Lecture 12 - Toddler + Preschooler and School aged children
1/81
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
82 Terms
What age range defines a Toddler vs. a preschooler
Toddler = 1+2 years old
Preschooler = 3+4 years old
Toddler + preschooler age is an Important time to establish ____________ and ___________
Healthy food preferences + eating habits
~1 yrs of age = should be eating what the family eats
******Development: What is the progression of MOTOR SKILL DEVELOPMENT?
at what age should they be doing what?
from 12 months to 36 months
WALKING = 12 months
CRAWLING up stairs = 15 months
RUNNING = 18 months
WALKIN up stairs = 24 months
Pedaling on a TRICYCLE = 26 months
Expanded ability for physical activity by 5 years of age (eg. kicking + throwing a ball)
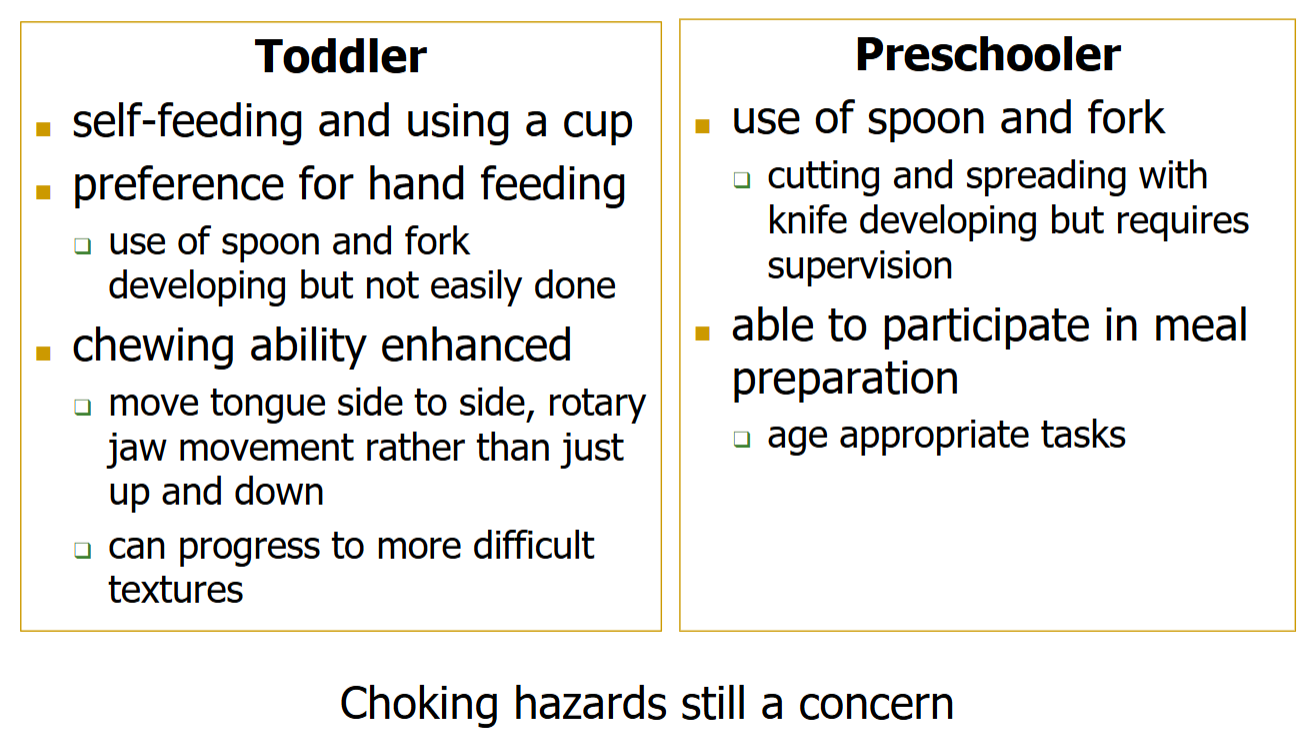
******Compare the Motor development FEEDING SKILLS between a TODDLER + PRESCHOOLER
What method of feeding and aspects related to feeding are they capable of?
