum toxin injections
What is the classic triad of s/sxs seen in dementia w/ Lewy bodies?
1) Parkinsonism (at same time as cognitive impairment)
2) Fluctuating cognitive impairment
3) Visual hallucinations
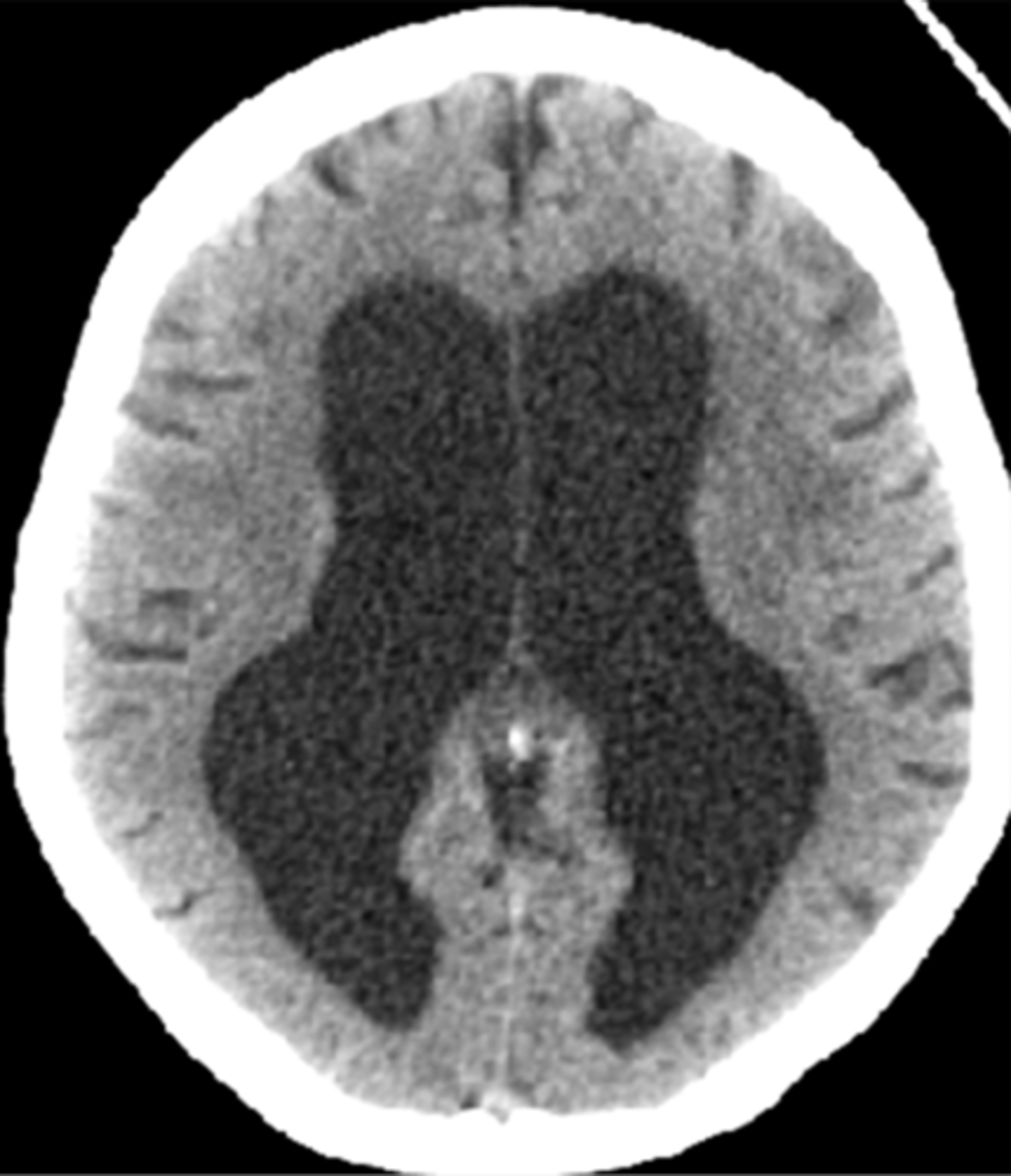
What is the classic triad of s/sxs seen in normal pressure hydrocephalus? What will be seen on imaging?
