RESUS, TRAUMA, CRISIS in KIDS
1/40
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
41 Terms
Indicators of a critically ill infant
Describe the aetiology of arrest in paeds pts
Resp pathology
most cardioresp arrests in children are secondary to hypoxia due to respiratory pathology (e.g. birth asphyxia, bronchiolitis, asthma, inhalation of foreign body)
Thus in ALS/BLS, oxtgen delivery rather than defibrillation is the critical first step
In the context of anaesthesia, hypoxia due to laryngospasm may lead to bradycardia then asystole
Neurological dysfunction may also lead to resp arrest
(e.g. convulsion, poisoning)
Circulatory failure
small proportion of cardiac arrests
Fluid loss or blood loss
gastroenteritis, burns, truma
Maldistribution of fluid
sepsis, anaphylaxis
Primary cardiac cause
UNCOMMON in kids
Discuss the assessment of blood loss in kids
Weight lost
Clinical signs
Labs
Clinical
Pulse
Brachial < 1yr
Carotid or femoral > 1 yr
CRT
sens but not specific
Skin colour/temp
Mottling indicates porr perfusion
BP
VERY LATE SIGN
UO decreased
Drowsy
How are children different in the assessment of this
Vital signs vary with age
Blood vol is larger 80-90 ml/kg
Bloood vol is smaller in ABSOLUTE TERMS
Children compensate for LARGE IV losses before beocming hypotensive
UO is rel greater 1-2 ml/kg/hr
Describe fluid resus in kids with blood loss
How to give
What vol of PRBC to kids who are not actively bleeding
3 way tap in order to rapidly syringe in fluid boluses