Toddler:
Self feeding + using a cup
Preference for hand feeding
Chewing ability enhanced
Preschooler
spoon + fork use
able to participate in meal preparation
*****Development: what are the characteristics of Cognitive + social development in TODDLERS?
Newly discovered INDEPENDENCE+ More INTERACTIVE with broadening social interactions
Observe + IMITATE
learn FAMILY CUSTOMS
FEARS can develop
EXPRESSION OF WILLS: manifesting as negativism + temper tantrums (frustration due to lack of ability to vocalize feeling)
*******Development; Cognitive + social: Language skills of TODDLERS
Language skills expand from 10 words at months to over 100 at ___months
Language explosion during toddler years
10 words at 18 months
over 100 at 24 months
*****Development: what are the characteristics of Cognitive + social development in PRSCHOOLERS?
EGOCENTRISM + magical thinking (eg. tooth fairy + easter bunny etc.)
Increasing social INTERACTION+ COOPERATIVE PLAY (toddlers = play side by side = no interacting; Preschooler = play together)
external behavior limits (affect)🡪 internal limits
TESTING OF LIMITS (control)
******In PRESCHOOLERS when talking about TESTING LIMITS during cognitive + social development, What are the results when:
Too much parental control
Too Little parental control
TOO MUCH = Lowered self confidence + initiative
TOO little = Anxiety
Define egocentrism
Can only think about themselves and not bale to understand what others are thinking
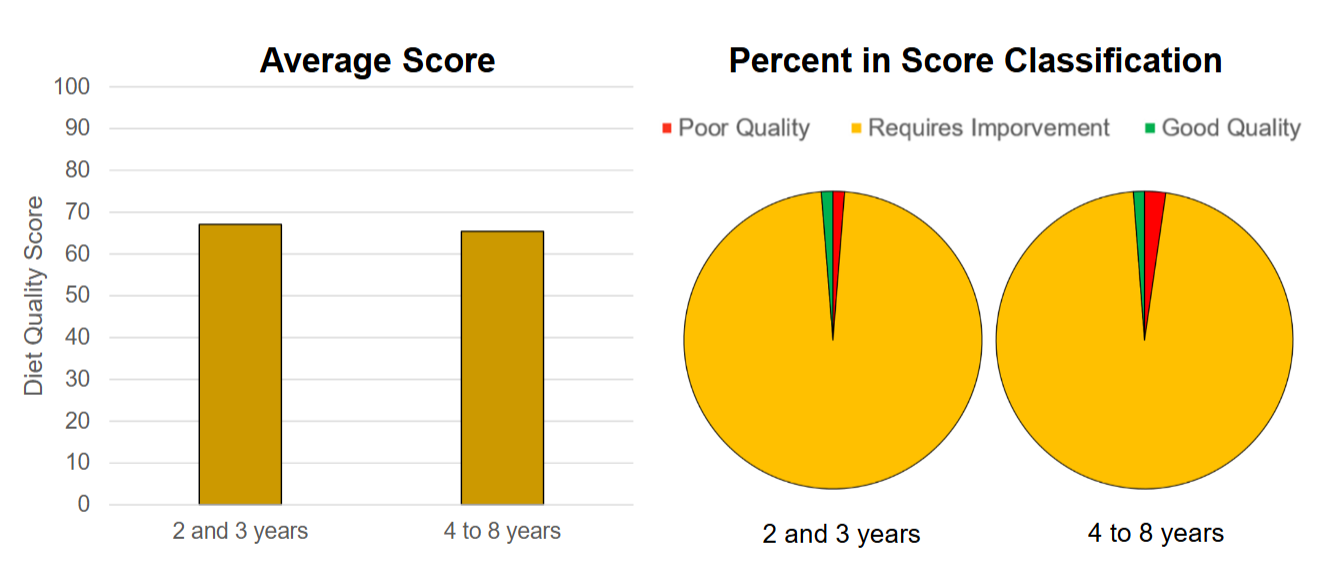
****What is the General Diet quality of Toddlers + preschoolers?
Require improvement
average diet quality decreases from 2-3 to 4-8
*****What is E needed for? What is the factor that most greater influences Energy need of a toddler or preschooler?
E = needed for maintenance, growth + activity
ACTIVITY = the most variable for the child (depends on stage of development, age, etc.)
****What is the formula for EER of a toddler?
EER = (89 x wt in kg -100) + 20
****What is different about the EER calculation for 3-8 year olds?
SEPERATE Formulas for BOYS + GIRLS
take into account wt, height, age + physical activity level
Toddler = only take into account wt
******What is the physical activity recommendations for children 0-4 (toddler + preschool) according to the 24hr movement guideline?
how long should they sit + screen time?