1) Gait instability
2) Urinary incontinence
3) Dementia
Hydrocephalus w/ minimal cortical atrophy (fluid buildup out of proportion to atrophy)
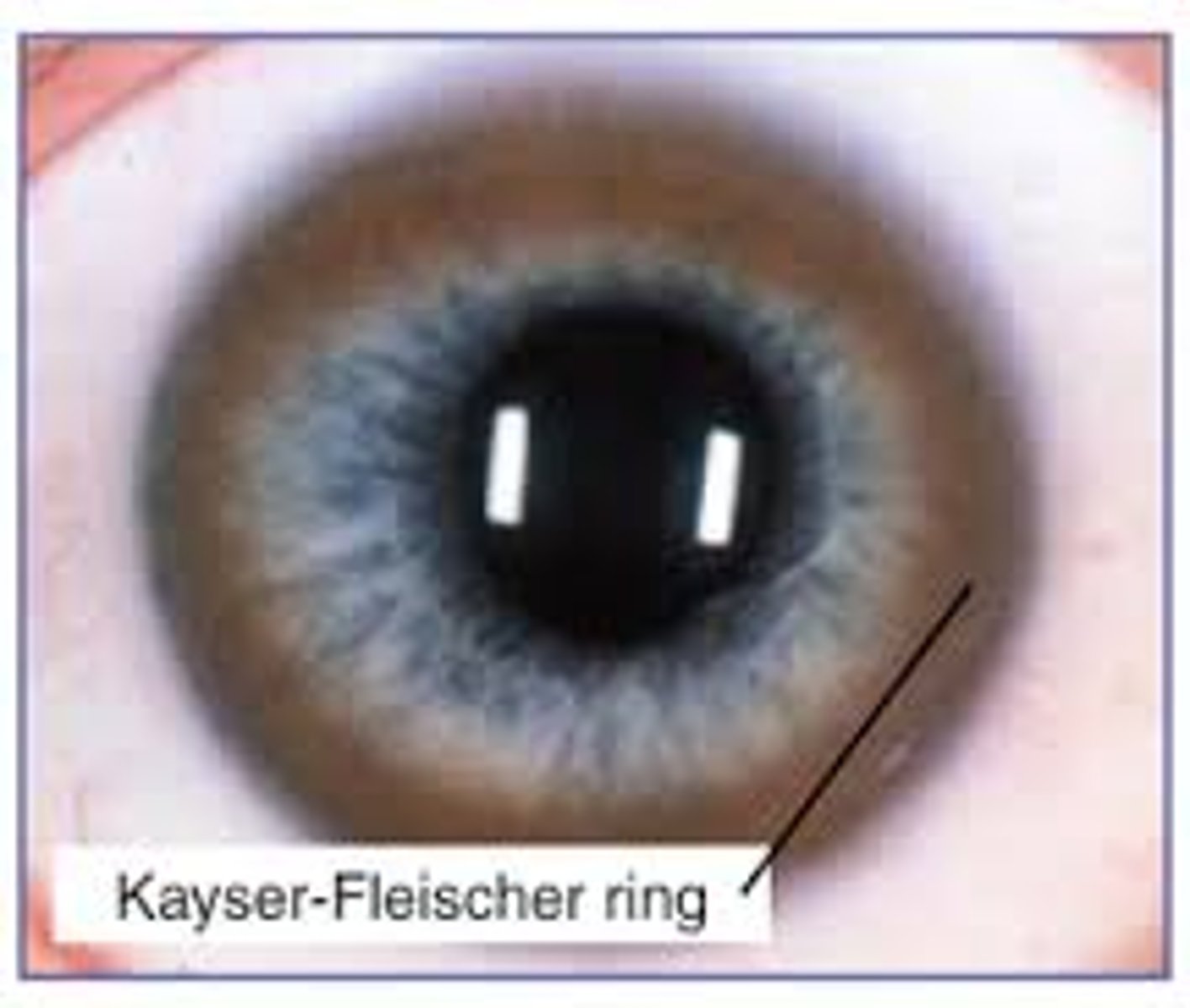
What is Wilson disease? What are some clinical presentation features that may clue us in to this disease?
Disorder of copper metabolism leading to its accumulation; onset of parkinsonism before age 40, Kayser-Fleischer rings in eye, wing-beating tremor

What is progressive supranuclear palsy (PSP) characterized by?
