Unit 6 - Human Physiology
1/140
Earn XP
Description and Tags
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
141 Terms
Alimentary Canal
Organs through which food passes:
Oesophagus
Stomach
Small & large intestine
Oesophagus/Esophagus
A hollow tube connecting the oral cavity to the stomach and is separated from the trachea by the epiglottis.
In it, food is mixed with saliva and moved in a bolus via peristalsis.
Stomach
Temporary storage tank where food is mixed by churning and protein digestion begins.
Lined with gastric pits w/ digestive juices —> pH~2
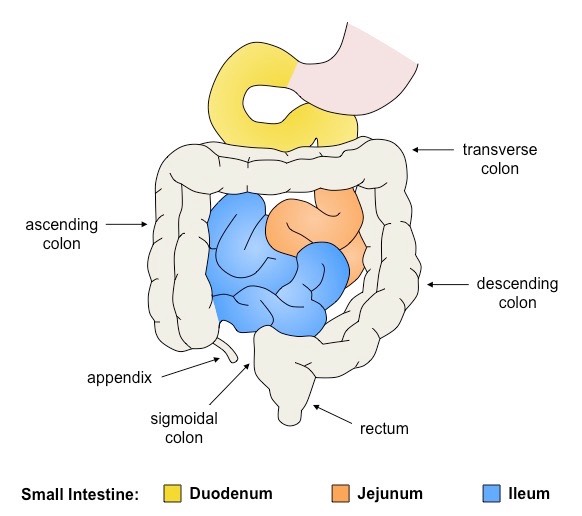
Small Intestine
A long, highly folded tube where usable food substances (nutrients) are absorbed.
Sections: Duodenum (first segment with digestive juices from gall bladder and pancreas), jejunum (digestive process mostly completed), ileum (highly folded + bile absorbed and returned to liver via vessels).
Structure of Small Intestine
Serosa: Protective outer covering composed of cells reinforced by fibrous connective tissue.
Muscle layer: Outer layer of longitudinal muscle (peristalsis) and inner layer of circular muscle (segmentation)
Submucosa: Composed of connective tissue separating the muscle layer from the innermost mucosa.
Mucosa: Highly folded inner layer which absorbs materials through its surface epithelium from intestinal lumen.
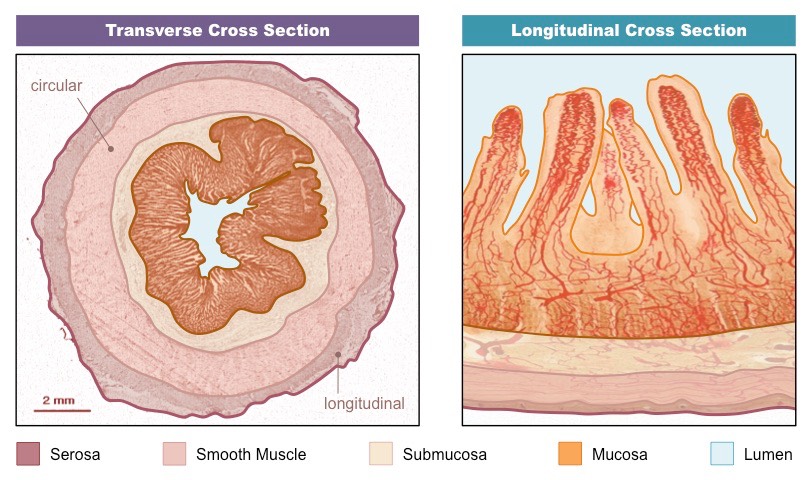
Villi
Finger-like projections from the folding of the inner epithelial lining of the intestine. → Protrude into the intestinal lumen = Increase SA for material absorption.
Features of Villi (6)
Microvilli: Ruffling of epithelial membrane = increases SA
Rich blood supply: Dense capillary network rapidly transports absorbed products.
Single layer epithelium: Minimises diffusion distance between lumen and blood.
Lacteals: Absorbs lipids from intestine into lymphatic system.
Intestinal glands: Exocrine pits (crypts of Liberkuhn) release digestive juices.
Membrane proteins: Facilitates transport of digested materials into epithelial cells.