20 ml/kg bolus
REASSESS
20 ml/kg bolus
REASSESS
PRBC
In children who are anaemic but not actively bleeding, volume of PRBC is:
o 10ml/kg of PRBC increases Hb by 3g/dL
o 4ml/kg of PRBC increases Hb by 1g/dL
Assessment and Mx of dehydration
Three types of fluids for kids
How to assess
Severity
RESUS - 10-20 ml/kg
MAINTENANCE - 4, 2, 1 (if unwell 2/3 of maintenance because kids secrete more ADH)
REPLACEMENT - Before used a clinician estimate but this is inaccurate. See RCH guideline. A constant fluid rate based on premorbid weight then just adjust the duration. Replace over 24h (if < 5%) but if larger deficit and sicker child then replace over 48h
eg. Vol in ml needed for replacement =
% deficit x BW x 10
5 × 10 × 10 = 500 ml
Use IBW
Weight lost
Clinical signs
Labs
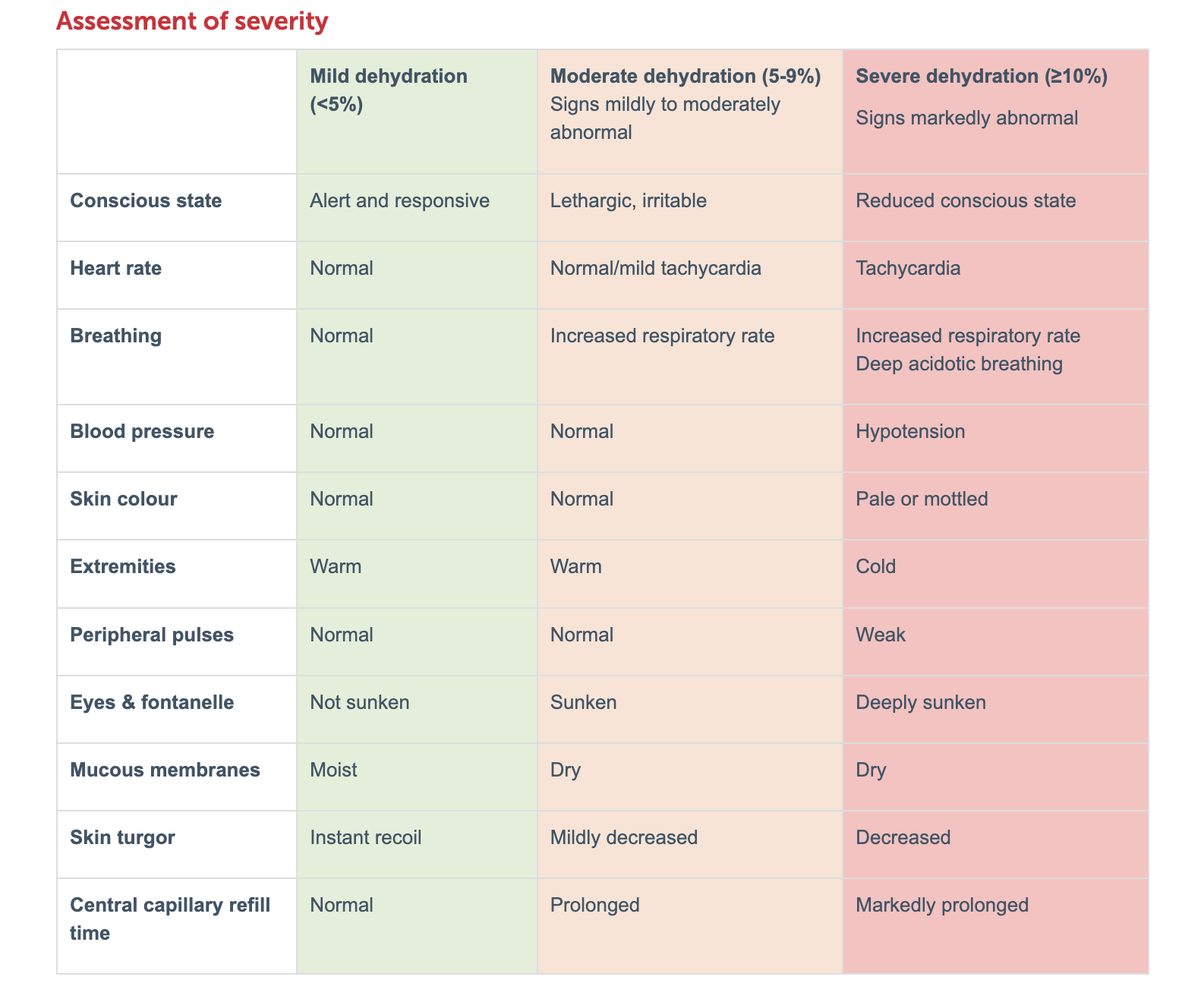
Degree of dehydration expressed as % of bw
3 MILD
6 MOD
9 SEVERE
How to gain access in shocked paeds pt
What are the options
IO where
How to confirm IO
What bloods
It is extremely difficult
IO
EXT JUG
FEMORAL VEIN using seldinger
Cutdown to long saphenous
Sagittal sinus cannulation in babies
Anteromedial surface of tibia
2-3 cm below tibial tuberosity
ie. away from growth plate
Aspiration of blood or BM
Free flow of fluid by gravity
Blood culture
Blood group
Biochem
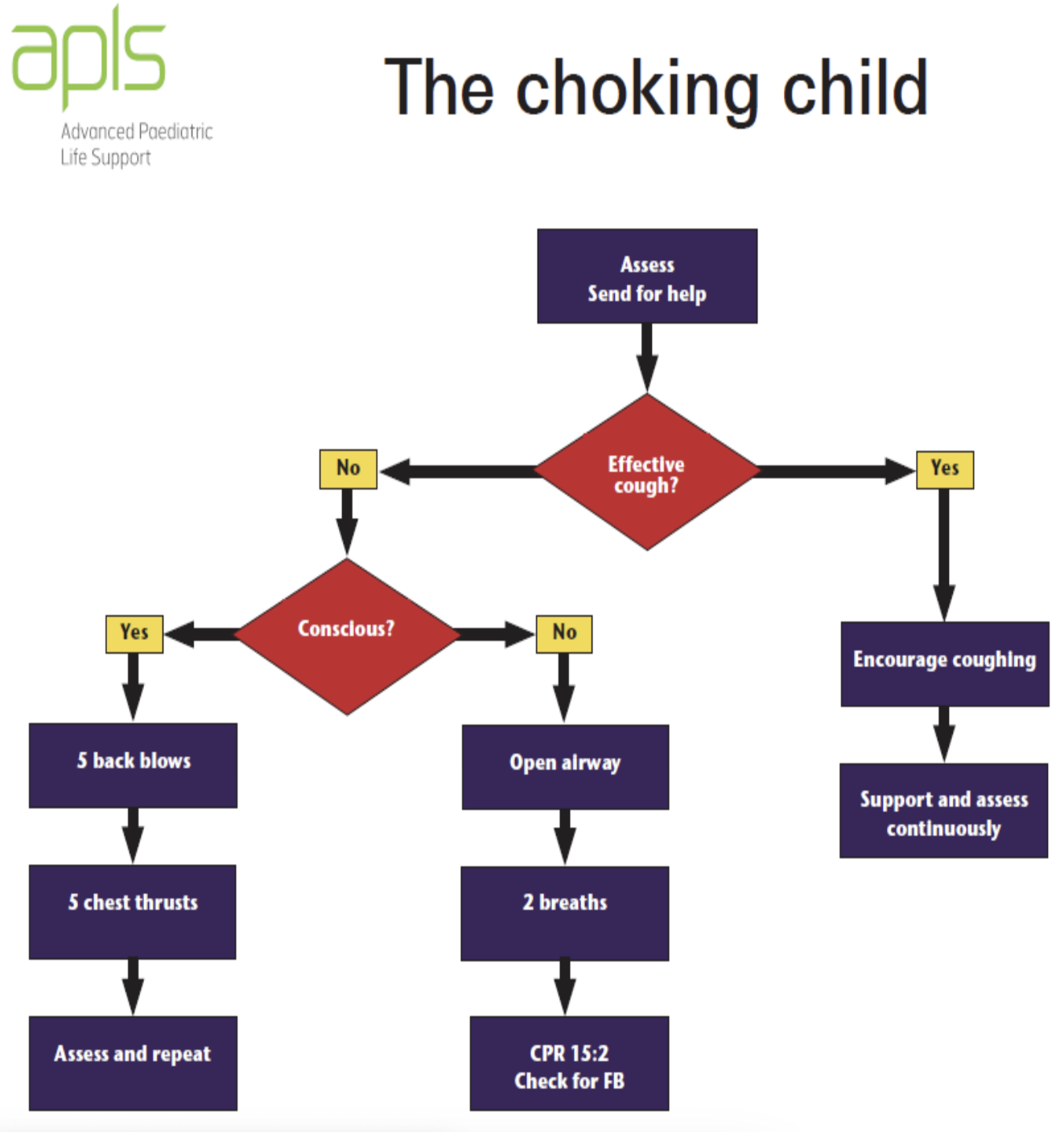
Mx of choking child
Paed ALS
bpm
30:2
15:2
Drug doses
Joules
Post resus
Compress 100-120 bpm
single person 30