How long should they sleep
How long should they move + intensity of movement
High level of physical activity + low sedentary behaviors + Sufficient sleep
General consensus = Children not active enough for optimum growth
Sit:
Not restrained for more than 1 hour
Less than 2 yrs = NO SCREEN TIME
2-4 yrs = <1 hr screen time
Quality sleep:
0-3months= 14-17
1-2 yrs = 11-14
3-4 yrs = 10-13
Move:
<1 yr = interactive play several times
1-2 yrs = 180min any intensity
3-4 = 180 min + 60 min ENERGETIC play
(remember 1-2 = toddler, 3-4 = preschool)
*****Do preschoolers Toddlers eat enough fiber?
NO (just like everyone else)
Canadian community health survey 2004
9.9 g → 1-3 yrs
13.4 g —> 4-9 yrs
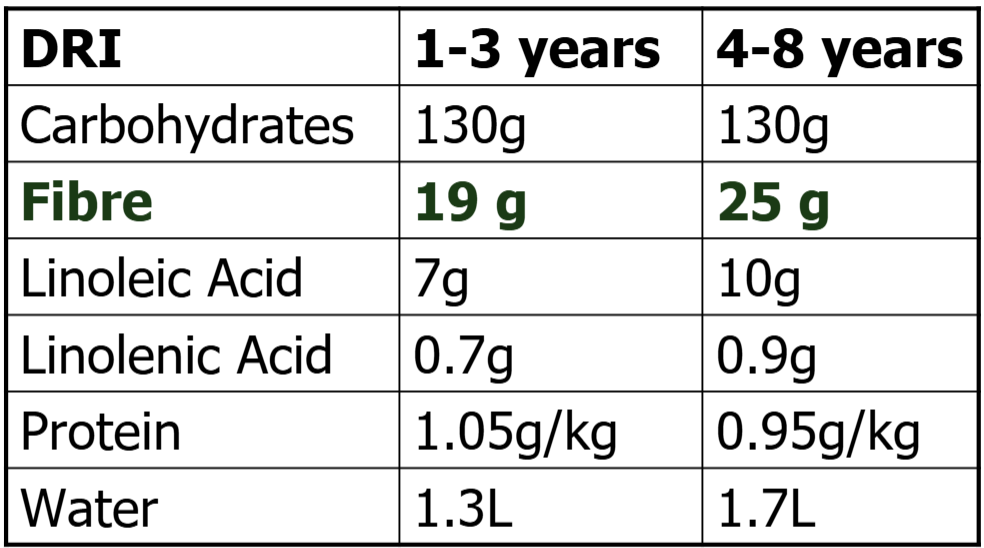
*****What is the FIBRE DRI for toddlers (1-3) + preschoolers (4-8)?
1-3= 19 g
4-8 = 25 g
****What are the Other Macronutrient requirements for 1-3 yrs + 4-8 yrs
Carb levels stay the same
Fiber, Linolenic acid + linoleic acid, and water INCREASE as age increases
PROTEIN per kg = DECREASES as age increases
*****What is the AMDR (acceptable macronutrient distribution range) % E of each macro for 1-3 yrs vs. 4-18 yrs?
1-3 yrs = still emphasizing FAT intake (high)
4-18 = closer to adult AMDR
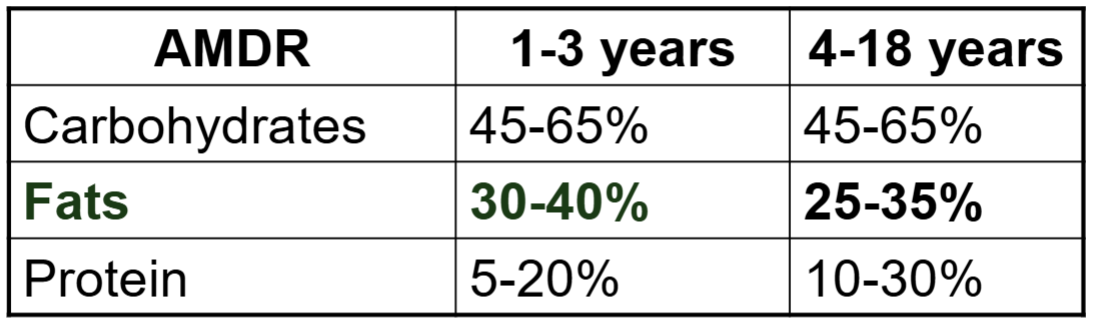
****What are the 2 macronutrients of concern for toddlers + preschoolers?
FIBER
FAT
*****Compare Fat intake in 1-3 yrs vs. 4-8 yrs
1-3 yrs: _____% of fat intake = below + _____% = above
4-8 yrs: _____% of fat intake = below + _____% = above
Younger age = not getting enough fat
1-3 yrs: 47% of fat intake = below + <3% = above
4-8 yrs: 5.5 % of fat intake = below + 6.8% = above
****What are 5 MICRONUTRIENTS of concern for toddlers + preschoolers
WHICH IS THE MOST COMMON nutrient deficiency?