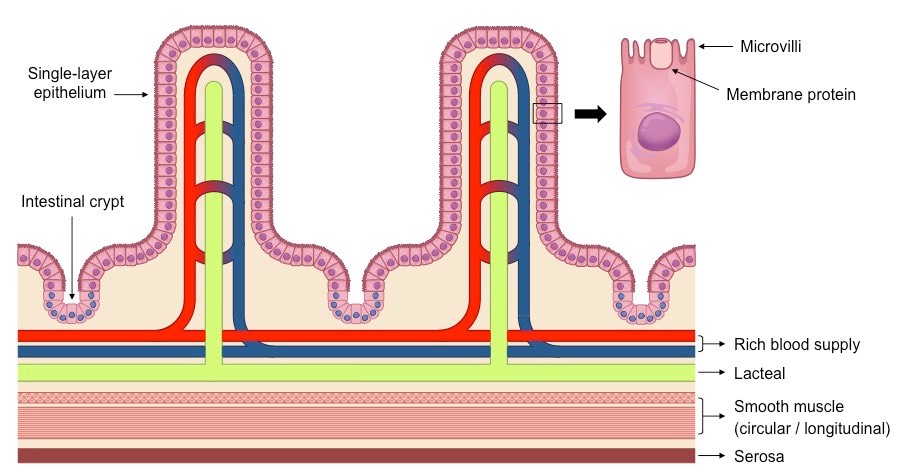
Structure of Villus Epithelium (5)
Tight Junctions: Occluding associations between plasma membrane of adjacent cells = impermeable barrier ( maintain concentration gradient).
Microvilli: Microvilli increase surface area of plasma membrane = more absorption
Membrane w/ digestive enzymes + channel proteins
Mitochondria: Epithelial cells have mitochondria = active transport.
Pinocytotic Vesicles: Uptake of fluids + dissolved solutes through ingestion (break down of membrane = vesicle)
Large Intestine
Final section of alimentary canal where water and dissolved minerals are absorbed.
Appendix + Ascending colon, transverse colon, descending colon, sigmoidal colon + rectum
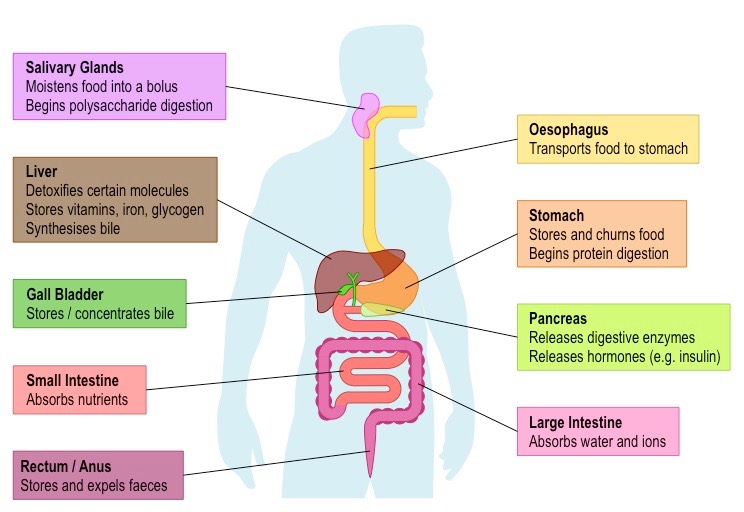
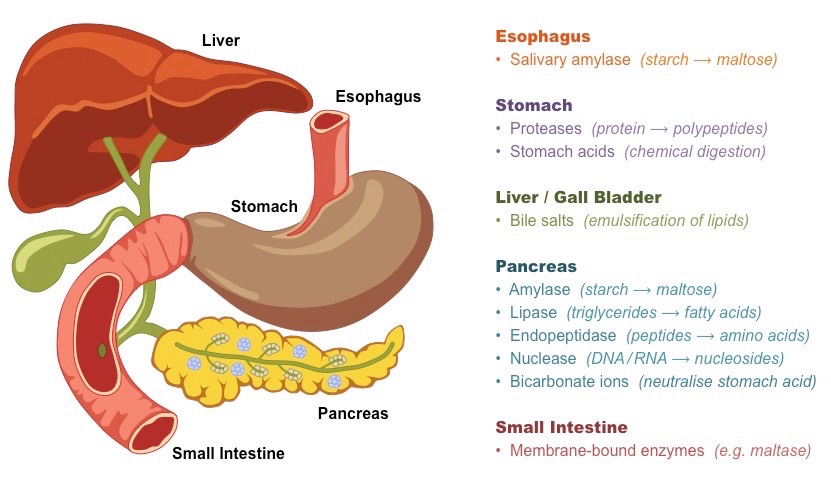
Accessory Organs
Aid in digestion but DO NOT TRANSFER food
Salivary glands, pancreas, liver, gall bladder.
Salivary Glands
Release saliva to moisten food and contains enzymes to initiate starch breakdown.
Include: Parotid gland, submandibular gland, and sublingual gland.
Pancreas
Produces broad spectrum of enzymes that are released into the small intestine via the duodenum.
Produces and secretes hormones like insulin and glucagon to regulate blood sugar concentrations.
Insulin: Lowers blood glucose levels by increasing glycogen synthesis + storage of glucose in liver & adipose tissues.
Glucagon: Increases blood glucose by limiting synthesis+storage.
Liver
Take the raw materials absorbed by the small intestine and uses them to make key chemicals.
Role: Detoxification, storage, metabolism, bile production and haemoglobin breakdown.