2 people 15
Adrenaline 10 mcg/kg
Amiodarone 5 mg/kg
4 JOULES/kg
Post resus
A-E
Optimise oxygen delivery
offload ventricle
maximise cerebral perfusion pressure
ECG, bloods, CXR, BSL
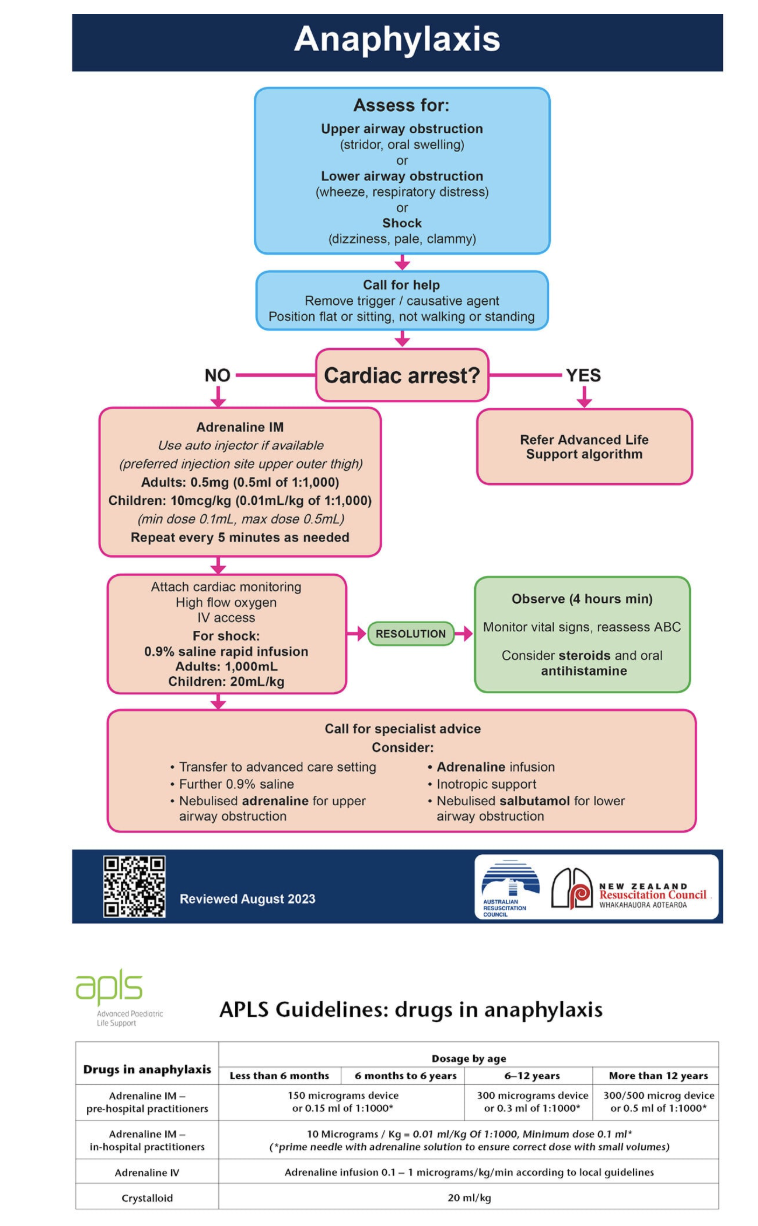
Anaphylaxis
Common causes
NMB
Latex
Abx
Contrast
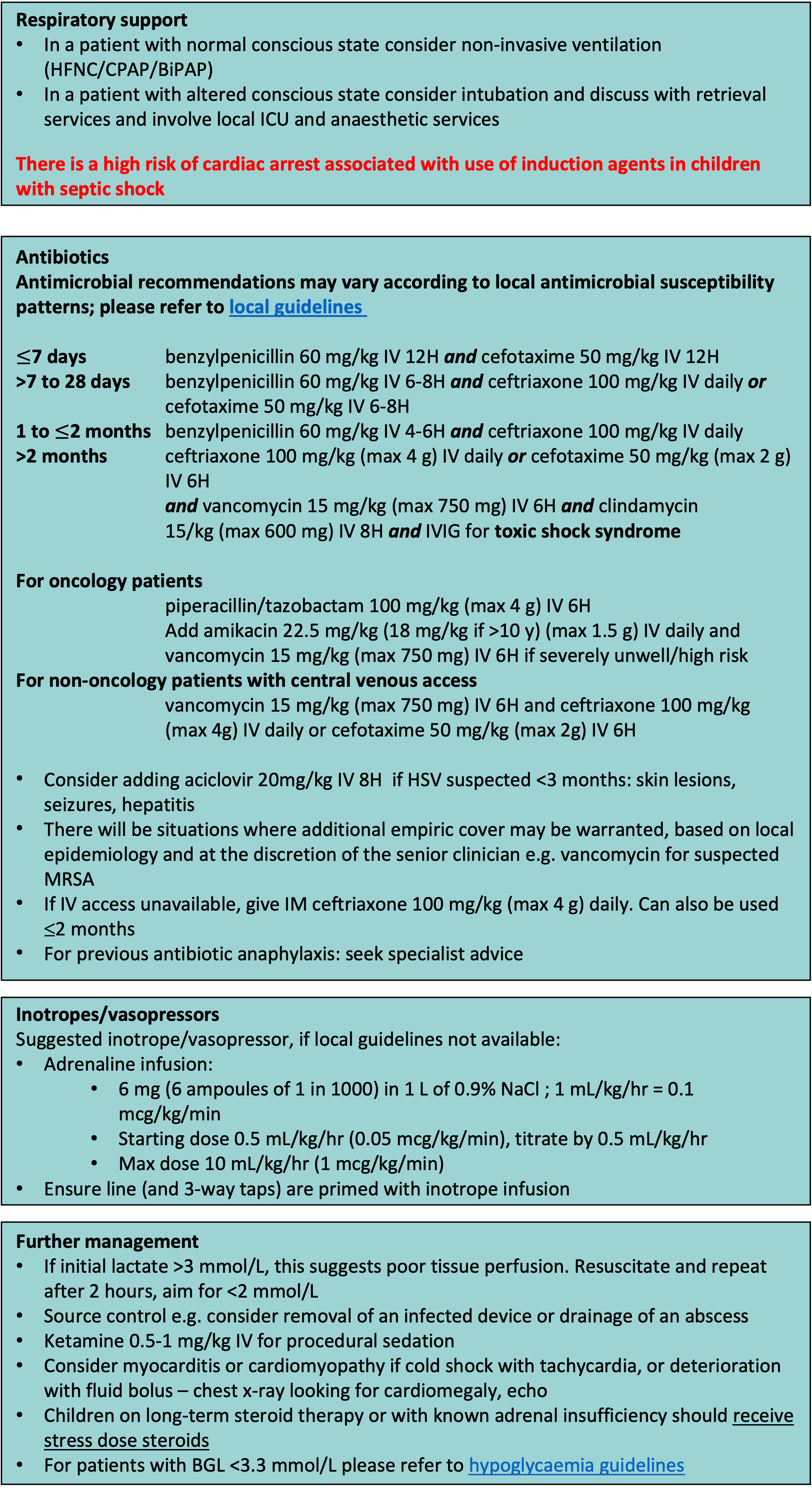
Sepsis
Major pathogens < 2 months old
Major pathogens in older kids
What % present cold shock
What % present warm shock
Every hr they remain in shock their mort
Key features of sepsis on assessment
2/3 children present in ‘cold’ shock (normal/low CO and high SVR)
1/3 children (and adults) present in ‘warm shock (normal/high CO and low SVR)
DOUBLES
RCH sepsis flowchart
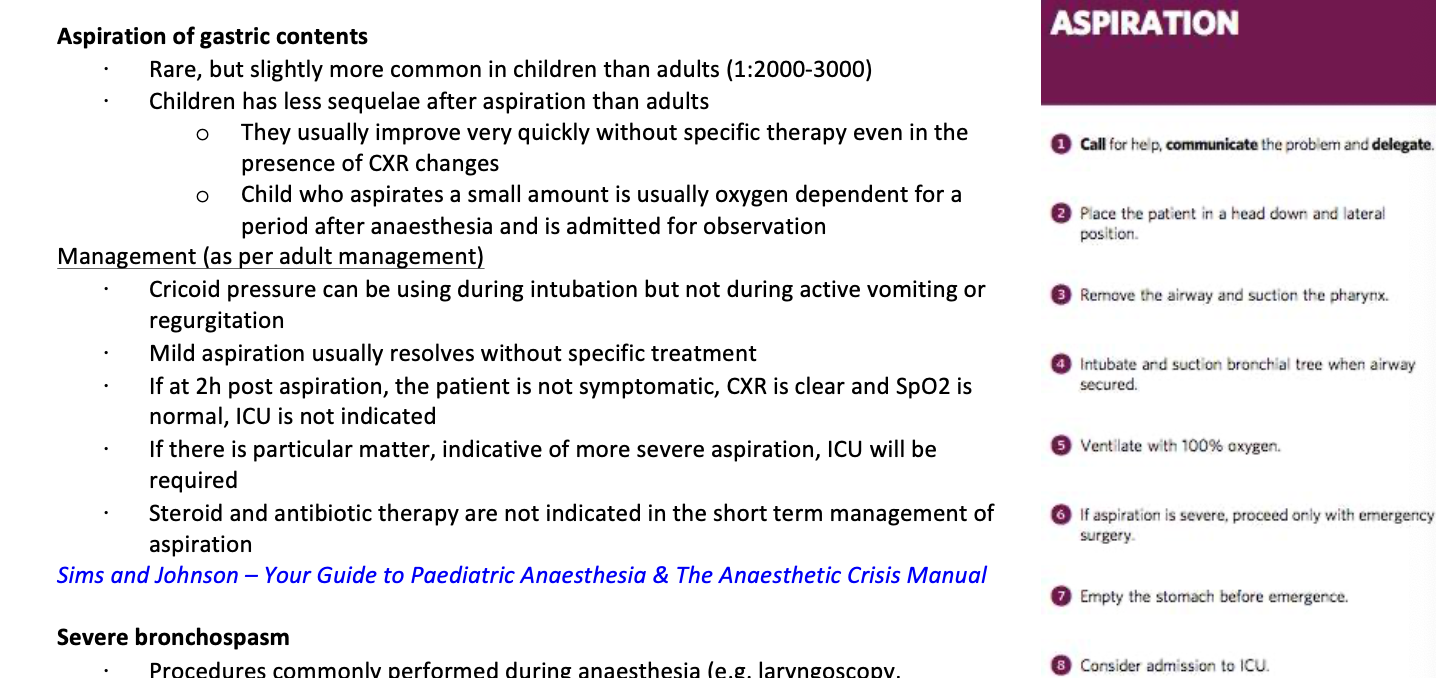
Aspiration
Severe bronchospasm
what can trigger
stable asthma pts?
What about wheeze preop?
Mx
Procedures commonly performed during anaesthesia (e.g. laryngoscopy, intubation, suctioning) are intense and potent stimuli that can trigger bronchospasm
In stable asthmatic patients, peri-op risk for bronchospasm is low and is not assoc with significant increase in morbidity
In the child with wheeze at time of pre-op assessment, there is a very high risk for intra-op bronchospasm
Severe bronchospasms requires more aggressive, IV bronchodilator therapy
Mx is as per adult but more frightening
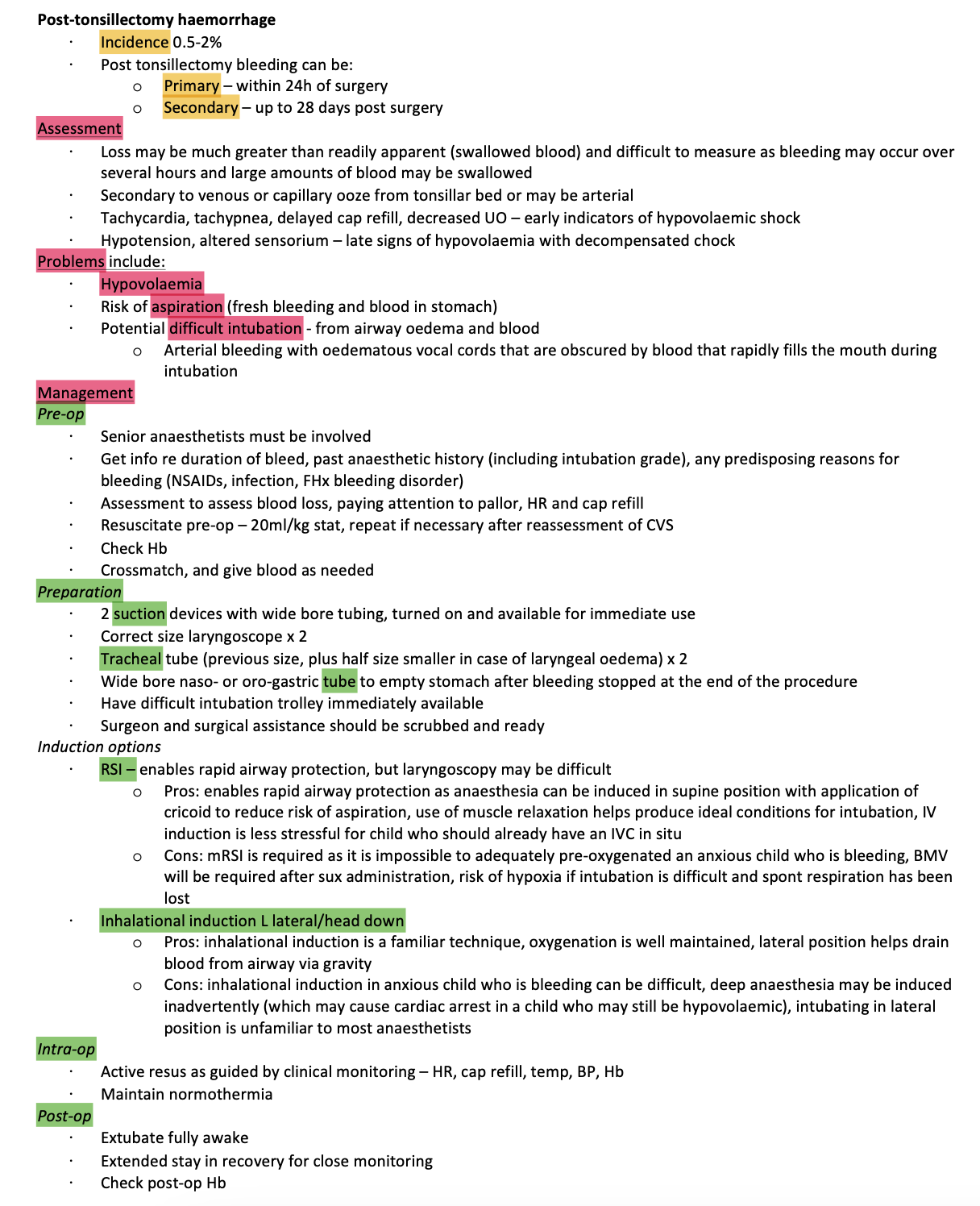
POST Tonsillectomy bleed
Incidence
Primary
Secondary
Factors that affect bleed rates
Assessment
KEY PROBLEMS