Which has the highest proportion of inadequate intake?
Which has highest EXCESS intake
iron = MOST COMMON deficiency
Ca
Vit D = Most inadequate intake
Sodium = Most EXCEESS intake
Potassium
Iron: ___% of 1-8 year olds had intake below EAR
Ca: ___% of 4-8 year olds had intake EAR
Vit D:____% of 1-3 year olds + ___% of 4-8 year olds had intake below EAR
Sodium: ____% of 1-3 year olds + ___% of 4-8 year olds had intake ABOVE UL
Potassium: Intake vs. AI in 1-8 yr olds
Iron = <5% but is the most common nutrient deficiency despite having less inadequate intake (this can be due to other factors other than intake eg. malaria, absorption, dietary choices etc)
Calcium = 23%
Vit D = 86% (1-3) + 93% (4-8) + MOST INADEQUATE
Sodium = 77% (1-3) + 93% (4-8) MOST EXCESS
Potassium = median intake = BELOW AI (1-8 yrs)
What does Low K and High Na indicate about a food?
LOW nutrient density = PROCESSED FOODS
*****What are the 3 stages of Iron Deficiency?
Depletion of stores
Reduced transport of iron (think 380 low RBC)
Iron deficiency ANEMIA
*****What type of diet is typical of Children that are LOW IN IRON or IRON DEFIENCIENT
Infants not provided iron-fortified foods @ 6 months of age
Young children with HIGH cow’s milk consumption (Ca+ = mineral competition for abs of Fe)
****What are some concern in regards to the impact of IRON DEFICIENCY in children?
Prevalence of deficiency = not clear → large population studies show 1-3% of children 3-11 yrs = iron deficient
concerns impact on COGNITIVE development + LEARNING
*****Iron deficiency in children is MORE prevalent in what population in Canada?
FIRST NATIONS + INUIT
Disadvantaged Urban: 25-50% of children have Iron deficient anemia
*****There should be no fat restrictions for those under the age of_____
2 years
***is a vegetarian or Vegan diet healthy for children?
YES
but it is difficult to get adequate E + Fat for children < than 2 yrs without animal products?
****What are some nutrients of concern for a VEGAN or VEGETARIAN diet for children?
Protein, Vit D + B12, Zinc, Iron, Calcium + Omega 3 (same as for adults)
****What are 2 types of foods recommended for vegan or vegetarian children?
Soy based follow-up formulas (a type of special formula for after 1 yr olds after breast feeding)
Fortified cereals
What are the GOALS of Toddler + Preschooler feeding?
adequate but not excessive E, Nutr + intake
Support normal development (growth, motor, cognitive + Social)
Establish healthy eating patterns + behaviors
Support self regulation of E intake
****Division of responsibility in feeding: What do PARENTS + CHILDREN DECIDE respectively
hint: think the 4W’s + H
Parents = What, When + Where
Child = Whether they eat or not + How much
How to Feed a toddler + preschooler (not too sure what the take away of this slide was)
Role modeling - types of foods, eating patterns, attitudes, activity/screen time/sleep
Foods available + accessible
Food preparation
*****How to feed a toddler + preschooler: What are the suggestions in regards to:
Eating schedule + role modelling
Exposure to new foods
Consistent Eating schedule = VERY IMPORTANT)
planned meals + snacks (With some flexibility)
Remove distractions (eg. electronics) when eating
sit at table with family when possible
Exposure to a variety of food + textures = combat neophobia
offer new foods WITH preferred foods
DO NOT make something specially for them if they won’t eat what you eat (give options within your control)
How many meals + snacks should toddlers + preschoolers eat? What should be the only thing consumed between meals or snacks?
3 meals + 2-3 snacks (2-3 hrs apart)
WATER should be the only thing between meals + snacks
How many Exposures to a new food does it take for a toddler or preschooler to accept it?