Gall Bladder
Stores the bile produced by the liver → Bile salts are used to emulsify fats.
Releases bile into the small intestine via the bile duct.
Drawing Digestive System
Stomach is a ‘J’-shaped bag and be connected to the oesophagus and small intestine
Liver should look like a right-angled triangle and be superimposed to the left of the stomach (right side of the human)
Bile duct (connected to gall bladder) and pancreatic duct should both feed into a U-shaped bend of the small intestine
Small intestine should be thinner in width than the large intestine
Mechanical Digestion
Food is physically broken down into smaller fragments.
Chewing (Mouth):
Mastication —> Grinding action of teeth
Tongue pushes bolus towards back of throat to esophagus.
Epiglottis prevents bolus from entering the trachea, and uvula prevents bolus from entering nasal cavity.
Churning (Stomach):
Stomach lined with muscles = physically squeeze+mix the food
Turned into chyme —> Enters small intestine where absorption occurs.
Movement of Food
Peristalsis
Peristalsis is the principal mechanism of movement in the oesophagus (but also stomach + gut)
Continuous segments of longitudinal smooth muscle rhythmically contract and relax = Food is moved unidirectionally along the alimentary canal (mouth to anus)
Segmentation
Segmentation involves the contraction and relaxation of non-adjacent segments of circular smooth muscle in the intestines = bi-directional chyme movement (mixing w/ digestive juices)
Can slow overall movement.
Chemical Digestion: Stomach Acids
Stomach contains low pH environment → Contains gastric glands = digestive acids.
Acidic environment = denature proteins + macromolecules = aid digestion.
Stomach epithelium contains mucous membrane = prevents acids from damaging the gastric lining.
Pancreas releases alkaline compounds → Neutralize acids as they enter intestine.
Bile
Liver produces bile that is concentrated within the gall bladder —> Released into intestine.
Bile contains bile salts = emulsifies fat globules into smaller droplets.
This emulsification = increase SA available for enzymatic activity.
Lipase vs. Bile
Lipase can only bind to lipid globules at their outer extremity (therefore, digestion of lipids IS SLOW)
However, bile have both hydrophobic + hydrophilic SURFACES.
Hydrophobic end = interact with lipids
Hydrophilic ends = prevents lipids from coalescing.
Enzymes
Carbohydrate: Amylase (salivary glands), enzymes for disaccharide hydrolysis immobilized on epithelial lining (small intestine), no enzyme capable of digesting cellulose.
Proteins: Release of proteases (~2 pH) in acidic pH of stomach; endopeptidases (small intestine) breaks down smaller polypeptide chains (pH~7).
Lipids: Occurs in intestines (emulsification of fat globules) → Digested by lipases from pancreas.
Nucleic Acids: Nucleases in pancreas.
Starch Digestion
Amylase digests amylose into maltose subunits and amylopectin into chains called dextrin.
Maltase on epithelial lining breaks these down into glucose monomers.
Membrane Transport Mechanisms: Secondary Active Transport
A transport protein couples the active translocation of one molecule to the passive movement of another (co-transport)
Glucose + amino acids are co-transported across the epithelial membrane by the active translocation of Na+
Membrane Transport Mechanisms: Facilitated Diffusion
Channel proteins help hydrophilic food molecules pass through plasma membrane.
Channel proteins are often situated near specific membrane-bound enzymes = localised concentration gradient.
Certain monosaccharides (e.g. fructose), vitamins and some minerals are transported by facilitated diffusion
Membrane Transport Mechanisms: Osmosis
Response to movement of ions & hydrophilic monomers (solutes) through liquids (water).
Small + large intestines.
Membrane Transport Mechanisms: Simple Diffusion
Hydrophobic materials move through hydrophobic portion of plasma membrane.
Lipids pass through lacteals.
Membrane Transport Mechanisms: Endocytosis
In intestines → Vesicles form around fluid via pinocytosis = materials ingested in en masse.
Circulation
Two distinct locations for blood transport
The left side of the heart pumps oxygenated blood around the body (systemic circulation) ==> Has a thicker myocardium (muscular wall) to pump blood further.
The right side of the heart pumps deoxygenated blood to the lungs (pulmonary circulation)
William Harvey’s Findings
Antiquated beliefs:
Arteries and veins are separate blood networks where veins pump natural blood (liver) and arteries pump heat (produced by heart).
Harvey’s findings:
Arteries and veins were part of interconnected network
Arteries pumped blood from heart.
Veins returned blood from heart.
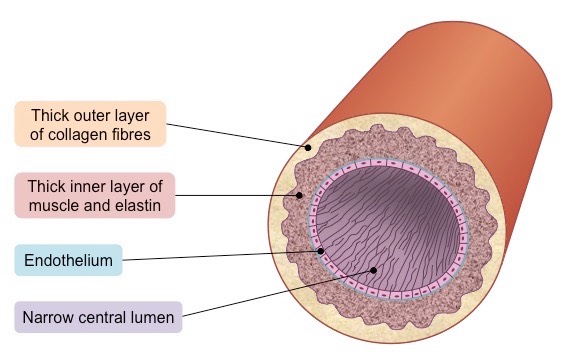
Arteries
Function: convey blood at a high pressure FROM heart ventricles to tissues in the body + lungs.