MANAGEMENT
Incidence
3.5% get bleed
0.9% RTT
FACTORS THAT AFFECT BLEED
Age (lower rates in kids)
Highest with quinsy and recurrent tonsillitis
Surg technique - highest with diathermy, lowest with blunt technique
KEY PROBLEMS - PPASHA
Hypovolaemia
Potential coagulopathy
Aspiration risk
Difficult and Soiled airway
Shared airway
Paediatric patient
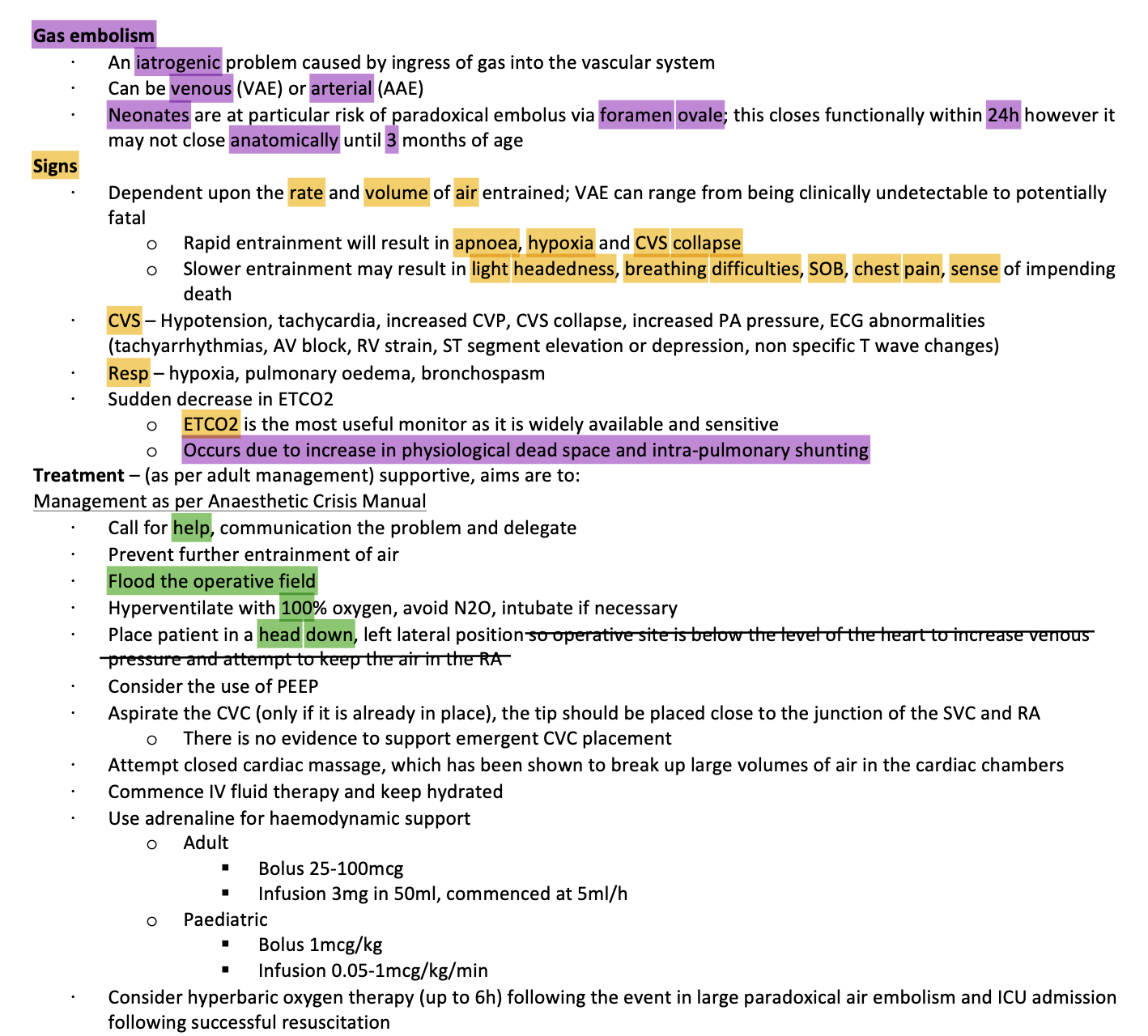
Gas Embolus
Why head down left laft with venous gas embolus
A head-down (Trendelenburg) position helps manage a venous gas embolism by using gravity to trap air bubbles away from the pulmonary artery outflow tract. This relieves the "air lock" in the heart so blood can keep pumping. Combined with a left lateral decubitus tilt, it prevents air from traveling to the brain or lungs
Venous Gas Embolism: Head-down and left-side positioning are recommended. This traps air in the apex of the right ventricle, keeping the outflow tract clear
Arterial Gas Embolism: The head-down position should be avoided. It increases intracranial pressure and can worsen cerebral edema. Patients with arterial bubbles should remain flat (supine)
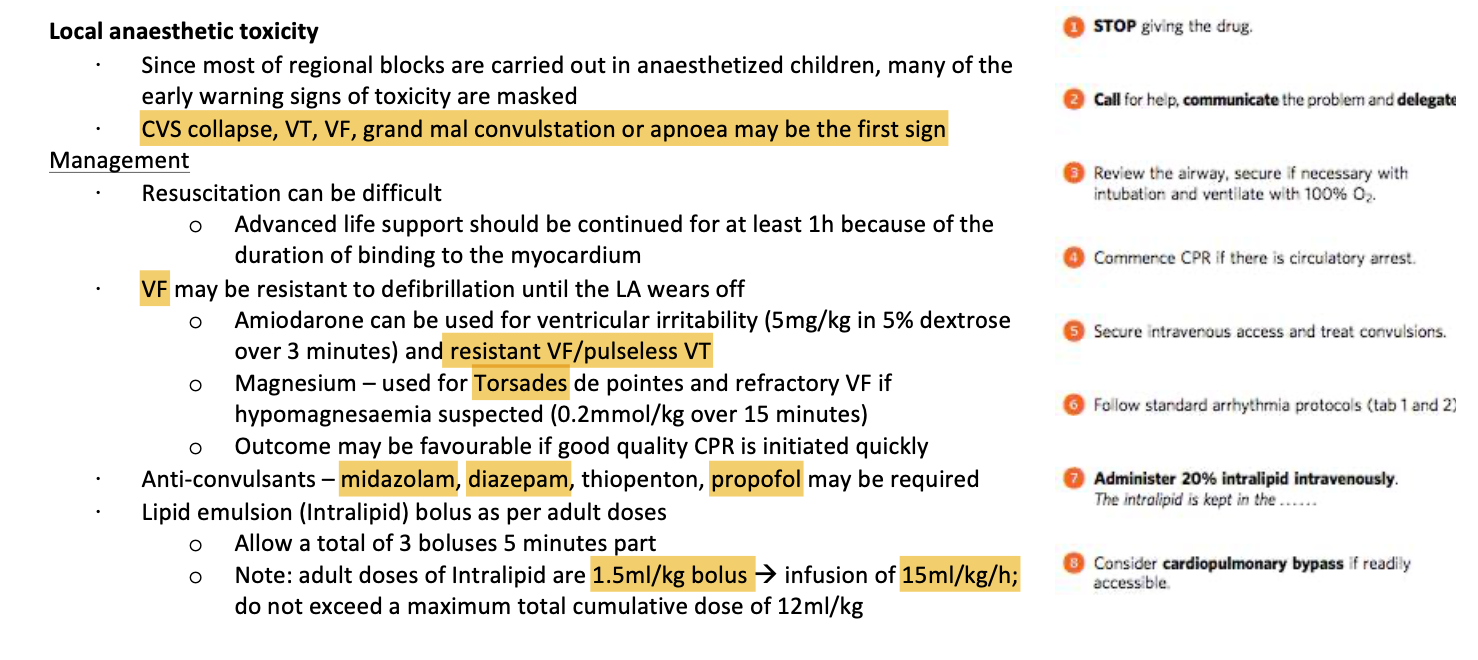
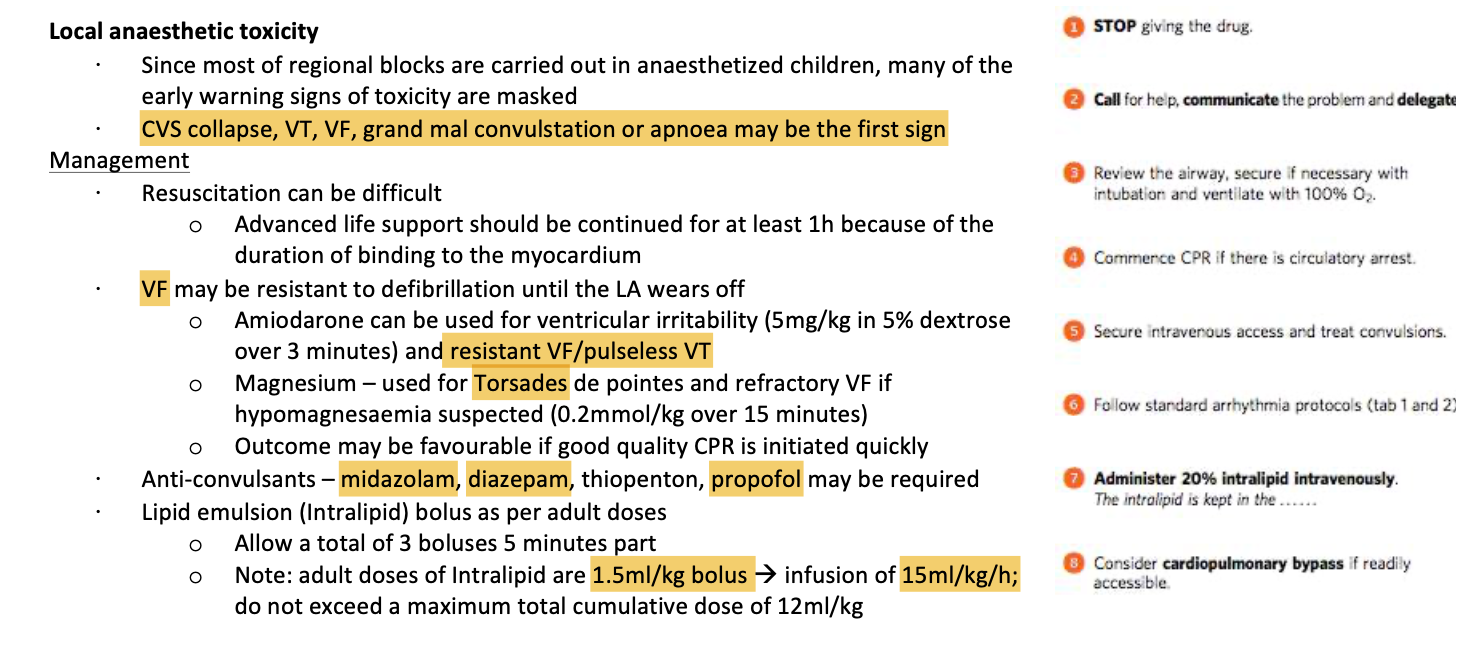
LAST
Malignant hyperthermia
Muscle diseases assoc with MH
v rare in 1st year of life
King denborough
myotonia fluctuans
PYLORIC STENOSIS
What will kill them on induction?
BG
What is it
Med or surgical emerg?
Three stages?
Incidence?
% male or female
Peak pres?