15+
see, smell, touch + taste = required before acceptance
***What is the encouraged method of feeding for toddlers + preschoolers? WHY?
encourage self-feeding regardless of messiness
IMPORTNAT for MOTOR skill development + SELF-CONFIDENCE
****What are 4 common Feeding Concerns for toddlers + preschoolers. Give explanation for why some of these occur.
SHOULD THE PARENT BE CONCERNED?
DON’T be CONCERNED generally DOES NOT result in undernutrition
Lack of interest in food + smaller appetite (compared to infancy)
Unpredictable amounts eaten
cause of above: eating will reflect their needs (growth rate decreases with age + occurs in spurts)
Reluctance to try new foods (neophobia)
Picky eating + food jags (only eat 1 thing for 1 week then hate it the next)
****What foods to offer a toddler + preschooler?
formula + breast feeding?
After 12 months formula = no longer needed but breastfeeding can continue (with Vit D supplements to 2 years)
Healthy foods
Variety
Unprocessed or minimally processed should be emphasized
Processed in moderation
Ultra processed = NOT needed
****In terms of BEVERAGE what should and should not be offered?
Beverages other than water should be limited
adequate milk but not excessive
NO sweetened beverages
*****What percent of MILK + what type should be offered until 2 years of age + why?
3.25% (full fat) → no fat restrictions under 2 years of age
other soy or plant based mils are NOT recommended for toddlers (not enough fat?)
soy formula until 2 years if no breast or other animal milk
*****What is the common cause of dental carries in young children?
Use of bottle or sippy cup when sleeping or throughout the day (recommend only H2O between meals and in cups + no sticky foods between meals)
constant exposure to carbs
Sticky foods also increase potential for dental carries
Simple CHO = used by bacteria in mouth → produced acid + erodes enamel
******What is the recommendation when it comes to how much to offer a toddler + preschooler? WHY?
Small amounts of food offered (0.25 or 0.5 servings of each food) → can always get more if not full
Progress to child self-serving from what is offered
Toddler/preschooler decides IF eat + HOW MUCH eaten
WHY = Promotion of AUTONOMY + REGULATION OF APPETITE
****Summarize the article by Birch L.L 2016 Learning to Eat: Behavioral and Psychological Aspects
What is the genetic predisposition of children
Traditional feeding risks + why?
Predisposition= bias to prefer sweet and salty tastes, and to reject new foods and flavors (neophobia)
need to introduce new foods + variety
Traditional feeding: is generally the default method of feeding (evolved to protect children from food scarcity, can be maladaptive in current environments) = increases risk of obesity
Responsive feeding + introduction to new food + variety = promote self-regulatory skills in feeding, beneficial as children are learning to eat in our obesogenic environment.
******What are INTERNAL REGULATION OF E INTAKE?
what is the control center
What are the 3 internal cues
Hypothalamus = control center for hunger + satiety
INTERNAL CUES: signals from nervous system, hormones + blood nutrient levels
***what internal cues trigger Hunger vs. Satiety?
Hunger = Low blood glucose, Ghrelin release, Other hormones
Satiety = stretch, CKK, Leptin + Other hormones
What are some examples EXTERNAL cues that influence the regulation E intake
Define external cues
Definition: Anything that can influence consumption other than feelings of hunger + satiety
Rewards
Peers
Portion size
Praise
social influence (social get togethers involves food)
“clean your plate”
How others around you are eating
Advertisements
Sight, smell + taste
Food as a reward
From the results of food records from toddler + preschool age children reveals _______ (variable/consistent) E intake in individual meals BUT _______ (variable/consistent) daily intake
VARIABLE E from individual meals
CONSISTENT daily intake regardless of the variability of individual meals
*****Info dump on the results of the Fat substitution study
How does the Food intake in toddlers + preschoolers respond to Low vs. High fat foods
Foods tasted the same but diff Fat% = different kcals
Results = Overall E intake in children from both groups = the same
COMPENSATED by adjusting amount eaten based on Kcal
Low E due to Low fat = Increased intake of Carb + protein sources to balance out E intake
*****how do Toddlers + preschoolers respond to Internal vs. External cues (is there an Influence?)
in relation to example of study given in class. High vs. Low Kcal yogurt + Internal vs. External cues effect on the amount of snacks eaten after eating yogurt
Result = EXTERNAL CUES DOES influence amount of food eaten
Internal cues only (no external cues) results = children who consumed lower kcal yogurt before offered snacks = ate MORE snacks than children who consumed higher Kcal Yogurt
children were able to think about how full they feel and consume adequate amounts of kcal based on how they feel
External cues results = children who consumed higher kcal yogurt at an excess of kcal as the external cues prompted them to eat more snacks
******How does parental behavior (praise/rewards) affect Toddler + preschooler food acceptance ?
Does encouraging to eat more affect how much is consumed
Encouragement or rewards does not increase the likelihood to eat a food/ improve food acceptance
it may even DECREASE
******How does Portion size affect amount of food consumed
at what age does portion size become an influence?