Structure of Arteries
Order: Outside to inside
Thick wall with outer layer of collagen to prevent rupturing from high pressure.
Arterial walls contain thick layer of inner muscle + elastic fibres to maintain pulse flow.
Endothelium: Thin membrane
Narrow lumen = maintain high blood pressure
Flow of Blood
Blood flows via pulses.
Muscle fibres:
Rigid arterial wall = withstand pressure.
Muscles can contract to narrow lumen = increase pressure between pumps as to maintain blood pressure.
Elastic fibres:
Allows arterial walls to stretch + expand in response to flow of pulse.
Pressure exerted on arterial wall = elastic recoil = push blood forward.
Capillaries
Exchange materials between tissues + blood travelling at a low pressure.
Arteries split —> Arterioles split —> Capillaries: Decreasing arterial pressure while total vessel volume increases.
Ensures every cell has a blood source.
Pool into venules which collate into larger veins when material exchange occurs.
Structures of Capillaries
Small diameter (~ 5 µm wide) which allows passage of only a single red blood cell at a time (optimal exchange)
Single layer of cells in capillary walls to minimise the diffusion distance.
Surrounded by a basement membrane which is permeable to necessary materials.
Differences:
Limit permeability: Capillary wall is continuous (endothelial cells with tight junctions)
Specialized for absorption (e.g. intestines, kidneys): capillary wall is fenestrated (contains pores)
Permeable to large molecules (e.g. in liver): sinusoidal and have open spaces between cells.
Flow of Blood in Capillaries
Blood flows through the capillaries slowly + low pressure = maximal material exchange
Higher hydrostatic pressure at the arteriole end = forces material from the bloodstream into the tissue fluid
Material that exits the capillaries at body tissues include oxygen and nutrients.
Lower hydrostatic pressure at the venule end = allows materials from the tissues to enter the bloodstream
Materials that enters the capillaries at body tissues include carbon dioxide and urea (wastes by cells)
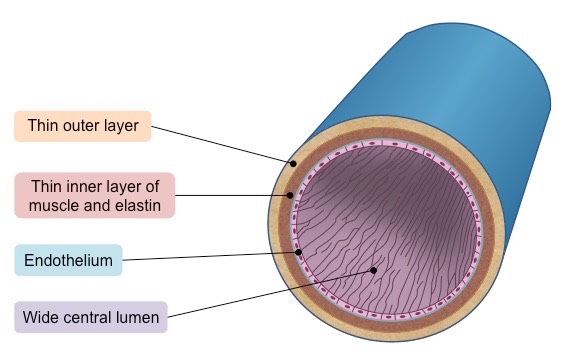
Veins
Function: Collect blood from tissues and convey at LOW pressure to atria of heart.
Structures of Veins
From outside to inside
Thin outer layer
Thin layer containing less muscle and elastic fibres as blood is at a very low pressure (~ 5–10 mmHg)
Endothelium
Very wide lumen (relative to wall thickness) to maximise blood flow for more effective return
Because the pressure is low, veins possess valves to prevent backflow and stop the blood from pooling at the lowest extremities
Flow of Blood in Veins
The veins contain one-way valves = maintain the circulation of blood by preventing backflow
Veins typically pass between skeletal muscle groups → Skeletal muscles contract = squeeze veins = cause blood to flow to site of compression.
Veins typically run parallel to arteries, and a similar effect can be caused by the rhythmic arterial bulge created by a pulse.
Blood Vessel Comparisons
Veins have thin walls but typically have wider lumen. → they transport blood at low pressure.
Arteries have thick walls and narrow lumens because they transport blood at high pressure → Arterial wall has three distinct layers (tunica)
Capillaries have walls that are only a single cell thick because they exchange materials between blood and tissue
Heart Structure: Chambers
Two atria (singular = atrium) – smaller chambers near top of heart that collect blood from body and lungs
Two ventricles – larger chambers near bottom of heart that pump blood to body and lungs
Heart Structure: Heart Valves
Atrioventricular valves – bicuspid valve on left side ; tricuspid valve on right side
In middle of atria and ventricles
Semilunar valves – aortic valve on left side ; pulmonary valve on right side
In middle ventricles and arteries
Heart Structure: Blood Vessels
Vena cava (inferior and superior): feeds into the right atrium and returns deoxygenated blood from the body.
Pulmonary artery connects to the right ventricle; deoxygenated blood to the lungs.
Pulmonary vein feeds into the left atrium = returns oxygenated blood from the lungs
Aorta extends from the left ventricle and sends oxygenated blood around the body.