PATHOPHYSIOL
three aspects
=== DEHYDRATION KILLS ON INDUCTION NOT ELECTROLYTE IMBALANCE
BG
Hypertrophy of outlet of stomach
MEDICAL EMERGENCY
Three stages
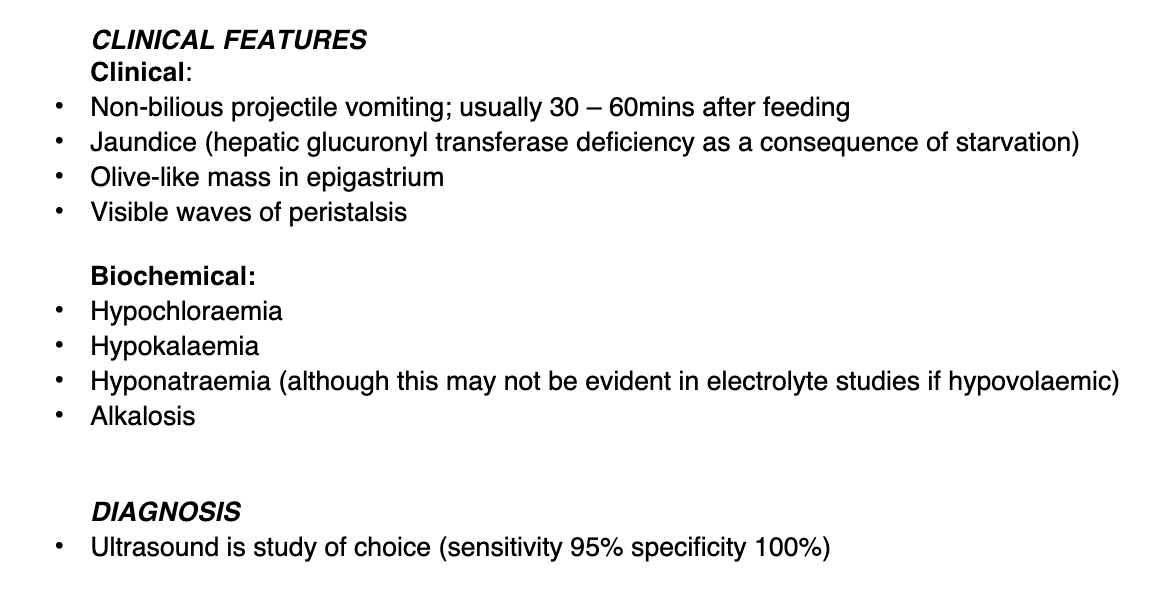
Hypochloraemic, hypoNa, MET ALK, DEHYDRATION, Alk urine
K depletion, paradoxical ACIDIC urine
SHOCK, Lactic acidosis, starvation ketosis
1 in 350
80% male
PEAK 2-5 weeks of age
PATHOPHYSIOL
Vomiting causes loss of HCl, water, small amount Na and K
Pancreatic bicarb is produced not secreted
→ Metabolic ALK
So much bicarb then overwhelms the resorptive capacity of PCT → alkaline urine
ECF vol depletion stims the RAAS
Na is retained and (K is lost and H+ is lost)
URINE becomes acidic
Total body K+ drops
Lose K in vomit but also shift from ECF to ICF due to alkalosis
(H+ moves out and K+ moves in)
Problem is - there is insufficient Cl in the glom filtrate
Cannot exchange with bicarb
Kidney cannot correct the acidosis (cant retain bicarb)
—→ ACIDIC URINE
—→ METABOLIC ALK
—→ IN EXTREME UNCORRECTED CASES THEN SHOCK, REDUCED TISSUE PERFUSION → METABOLIC ACIDOSIS
—> COMP RESP ALKALOSIS (Hyperventilation)
Clinical features
Diagnosis
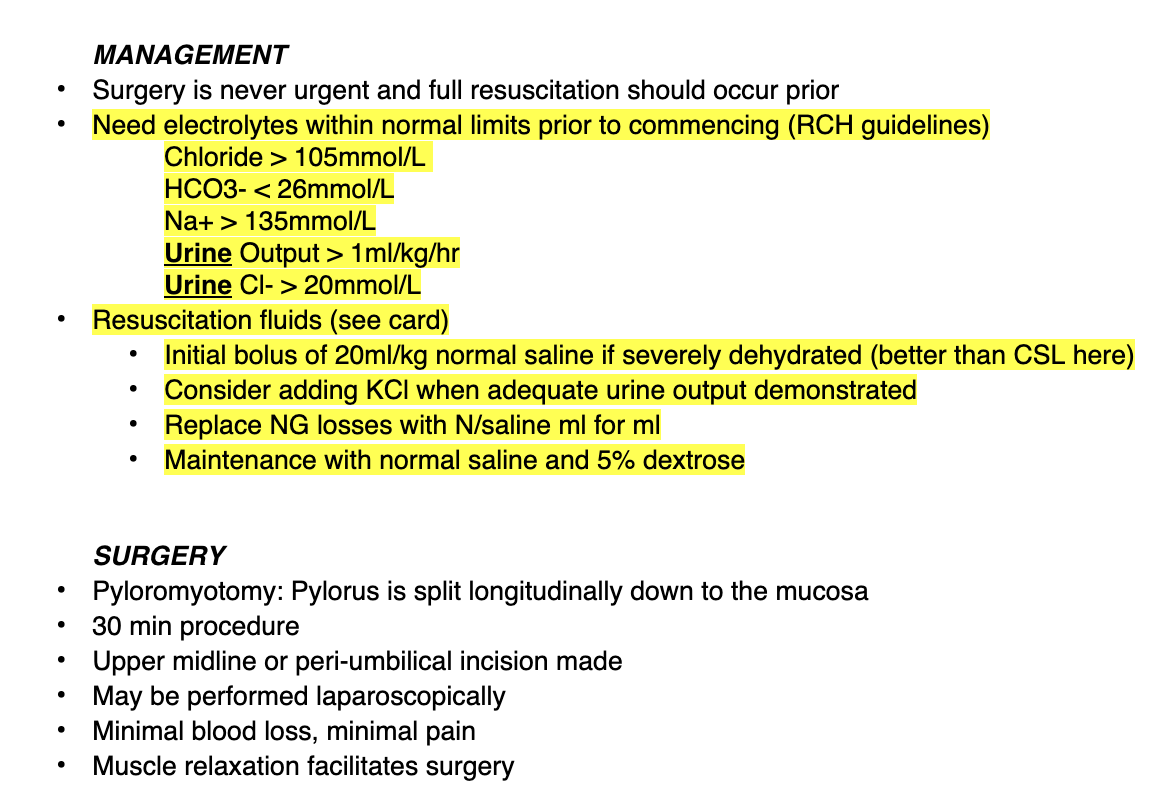
Mx
Is surgery urgent
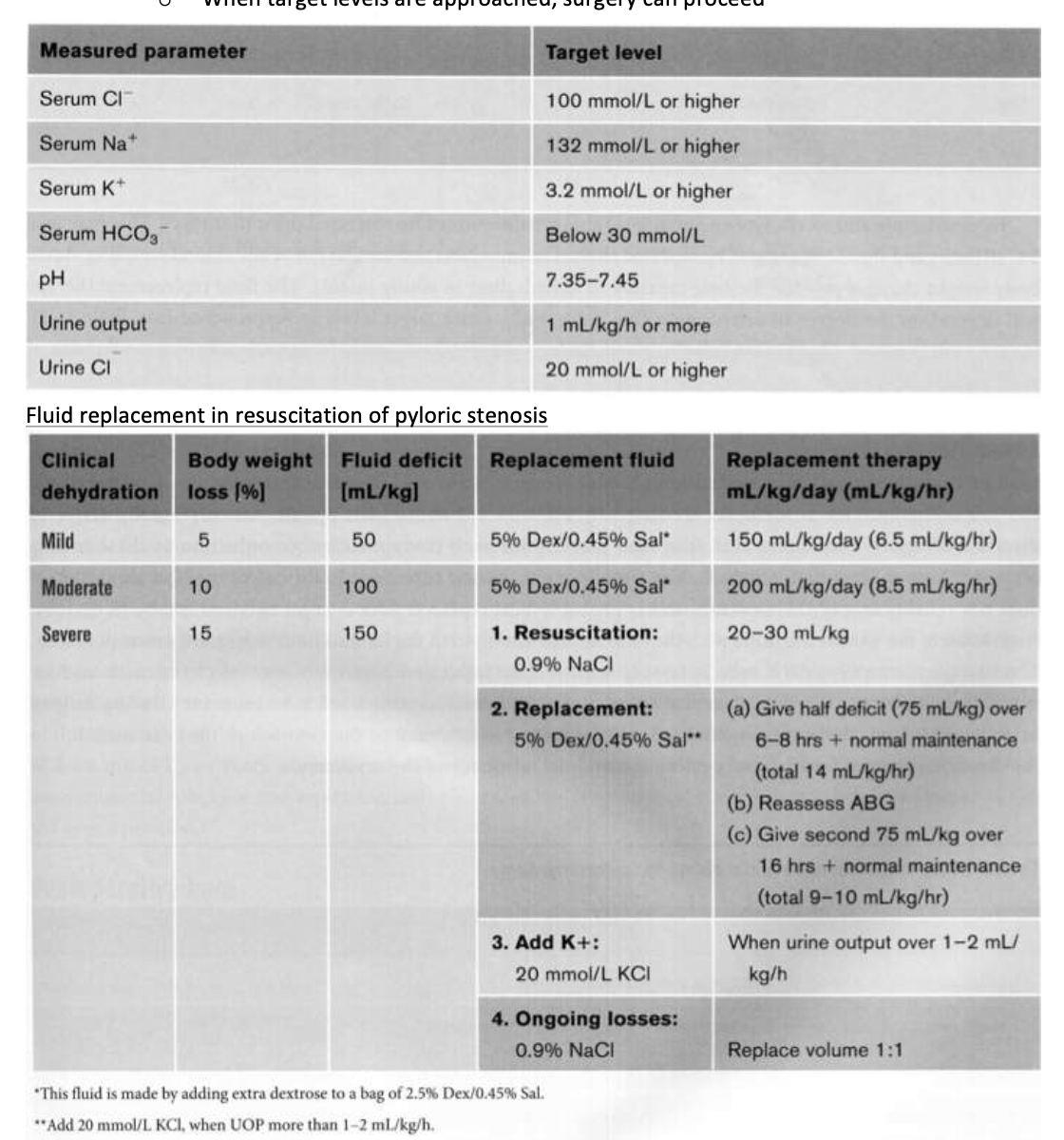
What must happen prior?