What is the take home message?
3.5 years = ate similar amounts of food regardless of portion size (respond to INTERNAL cues)
5 yrs = Increased consumption with Increased portion size
BE AWARE of how much you are giving your child
******How does Modeling affect toddler + preschooler food consumption?
WHO has to be the role model?
Modelling has a influence on food consumption → will change in the direction of the model
PEERS influence (no effect if parents were role models)
Children who didn’t like vegetable before modeling = increase intake of said vegetable
Children who liked vegetable before modeling = decreased intake of said vegetable
****Summary in terms of internal + external cues for toddlers + preschoolers
What are they responsive to
what can effect amount eaten?
Toddlers are responsive to internal cues: E intake variability, Eat more if lower E density
But are starting to become more sensitive to External cues: Praise, rewards, potion size, peers
****What has the biggest influence on toddler + preschooler eating + feeding?
FAMILY
****What ages are defined as School age children:
What ages are considered Middle childhood vs. Preadolescence
Middle childhood = 5-9
Preadolescence = 9-11 GIRLS + 10-12 BOYS
school age is still an important time to establish ______ and _______
establishing healthy food preferences + eating habits
*********What is INCREASING IN INFLUENCE for school aged children?
Increasing influence outside family
*****What are the characteristics of Motor skill development in school aged children?
Improved motor coordination
ability to perform more complex pattern movements
increasing muscular strength
*****Does physical activity start to contribute more or less to energy expenditure in school aged children?
= contributing MORE
E expenditure starts to become highly variable
*****what are school aged children supposed to be able to do in regards to feeding + food skills?
Masted used of utensils
Should be involved in food preparation + chores related to meals
Ready to learn about simple (not complex or “good” vs. “bad” food)nutrition facts + relate to foods they are eating (Eg. this food helps make you strong)
*****What are the characteristics of Social + cognitive development in school aged children?
Decreased egocentrism
More rational cause/effect reasoning (but thinking = concrete not flexible)