Heart Contraction
Contraction of heart is myogenic: signal for cardiac compression arises within heart by cardiomyocytes.
Controlled by sinoatrial nodes (SA Node) = primary pacemaker = controlling rate of heart beats (60-100 cardiac contractions/min).
SA node —> AV node (secondary pacemaker) —> Bundle of His (third pacemaker)
Fibrillation
Interference of pacemaker = irregular/uncoordinated contraction of heart muscle.
Defibrillation
When fibrillation occurs, normal sinus rhythm may be re-established with a controlled electrical current.
Electrical Conduction of Heart Beat
The sinoatrial node=sends out an electrical impulse that stimulates contraction of the myocardium.
This impulse directly causes the atria to contract and stimulates atrioventricular node (AV node) between the atrium and ventricle
AV node sends signals down the septum via Bundle of His.
The Bundle of His innervates nerve fibres in the ventricular wall = contraction forcing blood up.
—> Delay between atrial + ventricular contractions = time to maximize blood flow (in ventricle)
Nerve Signalling + Heart Rate
The pacemaker is under autonomic control from the brain → medulla oblongata (brain stem)
Two nerves connected to the medulla regulate heart rate:
The sympathetic nerve: releases the neurotransmitter noradrenaline=increase heart rate
Also stimulates adrenaline hormone from adrenal glands
The parasympathetic nerve (vagus nerve): releases the neurotransmitter acetylcholine=decrease heart rate
Hormonal Signalling + Heart Rate
Hormones are chemical messengers released into the bloodstream that act specifically on distant target sites.
Heart rate can undergo a sustained increase in response to hormonal signalling in order to prepare for vigorous physical activity
Adrenaline (a.k.a. epinephrine) is released from the adrenal glands (located above the kidneys) → stimulate SA node = increases heart rate.
Other factors affecting heart rate
Nerve signals= trigger rapid changes; endocrine signals=trigger more sustained changes
Changes to blood pressure levels or CO2 concentrations (and thereby blood pH → Picked up by sensors) will trigger changes in heart rate
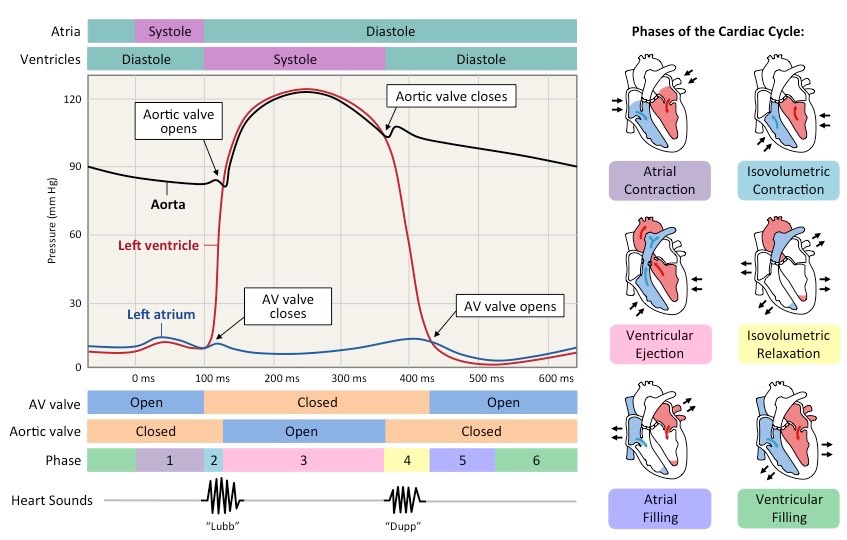
Cardiac Cycle: Atrial Systole
Chambers
Blood flows into atria + ventricle since pressure in them is lower.
When Ventricle ~70% full, atria CONTRACTS —> Force blood into ventricles.
Blood Flow
Blood flow from atrium to ventricle
Valves
AV Valve opens
Aortic valve closed
Cardiac Cycle: Ventricular Systole
Chambers:
Atria relaxes
Ventricle contracts
Blood Flow
Ventricle to aorta
Valves
As ventricles contract, ventricular pressure > atrial pressure = AV valves close to prevent back flow.
With both sets of heart valves closed, pressure rapidly builds in the contracting ventricles (isovolumetric contraction)
When ventricular pressure exceeds blood pressure>aorta → Aortic valve opens + blood is released into the aorta
Cardiac Cycle: Diastole
As blood exits the ventricle and travels down the aorta, ventricular pressure falls.
When ventricular pressure drops<aortic pressure → Aortic valve closes to prevent back flow.
When the ventricular pressure drops< atrial pressure—> AV valve opens and blood can flow from atria to ventricle
Throughout the cycle, aortic pressure remains quite high as muscle and elastic fibres in the artery wall maintain blood pressure.