Primarily vertical gaze deficits, parkinsonism, unexplained falls

JUST KNOW: multiple system atrophy (MSA) & corticobasal syndrome are both neurodegenerative disorders we should have in our differential, but they are super rare & Hoppe barely talked about them
What is Huntington disease, & what is a triad of s/sxs?
Autosomal dominant disorder characterized by a chromosome 4 defect in the huntingtin gene; gradual onset of (1) chorea, (2) dementia, & (3) behavioral changes
How is Huntington disease definitely diagnosed? Is there a cure?
Genetic testing; no - can manage chorea & other sxs but not cure them
In general, what are tics? Is suppressing them helpful?
Sudden, brief stereotypical involuntary movements or sounds that occur repeatedly; no - can actually exacerbate them
What is Tourette syndrome, & what is it characterized by? How is it treated?
Neurodevelopmental disorder characterized by multiple motor or vocal tics that begin in childhood & last at least 1 year; will usually respond to behavioral intervention before meds are needed
What is pediatric autoimmune neuropsychiatric disorder associated w/ streptococcal infections (PANDAS), & what is it associated with?
Acute onset of neuropsychiatric sxs (usually tics or OCD) in childhood following a streptococcal infection
What is restless leg syndrome characterized by? What is it often associated with?
Patients have an irresistible urge to move legs that is worse at night or with rest; iron deficiency

How is restless leg syndrome treated?
Iron supplementation (if deficient); gabapentinoids (gabapentin or pregabalin) are 1st-line
In terms of acute liver failure, what are the criteria for the fulminant, subfulminant, & acute-on-chronic categorizations, respectively?
Fulminant: encephalopathy & coagulopathy (in addition to liver failure) within 8 weeks of acute liver injury
Subfulminant: encephalopathy & coagulopathy (in addition to liver failure) between 8 weeks - 6 months after acute liver injury
Acute-on-Chronic: acute deterioration in liver function in someone w/ pre-existing liver disease
What are the 2 biggest causes of acute liver disease?
#1 = acetaminophen (APAP), #2 = idiosyncratic drug reactions (unexpected drug reaction)
What is Reye syndrome, & what is it caused by?
Rare case of hepatic encephalopathy associated w/ ASA use during acute viral infections (esp. influenza or VZV)
What is asterixis?
"Liver flap" involuntary jerking of hand that can indicate liver disease
What are some diagnostic findings of acute liver failure?
Extremely elevated AST & ALT (DeRitis ratio can d/dx), amylase may be elevated, PT/INR will likely be prolonged due to coag factor deficiency, serum NH3 will be elevated
Can acute liver failure be monitored in an outpatient setting?
No - requires immediate hospitalization
What is an agent that can be administered to reduce NH3 levels (if applicable) in acute liver failure? What about to reverse the effects of APAP toxicity?
Reduce NH3: lactulose
APAP antidote: N-acetylcysteine (NAC)
What are the leading causes of death in patients w/ acute liver failure?