Development of sense of self + self efficacy
Increase importance of peer relationships
independence
******How do eating behaviors change in school age children vs. toddler + preschool
eating more meals + snacks away from home
culture of setting (eg. school, sports, extracurriculars) + food availability
increased independence on food choices away from home
Increased influence of marketing
*******In school aged children what has the Strongest influence on food choices?
FAMILY = still the strongest
*******In school aged children what 3 influence on food choices are increasing ?
Peers
Environment outside of home
Media
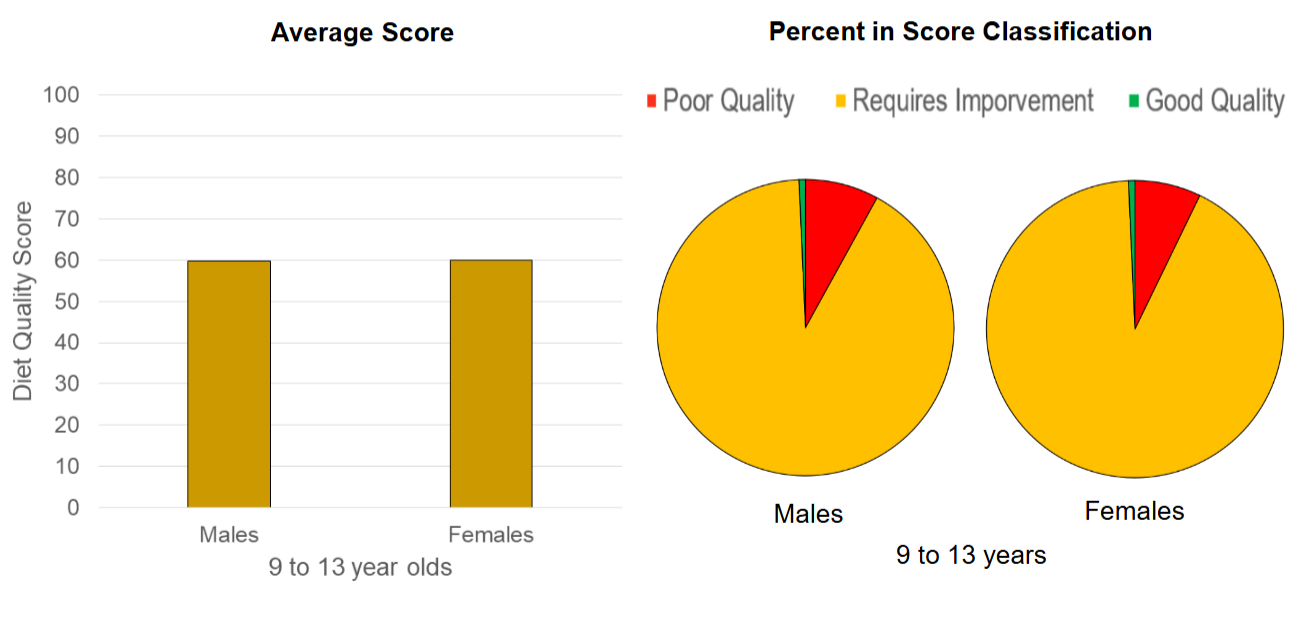
****What is the Diet quality for school aged children how does it compare to toddlers + preschoolers?
Majority = require improvement
poor quality = increased + good quality = decreased
*****In School aged children what has the biggest influence on EER?
EER formula?
E = required for maintenance, growth + activity
PHYSICAL ACTIVITY LEVEL + BIGGEST INFLUENCE
EER
separate formula for Boy + girl
Different formula for 3-8 vs. 9-18
********According to the 24hr movement guideline for 5-17 year olds
how long to sit + screen time
How long to Sleep
Step
Sweat
Sit
Limit sitting for extended periods
no more than 2 hours of RECREATIONAL screen time
Uninterrupted Sleep
5-13 yrs = 9-11
CONSISTENT bed + wake times
Step = Light activity
several hours, structured + unstructured
Sweat = moderate to vigorous
at least ONE HOUR
Vigorous activities, muscle and bone strengthening at least 3 days/week
How is the FIBER intake for school aged children 4-13?