Phases of Cardiac Cycle
Atrial contract —> Blood from atrium into ventricle
Isovolumetric Contraction builds pressure in the ventricle → Since AV valve is closed.
Ventricular Ejection occurs when ventricular pressure>aortic pressure —> Blood into aorta. Additionally, blood from RV can also go into pulmonary artery.
Isovolumetric relaxation
Atrial filling of blood
Ventricular filling.
Consequences of Coronary Occlusion
Blood clots
Potential for coronary heart disease.
If a coronary artery becomes completely blocked, an acute myocardial infarction (heart attack) will result.
Myocardial tissue requires the oxygen and nutrients transported via the coronary arteries in order to function = Coronary occlusion prevents it.
Physiological Respiration
Ventilation: The exchange of air between atmosphere and lungs —> Physical act of breathing.
Gas Exchange: The exchange of CO2 and O2 between alveoli + bloodstream (via passive diffusion).
Cell Respiration: Release of ATP from organic molecules.
Purpose of Ventilation
Concentration gradient in alveoli to allow gas exchange to occur (passive process):
O2 constantly removed from alveoli into bloodstream + CO2 released.
Lungs=ventilation system
O2 levels stay high in alveoli (and diffuse into the blood)
CO2 levels stay low (and diffuse from the blood)
Lungs have large surface area = increase the overall rate of gas exchange
Ventilation Changes (Physical Activity)
ATP production (via cellular respiration) produces carbon dioxide as a waste product (and may consume oxygen aerobically)=changes in blood CO2 levels
Changes in levels are detected by chemosensors in the walls of the arteries —> signals to the brainstem
As exercise intensity increases=increase demand for gas exchange= increase levels of ventilation.
Tidal Volume
Increasing the volume of air taken in and out per breath allows for more air in the lungs to be exchanged.
Ventilation Rate
Greater frequency of breaths allows for a more continuous exchange of gases.
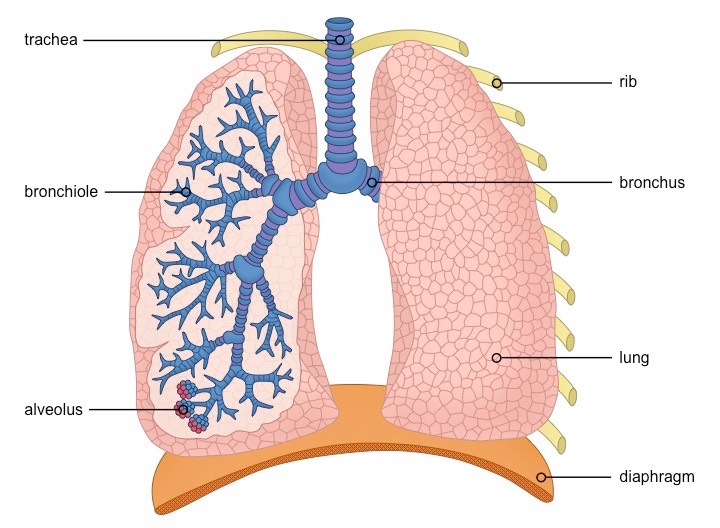
Respiration System
Air enters the respiratory system through the nose or mouth.
Passes through the pharynx —> trachea
Trachea —> until it divides into two bronchi which connect to the lungs
The right lung is composed of three lobes, while the left lung is only comprised of two (smaller due to position of heart)
Inside each lung, the bronchi divide into many smaller airways called bronchioles = Increase SA
Each bronchiole have alveoli, where gas exchange with the bloodstream occurs
Alveolus Structure (4)
Alveoli function as the site of gas exchange.
They have a very thin epithelial layer=minimise diffusion distances.
Rich capillary network=increase the capacity for gas exchange with the blood.
Roughly spherical=maximise the available SA for gas exchange
Internal surface covered in fluid = dissolved gases are better able to diffuse into the bloodstream
Pneumocytes
Cells that line the alveoli and comprise of the majority of the inner surface of the lungs.
Type I pneumocytes (4)
Type I pneumocytes are involved in the process of gas exchange between the alveoli and the capillaries
They are squamous: extremely thin (~ 0.15µm) —> minimising diffusion distance.
Connected by occluding junctions=prevents leakage of tissue fluid into the alveolar air space.
Type I pneumocytes are amitotic and unable to replicate.
Type II pneumocytes (3)
Type II pneumocytes=the secretion of pulmonary surfactant, which reduces surface tension in the alveoli
They are cuboidal + possess many granules (for storing surfactant components)
Type II pneumocytes only comprise a fraction of the alveolar surface (~5%) but are relatively numerous.
Pulmonary Surfactant
While moist lining of alveoli = helps gas exchange, it also increases tendency to collapse —> Surface tension (elastic force): created by cohesion of liquid molecules.
Pulmonary surfactant decreases surface tension.