Cerebral edema & sepsis/SIRS
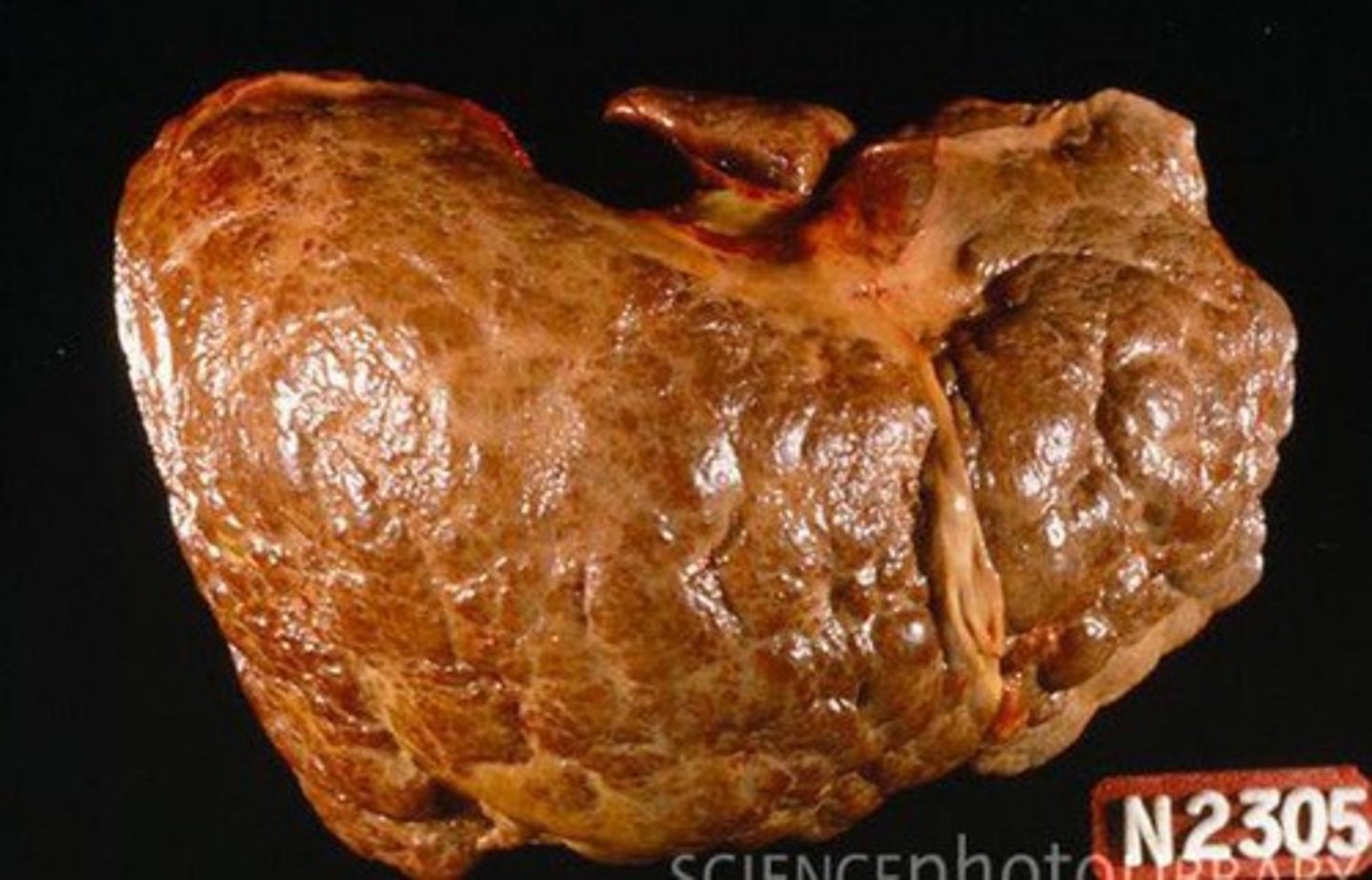
What is cirrhosis, & what is it characterized by?
Chronic "late-stage" liver disease due to ongoing hepatocellular injury & inflammation leading to fibrosis, scarring/distortion of hepatic architecture, & nodule formation
What are some general possible causes of cirrhosis? What are some possible complications?
Chronic Hep B/C, alcohol, MAFLD/MASH; portal HTN, volume overload, coagulopathy, encephalopathy, hepatocellular cancer
What are some possible s/sxs of liver cirrhosis?
Upper GI bleeding, fetor hepaticus, spider angiomas, palmar erythema, pleural effusion, gynecomastia, ascites, caput medusae, hepatomegaly, splenomegaly, testicular atrophy, peripheral edema, asterixis
What is fetor hepaticus?
Rotten, musty odor of decay sometimes on the breath of patients w/ cirrhosis
What is caput medusae?
Varicose enlargement of periumbilical veins due to portal HTN sometimes seen in patients w/ liver cirrhosis

What are some lab findings of liver cirrhosis? What is the definitive diagnostic tool?
Thrombocytopenia, AST/ALT ratio > 1, progressive ↑ in bilirubin, ↓ albumin, prolonged PT/INR; liver biopsy
What is the METAVIR scoring system used for? What are the 2 categories it assesses?
Assesses severity of liver (1) inflammation & (2) fibrosis to grade necessity of transplantation
How is cirrhosis managed/treated?