Briefly what do the surgeons do
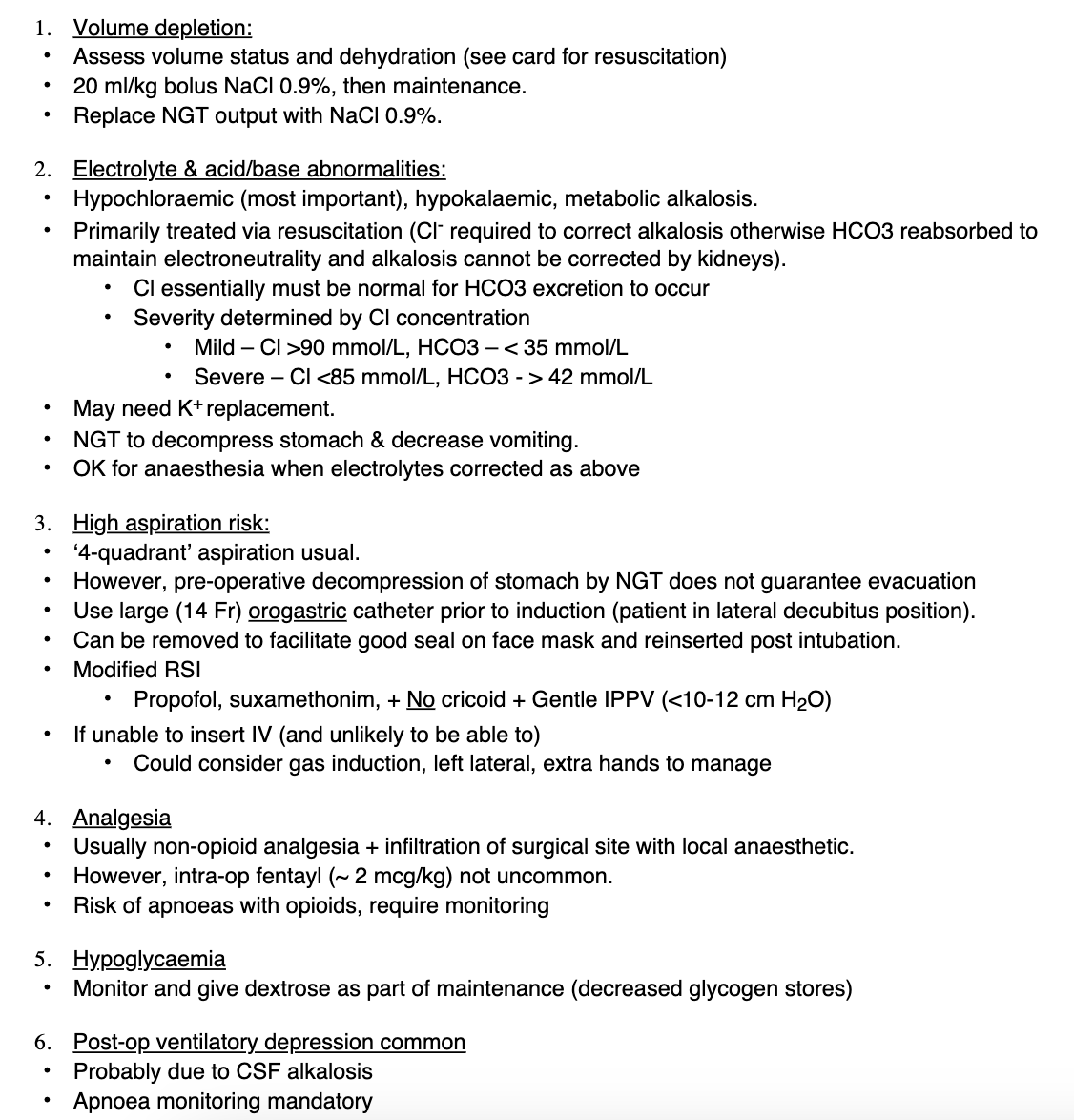
Anaesthetic Implications
PREP
Vol depletion
Electrolyte abnormalities
Pre-op wide bore NGT decompression
INDUCTION - controversial
Many paeds anaes use sevo and atrac - avoiding sux brady
OR propofol and sux
Very few know how to do cricoid in neonate
MAINTENANCE
Non-opioid or small amount of fentanyl
Risk of apnoeas
Hypoglycaemia
EMERGENCE
Extubate light
DISPOSITION
Post-op ventilatory depression common
How is severity assessed?

Fluid resus and replacement in PS
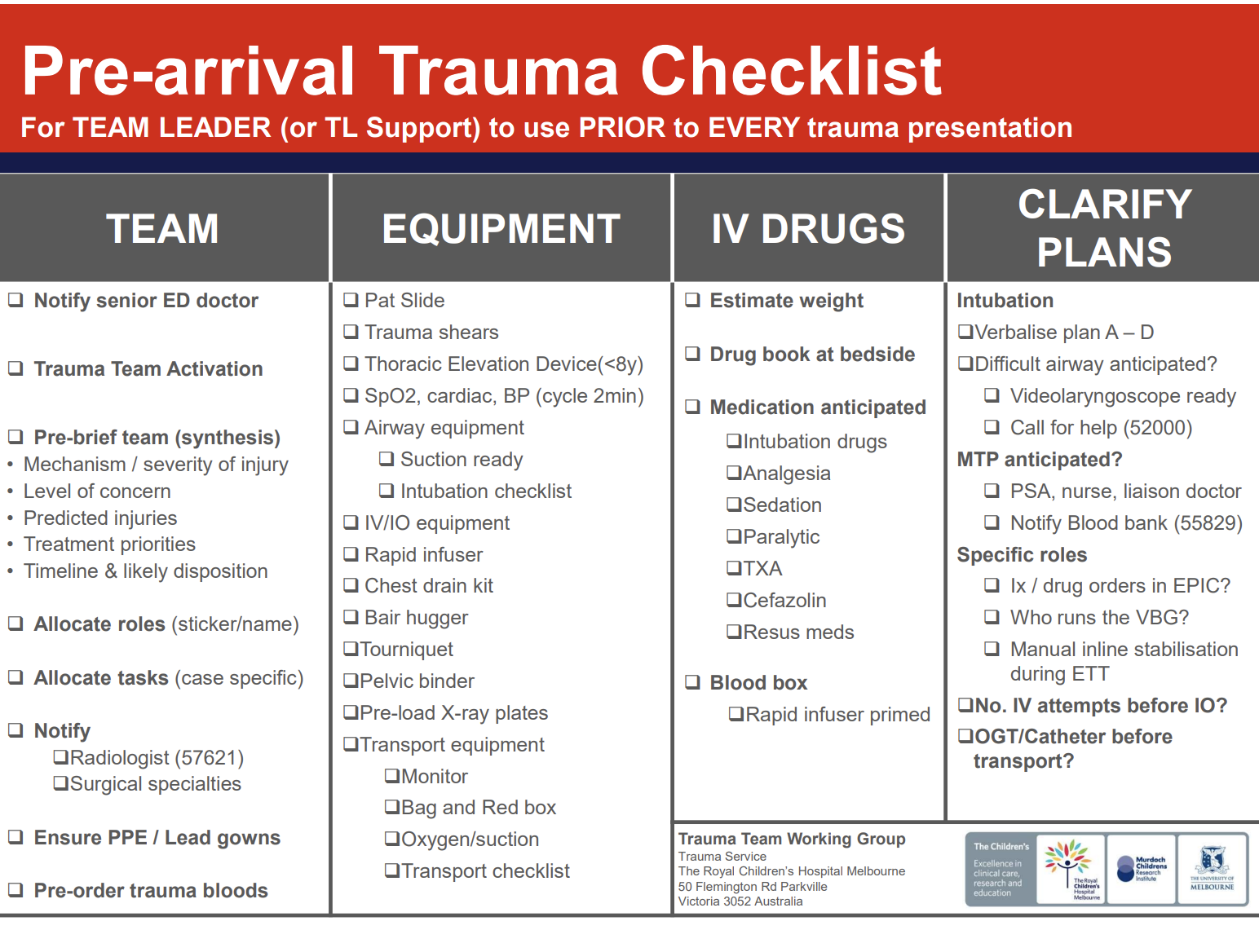
Outline special preparations in the emergency department prior to the arrival of a paediatric trauma patient
TEAM
EQUIPMENT
IV DRUGS
PATIENT
PAEDS TRAUMA PT ARRIVED
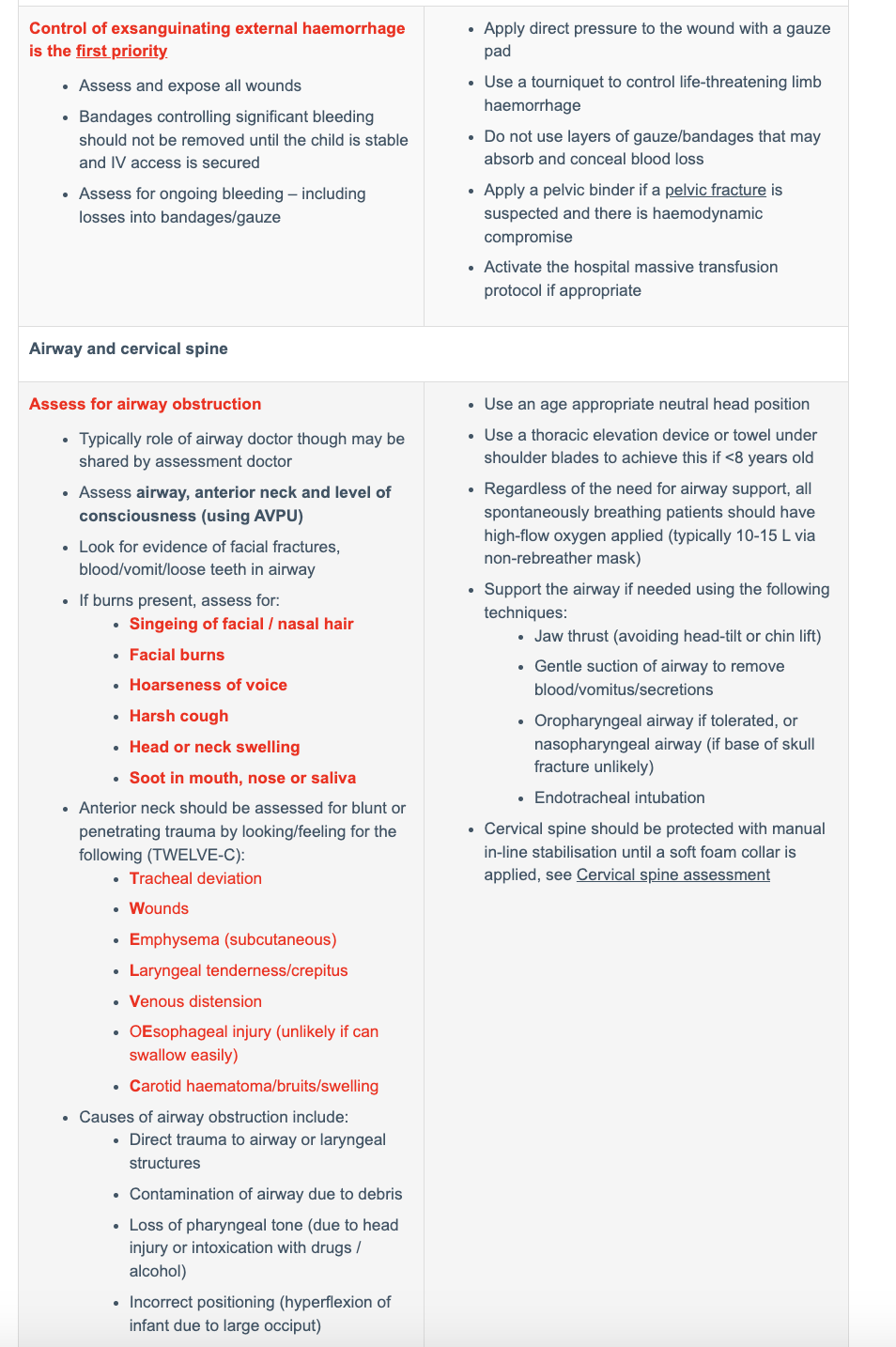
Control of exsanguinating external haemorrhage
AIRWAY AND CSPINE
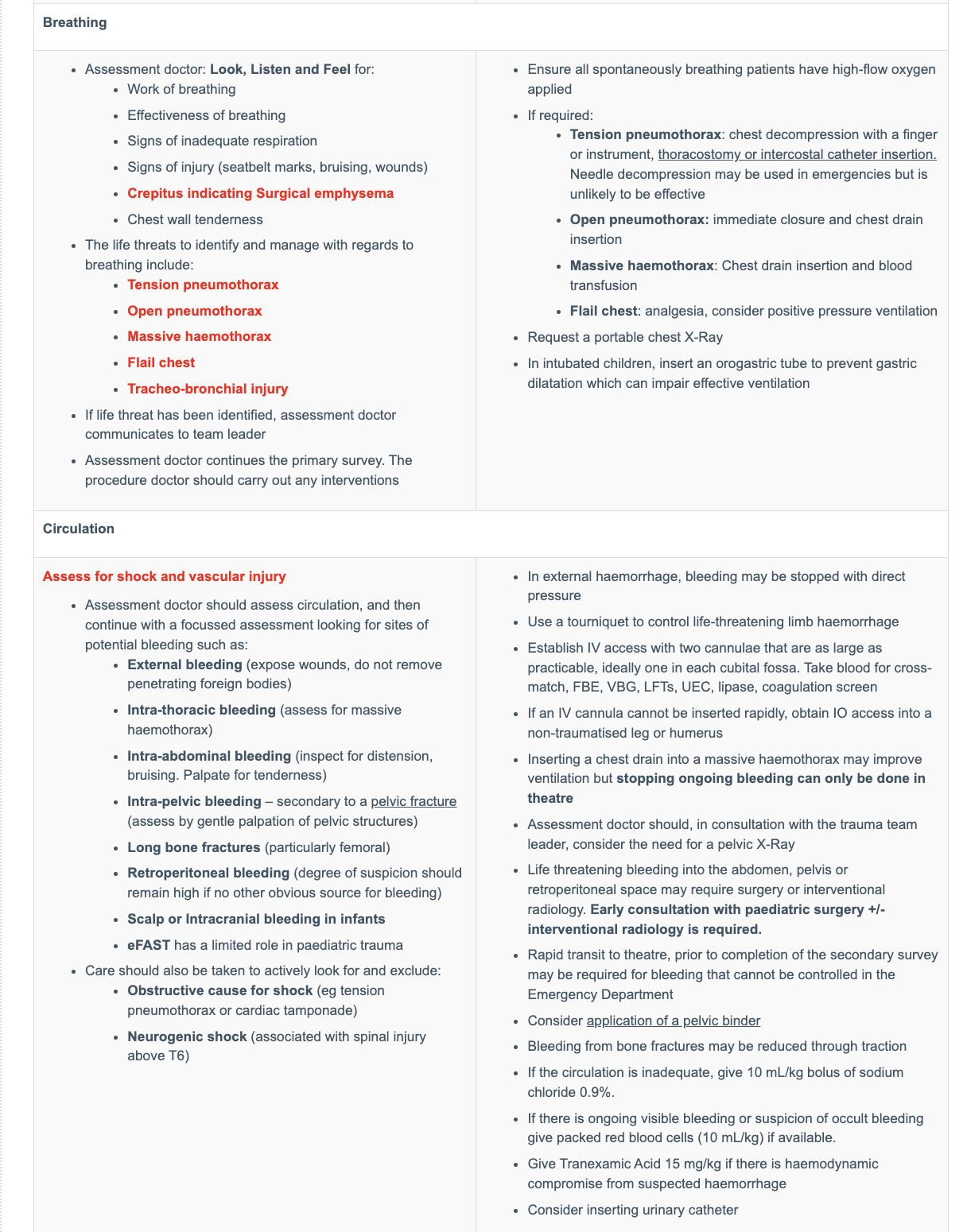
BREATHING
CIRCULATION
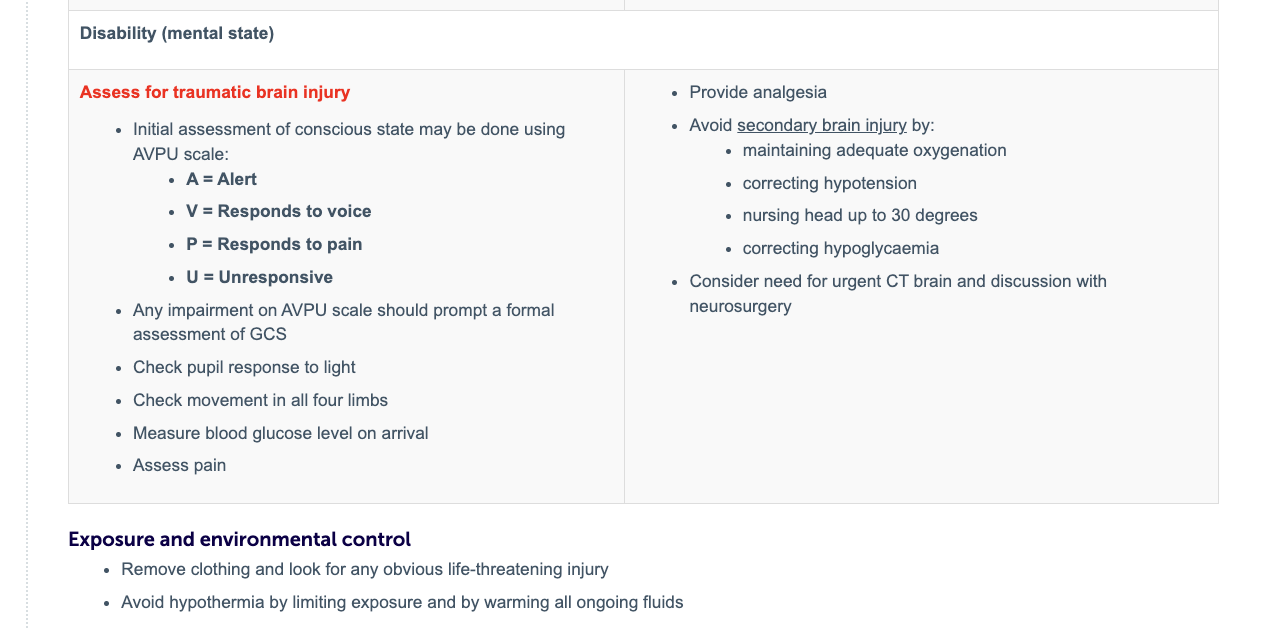
DISABILITY
Paeds trauma continued
Control of exsanguinating external haemorrhage
AIRWAY AND CSPINE
BREATHING
CIRCULATION
DISABILITY
Paeds Trauma
Control of exsanguinating external haemorrhage
AIRWAY AND CSPINE
BREATHING
CIRCULATION
DISABILITY
EXPOSURE
Outline the use of the Broselow tape in paediatric trauma
Uses child’s height or length to estimate weight
If the weight is not known, some centres use the Broselow tape to estimate the child’s weight and to determine drug doses, equipment sizes (e.g. ETT) and energy for DC shock without any calculations
Ensure the tape is rolled out on the receiving bed, ready to use
Tape is laid alongside the child and estimated weight read from the tape
Describe traumatic injury patterns in children that differ from adults, including spinal cord injury without radiological abnormality (SCIWORA) and tension pneumothorax
Kids are small
Trauma affects more organs
Greater dist of force