As alveoli expands (gas intake) = surfactant spreads = decrease surface tension + increase rate of expansion (in smaller alveolus) to ensure same rate of inflation.
Breathing
Change of pressure within lungs by changing volume of thoracic cavity.
Pressure is inversely proportional to volume.
Mechanisms of Breathing: Volume increased
Lung pressure drops below atmospheric pressure.
Air move into lungs to equalize pressure —> Inspiration.
Diaphragm contracts —> Expand lungs = increase chest volume.
Mechanisms of Breathing: Volume decreases
Lung pressure rises above atmospheric pressures.
Air move out of lungs → Expiration
Diaphragm relaxes → Presses on lungs (smaller) = decrease chest volume.
Inhalation
Diaphragm contract = increase thoracic cavity volume
External intercostals (muslce between ribs) contract = ribs expand up and forward.
Additional muscle groups: sternocleidomastoid, pectoralis minor.
Exhalation
Diaphragm relax = curves up = decreases volume of thoracic cavity.
Internal intercostal muscles contract = ribs down and in.
Abdominal muscles contract= forced exhalation.
Elastic recoil of lungs = forces air OUT of lungs during expiration.
Additional muscles pull ribs down = quadratas lumborum.
Lung Disorder: Emphysema
Walls of alveoli loses elasticity due to damage.
Leads to abnormal enlargement of alveoli and decreased SA for gas exchange.
Degradation of walls = holes = alveoli merge into pulmonary bullae.
Consequences: increased susceptibility of chest infections, cyanosis, shortness of breath, etc.
How smoking causes emphysema
Chemical irritants in cigarettes = damage alveolar walls.
Damage to lung tissue = recruit phagocytes that produces elastase.
Elastase breaks down elastic fibres in alveolar wall.
Lung Cancer
Uncontrolled proliferation of lung cells.
The lungs are vital to normal body function and thus the abrogation of their normal function is particularly detrimental to health
The lungs possess a very rich blood supply, increasing the likelihood of the cancer spreading (metastasis) to other body regions
Spirometry
Spirometry involves measuring the amount (volume) and / or speed (flow) at which air can be inhaled or exhaled —> Detects changes in ventilation.
Neurons
Specialized cells that transmit electrical impulses within the nervous system → Detect + respond to stimuli.
Sensory neurons: transmit information from sensory receptors to CNS
Relay neurons: Transmit info within CNS as part of decision-making process.
Motor neurons: Transmit info from CNS to effectors → Initiate response
Neuron Structure (Motor Neuron)
Dendrites: Short-branched fibres that convert chemical information into electrical signals.
Axons: Elongated fibre that transmits electrical signals to terminal regions for communication.
Soma: Cell body containing nucleus + organelles → Essential metabolic processes.
Axon terminals at the end of axons → Where synaptic transfer occurs.
Some neurons may have myelin sheath (phospholipids + proteins) = Improve conduction speed of electrical impulses along axon (action potential jumps between nodes of Ranvier).
Myelin
Produced by glial cells → Schwann cells in peripheral nervous system and oligodendrocytes in central nervous system.
Increase speed of electrical transmissions via saltatory conduction → Action potentials “hop” between nodes.
Takes up space.
Resting Potential
Difference in charge across membrane when neuron is not firing. → Inside of neuron is MORE NEGATIVE relative to outside (~-70 mV.)
Maintained by sodium-potassium pump (active process):
Na+ and K+ pump is transmembrane protein that exchanges these ions (antiport).
Expels 3 Na+ for every 2 K+ ions admitted. → Creates electrochemical gradient where cell interior is relatively negative compared to extracellular environment.
Requires hydrolysis of ATP.
Action Potential Definition
Rapid changes in charge across membrane that occurs when a neuron IS firing.
Action Potential: Depolarization
Sudden change in membrane potential from relatively negative to positive internal charge.
Sodium channels open within membrane of axon. Since Na+ ions are concentrated outside = opening of channels = passive INFLUX of sodium.
Influx = Positive membrane potential (+30 mV).
Action Potential: Repolarization
Restoration of membrane potential following depolarization.
Potassium channels open within membrane of axon.
K+ ions are more concentrated inside neuron = Passive EFFLUX of K+
Efflux = membrane potential becomes more negative (~-80 mV).
Refractory Period
The period of time following nerve impulse before neuron can fire again. Need to restore concentration gradient (since ionic distribution is largely reversed).
Requires antiport action of sodium-potassium pump to ensure that more Na+ is outside, and K+ is inside neuron.
Inside ~-70 mV again
Nerve Impulses
Action potentials that move along the length of axon as wave of depolarization.
+ Depolarization occurs when change in internal membrane charge reaches ~-55 mV
+ Ion channels that occupy length of axon are VOLTAGE-GATED → So depolarization at one point = opening of ion channels at next segmenet = unidirectional wave along axon length.