Address underlying cause, protect liver (avoid hepatotoxic agents, HAV & HBV vaccines, etc.), manage complications
What are some things that can be done to manage third-spacing, portal HTN/variceal bleeding, encephalopathy, & coagulopathy as complications of cirrhosis, respectively?
3rd-spacing: furosemide, spironolactone/eplerenone
Portal HTN/variceal bleeding: non-selective beta-blockers, octreotide
Encephalopathy: lactulose
Coagulopathy: FFP
What classification is eligible for liver transplantation using the Child-Pugh Score & Classification? What about using the Model for End-Stage Liver Disease (MELD) score?
Child-Pugh: class B7-9
MELD: score of 17+
Which Hepatitis viruses are RNA viruses & which are DNA?
All are RNA except Hep B (which is a DNA virus)
How is each Hepatitis virus (A-E) transmitted?
A: fecal-oral
B: infected body fluids
C: bloodborne (esp. IV drug use)
D: infected body fluids (esp. blood)
E: fecal-oral or zoonotic
What is unique about the transmission/infectivity of Hep D?
It can only cause infection if the HBsAg is present
Although Hep E is not seen frequently in the US, is it common worldwide?
YES - is the most common cause of acute viral hepatitis worldwide!
Which Hepatitis viruses are most at risk of producing a chronic disease state? Are there any that will 100% not do this?
Hep B & C have high rates of chronic disease; Hep A does not have a chronic state
Polyarteritis nodosa (PAN), Guillain-Barre syndrome, & a serum sickness-like reaction (SSLR) are possible complications of which Hepatitis virus?
Hep B

What will the AST/ALT ratio be cases of viral hepatitis?
< 1 (d/dx from cirrhosis)
JUST KNOW: look at the CS viral hepatitis PPX to learn the diagnostic markers for each Hepatitis virus type
How is viral hepatitis managed? Are there any strains that antiviral therapy is effective against?
Patient education & supportive care; YES - Hep C they are the mainstay of treatment (& case-by-case basis for B & D)
How is Hep A prevented? Is there a recommended routine screening method for this strain?
HAV vaccine; no, none at the moments
How is Hep B prevented? Is there a recommended routine screening method for this strain?
HBV vaccine; yes - done in all adults at least once in their lifetime, all pregnant patients, neonates born to HBsAg-negative mothers, & people w/ exposure risk