Connective tissues more elastic therefore shearing forces may tear major blood vessels
Flexible skeletal system means significant organ damage with no overlying fractures
Abdo wall less protected by fat and subcut tissue
LARGE head in comparison to body
Little evidence of external injury
PLUS physiological compensatory mechanisms masks deterioration
remember BP maintained until 30% lost
Common causes of paed trauma
MVA
drown
burns
NAI
Firearms
Falls
Types of injury set patterns according to age
Infant → head injury, big head, thin skull
Young kids → thoracic and abdo - low c of grav
Children < 5y → falls and drowning
Older kids → Limb injuries - higher c of grav
Spinal cord injury without radiological abnormality (SCIWORA)
What
Causes
Ix
Mx
An injury that presents with objective signs of cervical spinal cord damage, but no radiological evidence of fracture or ligamentous instability of the cervical spine
Flex and extension injuries
Fall, MVA
MRI
MTD care and immobilise C Spine up to 3 months
Describe indicators of non-accidental injury in paediatric populations and outline an appropriate course of action when non- accidental injury is suspected
Indicators
Obligations of anaesthetist
Features suspicious of NAI
Injuries inconsistent with history
Child reports adult harm
Multiple injures of differing ages
Delayed presentation
Unusual injuries
Significant bruising, especially in children too young to walk
Fractures in children too young to walk, rib fractures, multiple fractures or long bone fractures in young children
Cigarette burns, well demarcated burns or bite marks
Injuries in inaccessible places such as neck, ear, hands, feet and buttocks
Intra-oral trauma, damage to frenulum, esp in children too young to walk
Genital or anal trauma
Subdural haematoma, retinal haemorrhages
Injury to internal organs with no history of major trauma
Mx of burns