Oscilloscope Traces
Oscilloscopes are instruments that measure membrane potential across a neuronal membrane. Data displayed in time (milliseconds) on X axis and membrane potential (mV) in Y axis.
Resting potential ~-70 mV
Depolarization: +30 mV
Repolarization: -80 mV
Refractory: Returns to level of resting potential
Synaptic Transfer
Chemical transfer across synapses.
When action potential reaches the axon terminal of presynaptic neuron, it triggers the opening of voltage-gated calcium channels.
Ca2+ diffuse into the cell → Bind to vesicles containing neurotransmitters → Causes exocytosis.
Neurotransmitters are released into synaptic cleft.
Neurotransmitters bind to receptors on post-synaptic membrane (connected to ligand-gated ion channels).
Causes channels to open = generates electrical impulse in post-synaptic neuron.
Neurotransmitters can be recycled (reuptake pumps) or degraded (enzymes in cleft).
Neurotransmitters
Chemical messengers released from neurons to transfer signals across the synaptic clef.
Can be excitatory (Excitatory post-synaptic potentials [EPSPs]) or inhibitory (IPSPs) to a response.
Response to different cell types -
Neuron: Stimulation/inhibition of electrical signal.
Glandular cell: Stimulation/inhibition of secretion (exocrine/endocrine)
Muscular Fibre: Stimulation/inhibition of muscular contraction/relaxation
Exocrine System
Includes glands that secrete substances into a ductal system to an epithelial surface
Endocrine System
Secrete products (i.e. hormones) directly into bloodstream.
Acetylcholine
Commonly released at neuromuscular junctions and binds to receptors on muscle fibres to trigger muscular contractions.
Released in autonomic nervous system to promote parasympathetic responses (i.e. rest + digest)
Activates a post-synaptic cell by binding to either classes of specific receptor → Nicotinic or muscarinic.
Need to be continually removed from synapse since overstimulation = fatal convulsions and paralysis.
Acetylcholinesterase (AChE)
Synaptic enzyme that breaks down acetylcholine into acetyl group + choline.
AChE either released into synapse from presynaptic neuron or is embedded on membrane of post-synaptic cell.
After, liberated choline returns to presynaptic neuron to be coupled with another acetate → Reform acetylcholine.
Neonicotinoid Pesticides
Irreversibly bind to nicotinic acetylcholine receptors in pests.
Trigger a sustained response = causes insects to die since they have receptors that bind to neonicotinoids more strongly.
Neonicotinoid pesticides CANNOT be broken down by acetylcholinesterate.
Graded Potential
Opening of channels on post-synaptic membrane= small changes in membrane potential (graded potential).
A nerve impulse is only initiated if a threshold potential is reached.
Excitatory neurotransmitters (e.g. noradrenaline) cause depolarisation by opening ligand-gated sodium or calcium channels
Inhibitory neurotransmitters (e.g. GABA) cause hyperpolarisation by opening ligand-gated potassium or chlorine channels
If depolarization > hyperpolarization + threshold is reached = neuron fire (vice versa.)
Central Nervous System
Made up of brain + spinal cord
Contains relay neurons
Peripheral Nervous System
Made of peripheral nerves that link CNS to body’s receptors + effectors
Contains sensory neurons + motor neurons.
Stimulus-Response Model
Receptors transform stimuli into electrical nerve impulses transmitted via neurons to CNS → Where decision-making occurs.
When a response is selected, the signal from neurons is transmitted to effectors (organs that produce a response to stimulus).
Response = resulting change in organism
Reflex Actions
Reflex: Rapid and involuntary response to stimulus that triggers reflex arc.
Sensory information directly relayed to motor neurons within the spine = faster response without conscious thought.
Insulin
Antagonistic hormone released from pancreas and acts (mostly) on liver.
When blood glucose level is high = insulin from Beta cells of pancreas = reduce bg concentration.
Stimulating glycogenesis in liver = increase glucose uptake by liver/adipose tissue.
Glucagon
Antagonistic hormone released from pancreas and acts (mostly) on liver.
When blood glucose level low = glucagon from alpha cells of pancreas = increase level.
May involve glycogen breakdown in liver (Glycogenolysis) + increased glucose release by liver/adipose tissue.
Diabetes mellitus
Metabolic disorder that results from prolonged high blood glucose.
Type I: Beta cells do not produce insulin = glucose not removed from bloodstream = treated by insulin shots.
Type II: Desensitization (down-regulation) of insulin receptors = glucose not removed = treated by lifestyle changes.
Causes: genetic disposition, diet (excess in fat, cholesterol, etc.)
Thyroxin
Secreted by the thyroid gland = signals derived from hypothalamus = acts on nearly every tissue.
Partially composed of iodine (iodine deficiency = decreased thyroxin production).
Iodine deficiency = goiter.
Role: Increase basal metabolic rate by stimulating carbohydrate/lipid metabolism (oxidation).
Results in increased heat = thyroxine controls body temperature.