How is Hep C prevented? Is there a recommended routine screening method for this strain?
There is no vaccine; yes - done in all adults at least once in their lifetime, all pregnant patients, & those who are high-risk or have had exposure
What is the prognosis of viral hepatitis like?
Acute disease is usually self-limited (depending on patient's risk factors obviously), but chronic disease can lead to cirrhosis & hepatocellular cancer
What is alcohol-associated liver disease (ALD)? Why is it clinically-significant?
Spectrum of disease causing steatosis, hepatitis, steatohepatitis, and/or cirrhosis due to excessive alcohol intake; is the most common precursor to cirrhosis in the US (& also the most common reason for liver transplant during COVID pandemic)
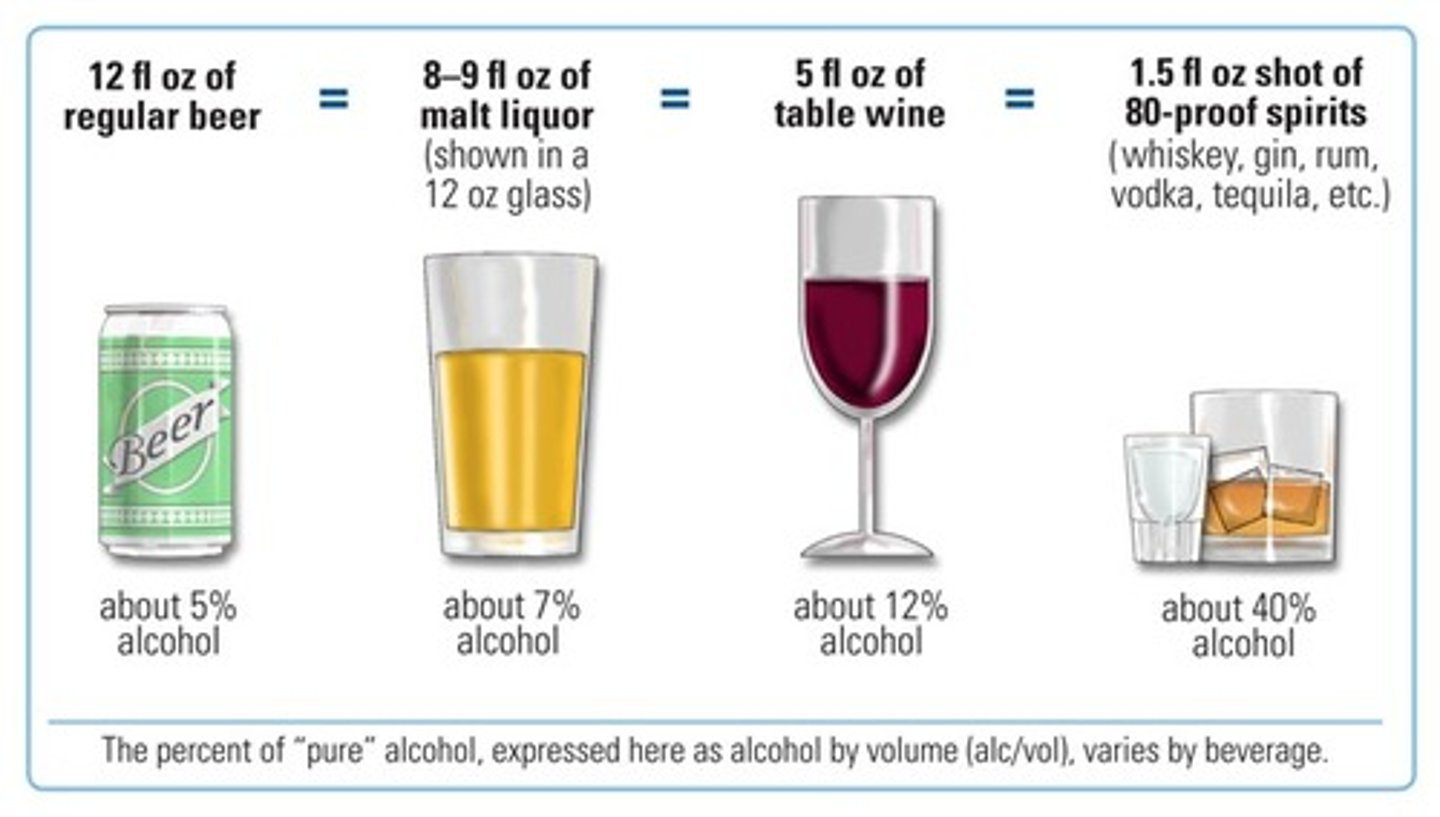
What amount of alcohol is considered to be 1 standard drink in the US? "Excessive alcohol consumption" is considered to be an intake of what?
1 drink = 14g of alcohol
Excessive intake = ≥ 30 g/day (aka 2+ drinks each day)
What is the actual toxic alcohol metabolite that causes liver damage? What enzyme is responsible for producing this metabolite?
Metabolite: acetaldehyde
Enzyme: alcohol dehydrogenase (ADH)
Do sxs of ALD usually present early on?
NO - not usually until severe damage has already occurred (hepatomegaly may be possible early sign)
What is Wernicke-Korsakoff syndrome (WKS), & what is it caused by? What is a classic triad of sxs?
Neuropsychiatric disorder of severe thiamine (B1) deficiency often associated w/ alcohol abuse; (1) confusion/delirium, (2) oculomotor dysfunction (nystagmus, etc.), (3) ataxia
How is WKS treated?
Emergency IV thiamine
What do we expect the AST/ALT ratio to be in ALD? What is another serum marker than can indicate heavy alcohol use? What would be the definitive diagnosis of ALD?
Ratio > 2:1; gamma-glutamyl transferase (GGT); liver biopsy
How is ALD treated/managed?
Abstinence from alcohol is critical; counseling should be offered
What is drug-induced liver injury (DILI) & how can it manifest?
Exactly as it sounds - damage to the liver due to drug/medication use; can be direct toxicity (like w/ APAP & ETOH), idiosyncratic (unexpected), or indirect (exacerbates prior disease)
In DILI, what R value would indicate a cholestatic, hepatocellular, & mixed liver injury, respectively?