Median intake = BELOW AI
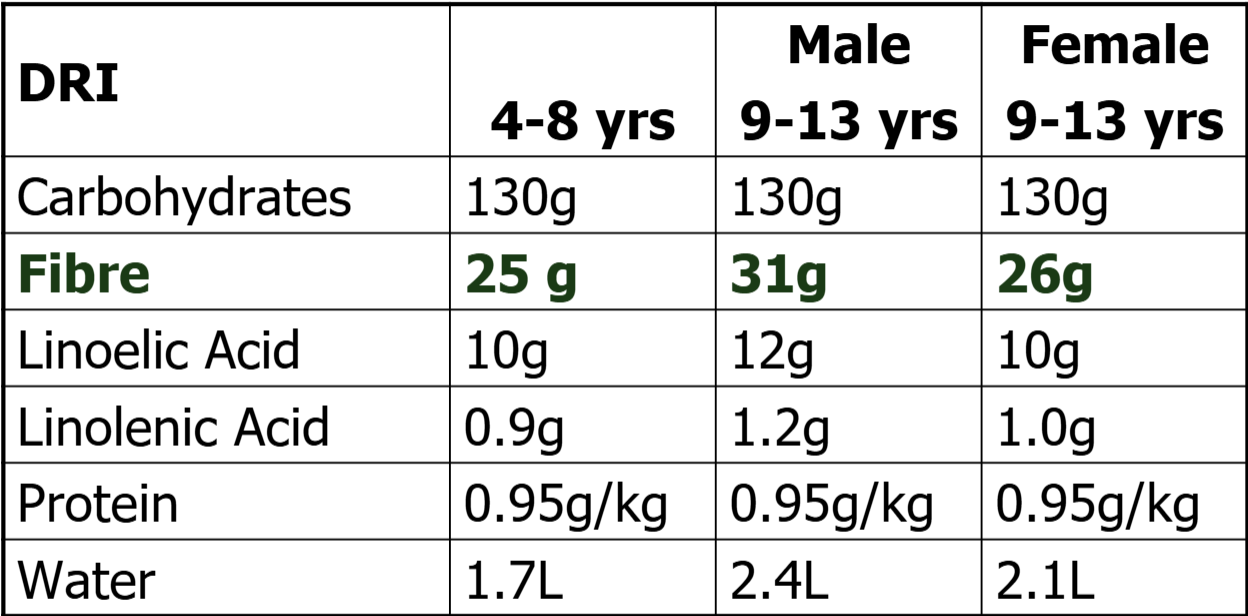
*****What is the DRI for FIBER
Age 4-8
MALE 9-13
FEMALE 9-13
4-8 = 25g
MALE 9-13 = 31
FEMALE 9-13 = 36
fiber intake = calculated as 14g/1000kcal
*****Other than fiber what is the DRI for other MACROS in school aged children?
Carb, Linolenic acid + protein = stay CONSISTENT
Water increases for as you get older
Linoleic acid increases for MALE only
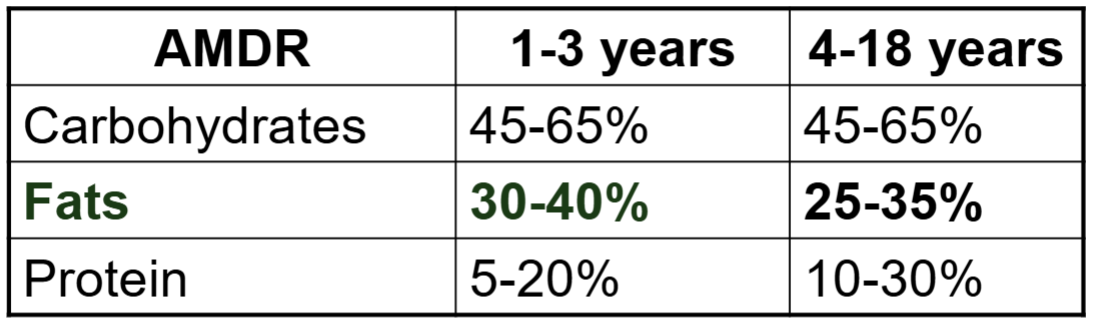
*****What is the AMDR (adequate macro, distribution range) as % of E intake for school aged children 4-18
focus on % of fat
how does it change from toddler/preschool?
FAT decreases as you age
****FAT intake in 9-13 year old school age children:
Girls: ____% of fat intake was BELOW + ___% ABOVE
Boys: ____% intake ABOVE
Boys take in more fat
Generally there is less inadequate intake compared to toddlers/preschoolers
Girls: 6.5% of fat intake was BELOW + 11% ABOVE
Boys: 12% intake ABOVE
*******What are 8 MICRONUTRIENT of CONCERN for 9-13 year olds (intake less than EAR or over UL)
male vs female
IRON
CA
Vit D MOST
Vit A
Magnesium + Zinc: generally for girls only?
Potassium under AI
Sodium = ABOVE UL
Females = MORE DEFICIENT than males
What is the goal when it comes to feeding SCHOOL AGE CHILDREN?
SAME as toddlers + preschoolers
adequate but not excessive E + NUTR intake
Support normal development (growth, motor, cognitive + social)
Encourage healthy eating patterns + behaviors (family = STRONGEST influence)
Support self-regulation of E intake
*******Division of responsibility in feeding for school age children
What do Parents vs. children decide
Parents = What, When + Where
Children = how much + whether
How to feed school aged children (5 points - don’t really get the take away of this slide)
role modeling
Foods available + accessible
Food preparation
consistent schedule
Meals at table without distractions
selecting foods + serving size from what is offered
*****What are some Practices of Parental control that can HAVE NEGATIVE IMPACT
pressure to eat
restriction for weight
Threats or bribes
Intrusive control vs. permissive feeding
Other practices if done with pressure, consequences or overriding internal cues
prompt to eat, rules + limits, redirection + negotiation
*****Body image
when does it start
What can affect/cause?
Negative image + disordered eating can start in early childhood
Trigger/cause:
rebound adiposity can trigger negative opinions of body image
Parents own attitude towards own body wt
Sever restrictions of unhealthy foods + or focus on wt can increase risk of disordered eating in children
******Summary Toddler/preschool + School age
growth rate
impacts on feeding + preferences
diet quality of Canadians
Growth rate DECREACES compared to infancy
Development impacts feeding skills + eating behaviors
Food preferences + behaviors develop early
Division of responsibility with feeding (4 W’s + How; parents vs. child) important in regulation of E intake
Small percentage of Canadian Children have good diet quality, intake of some nutrients = above or below rec.
*****Summary of Development of responsibilities in feeding (W’s + how, parent vs. child)
Infant
Toddler/preschool
School age
Adolescent
Infant
Child = Whether they eat, Where, When + how much
parent = What
Toddler → adolescence
child = How much and if they eat (Whether)
Parent = What + When + Where