See colourful page
Fluid Mx in burns
Fluid needs to be replaced
Greatest amount is in first 24h
First 8-12h IV to interstitial comps therefore any fluid given will rapidly leave IV comp
AIM MAINTAIN ADEQUATE CIRC VOL
Too little hypoperf
Too much then oedema and tissue hypoxia
MODIFIED PARKLAND FORMULA
3-4 ml x kg x % burn
this gives you ml to give in 24h of Hartmanns
Give half over 8h
Remaining half over 16h
MATINTENANCE FLUID - added to above for kids < 30 kg
4, 2, 1
Analgesia in Burns
Multimodal
Regional block - can be hard infection, gen sepsis
OPIOIDS
Ketamine but beware delirium
Role of gabapentin expanding
IV better than PO
PSYCHOLOGICAL MX
Pathophys of burns
Burns cause thermal injury to the skin, which in turn compromises its protective functions. By doing so, this effective barrier is lost and complications, such as hypothermia and infection, can occur
Massive inflammatory response
Dead tissue
Massive energy demand for temperature and wound healing
Sympathetic response
TO TREAT RESPONSE
Debridement / remove source
No evidence for steroids
Gut may stop working
Feeding issues are possible
Increasing metabolic demands due to dead tissue and wound healing
Increase CO (7x normal)
Need to have adequate nutritional support for severe burns
Raised temp (altered set point - constant high temp)
Respiratory system will +++ to get rid of CO2 being produced everywhere
Loss of skin
Brain should be normal
Renal dysfunction
Muscle breakdown
Key anaesthetic issues of a Burns pt
TEMP MX
ANALGESIA
FLUID MX
ACCESS
Drowning
Def
Hx
Exam
Ix
Mx
Def
is the process of experiencing respiratory impairment from submersion/immersion in a liquid
Mx - key things go think about
VOM is common - Aspiration of vomit is a major comp - place spont breathing kids in left lateral
Hypothermia is a common comp
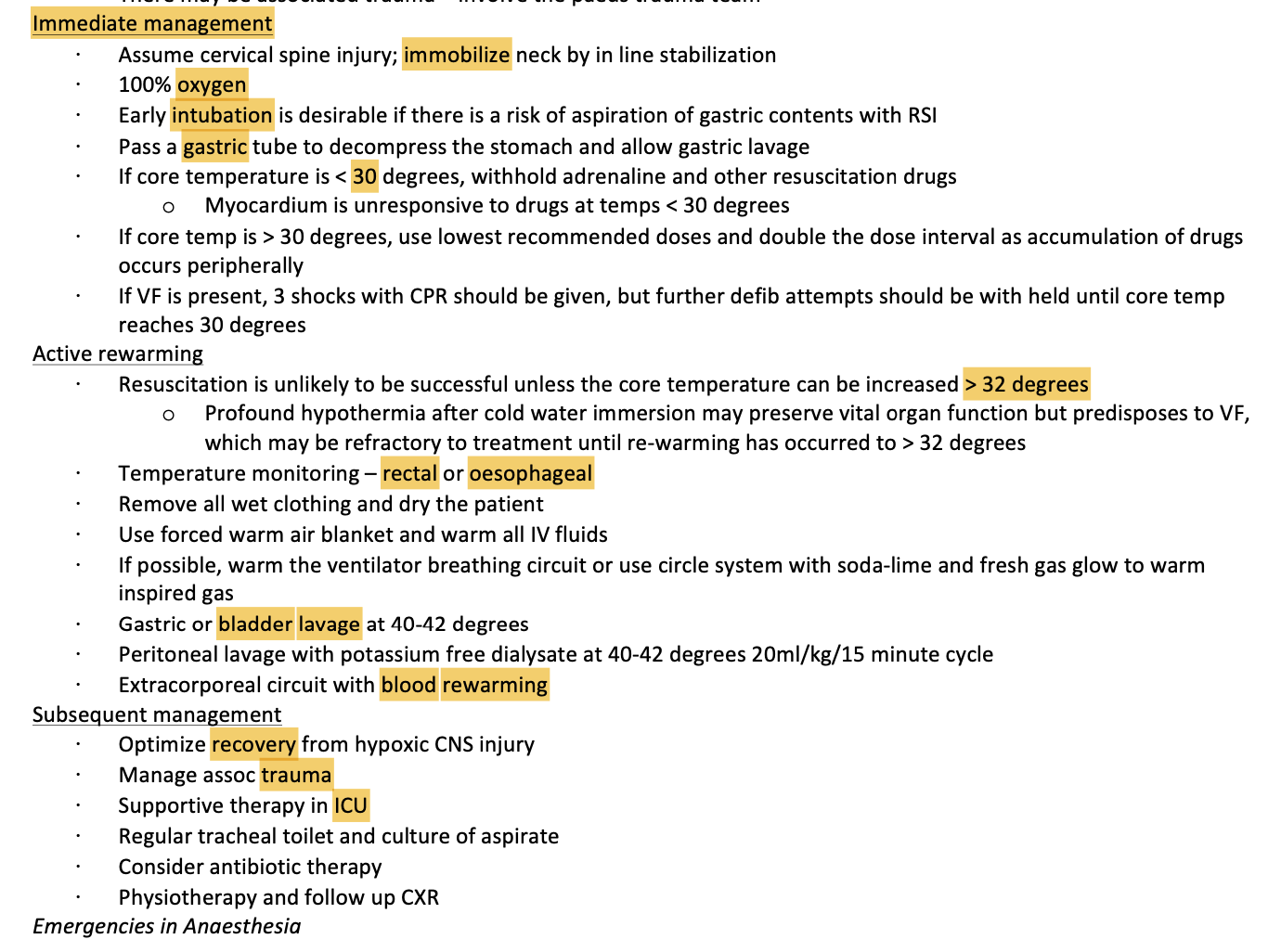
Immediate Mx
Active rewarming
Subsequent Mx