Cholestatic: R value < 2
Hepatocellular: R value > 5
Mixed: R value 2-5
What are the 2 most common agents/drug classes implicated in DILI?
Antibiotics = #1, APAP
What is the definitive diagnosis for DILI like? What is the prognosis like?
Liver biopsy; generally good - most cases can be reversed w/ d/c of the offending agent
What are metabolic-associated fatty liver disease (MAFLD) & metabolic-associated steatohepatitis (MASH)?
Spectrum of liver disease leading to steatosis (MAFLD), fibrosis, steatohepatitis (MASH), and/or cirrhosis PLUS at least one component of metabolic syndrome is present
What is the biggest risk factor to develop MAFLD/MASH?
Insulin resistance (& obesity)
What is a lifestyle change patients can make that protects against MAFLD?
Physical activity (even if you're not losing weight!)
Are most patients w/ MAFLD/MASH symptomatic? What AST/ALT ratios do we expect to see if the patient has steatosis vs. fibrosis/cirrhosis?
No - most are asymptomatic; steatosis = ratio < 1 (d/dx from viral hepatitis via a hepatitis panel), fibrosis/cirrhosis = ratio > 1
What is the definitive diagnosis for MAFLD/MASH? What is the cornerstone of therapy?
Liver biopsy; lifestyle modifications are essential
What is a drug that was recently FDA-approved to help improve insulin resistance and/or weight gain in patients with MASH + moderate/severe fibrosis?
Resmetriom
What is hemochromatosis, & what is it charactezied by?
Genetic disorder leading to ↑ iron absorption in the duodenum & subsequent progressive iron accumulation in tissues & organs
How is hemochromatosis usually diagnosed? What is a significant possible complication (at least in terms of the liver)?
Usually in the asymptomatic phase due to incidental lab findings & a positive FMHX; cirrhosis (and all the problems that go with it)
What are some diagnostic studies we can do to diagnose hemochromatosis?
Iron studies (↑↑ ferritin possible), AST & ALT mildly elevated, MRI to visualize iron deposits & liver damage
What is our mainstay of treatment for hemochromatosis? What is an alternative if patients are comorbid anemia?
Regular phlebotomy = 1st-line; iron chelation therapy
What is Wilson disease, & what is it characterized by?
Genetic disorder of copper clearance leading to copper accumulation in the liver, brain & cornea
What is a key physical exam finding of Wilson disease?
Kayser-Fleischer rings in cornea
In terms of diagnosing Wilson disease, what levels do we expect to see of serum ceruloplasmin & urinary copper excretion (24-hr)?
Ceruloplasmin: decreased (protein that actually binds copper in the bloodstream)
Urinary excretion: increased (kidneys try to compensate but it's still not enough)
Is a liver biopsy usually needed to diagnose Wilson disease?
No, not unless labs are inconclusive
What is a copper chelating agent that can be administered to treat patients w/ Wilson disease who are symptomatic or have organ damage? What else must we give the patient with this drug?
D-penicillamine; also give them Vit. B6 (pyridoxine) since this drug depletes B6
What are considered normal oral, rectal, tympanic, axillary, & forehead (infrared) temperatures, respectively?
Oral: 98.6 F (37C)
Rectal: 99.6 F (most reliable)
Tympanic: 99.6 F
Axillary: 97.6 F
Infrared: 97.6 F
As a general rule of thumb, what temperature is considered to be a "fever?"
Temp > 100.4 F (38 C)
Is a fever considered a diagnosis?
NO - it is a sign/symptom
What are the diagnostic criteria for a classic fever of unknown origin (FUO)?
1) Illness of at least 3 weeks duration
2) Temperature > 38.3 C (101 F)
3) Diagnosis has not been made after 3 outpatient visits/days in the hospital
Although FUOs are of an "unknown origin" by definition, what tends to be the most common cause?
Infectious organisms (TB is the most common one)
What is the most common infectious etiology of a FUO?
TB (others possible too)
What are the most common autoimmune etiologies of a FUO?
Temporal arteritis, juvenile rheumatoid arthritis, systemic lupus erythematosus
What are the most common neoplastic etiologies of a FUO?
Lymphoma, renal cell carcinoma, melanoma
What are the most common miscellaneous etiologies of a FUO?
Medications, chronic PE, hyperthyroidism