Unipolar Depressive and Bipolar Disorders
1/94
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
95 Terms
What is the definition of depression in a clinical context?
A mood state characterized by feelings of sadness, hopelessness, emptiness, lack of joy, and/or despair that impairs functioning.
What are the three main components of the 'What causes depressive disorders?' model?
Predisposing vulnerability (genetics, personality, history), triggers (life stressors/adversity), and biological response (brain and systemic changes).
What are the three proposed biological pathways of depression?
1) Monoamine Dysregulation
2) Neuroendocrine Dysfunction
3) Dysregulation of inflammatory cytokines
What are the prevalence risk factors for depression?
Average onset of 30 years old, Females, Native Americans, low incomes, isolation
What are symptoms of depression?
Appetite change, insomnia, anhedonia, dysphoria, fatigue, agitation, decreased concentration, low esteem, guilt, suicidal thoughts
What are physical signs of depressive disorders?
Poor self care, withdrawn behavior, reluctance for eye contact, brief answers to questions, decreased motor activity, depressed or tearful affect
What laboratory tests are typically considered during the evaluation of a patient with suspected depression?
TSH, CBC, CMP, A1C, B12/folate levels, HCG (pregnancy test), and Urine Toxicology
What are the two core symptoms required for a diagnosis of Major Depressive Disorder (MDD)?
At least one of the following: depressed mood or markedly diminished interest/pleasure in activities (anhedonia).
How many symptoms must be present for MDD and for how long?
2 or more weeks of at least 5 symptoms that cause significant distress or impairment
What other symptoms aside from the required two may be present to meet the "5 symptom" minimum?
weight loss/gain, appetite change, insomnia/hypersomnia, psychomotor agitation, fatigue, feelings of worthlessness or guilt, difficulty concentrating, recurrent thoughts of death
What is a key exclusionary factor for an MDD diagnosis?
the patient must never have had a manic or hypomanic episode
What are the severity scores for the PHQ-9 screening?
Mild: 5-9
Moderate: 10-14
Moderately severe: 15-19
Severe: ≥ 20
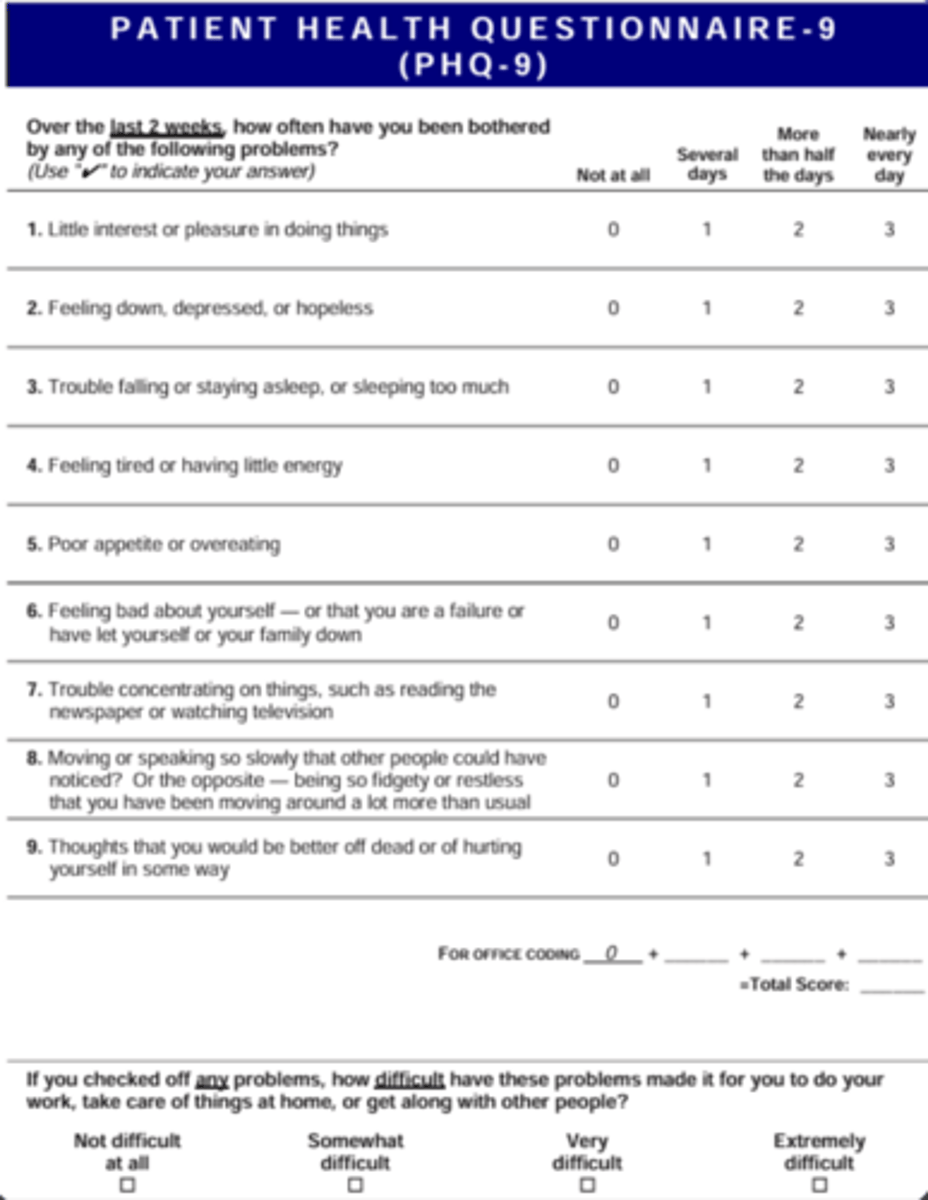
What PHQ-9 score indicates a possible depressive disorder requiring further evaluation?
Score ≥ 10
What are the strong health associations of depression?
CAD, DM, Parkinson disease, Stroke
How does Major Depressive Disorder affect all-cause mortality?
It is associated with a 50-100% increase in all-cause mortality; increase risk of suicide up to 17x
What is the epidemiology of suicide?
- Attempts are twice as common in females and 3-5x greater in young adults 18-25 years old
- Completions are 2-4x more common males
- Deaths highest in >75 years and 45-64 years
What are the risk factors of suicide?
prior attempt, self-harm history, family history of psyche illness/suicide, recent severe loss, isolation, lack of social support, substance abuse
What are the risk factors for suicide in children and adolescents?
Impulsiveness, hopelessness, intellectual disability, life stressors, ACEs, disciplinary problems, troubled relationships
What is the immediate management step if a patient has suicidal intent or a plan?
contact a crisis hotline or 911
What is the management of mild MDD (≥5 symptoms and score of 5 to 9)?
CBT or active surveillance
What is the management of moderate MDD (≥5 symptoms and score of 10 to 19)?
Antidepressants or CBT
What is the management of severe MDD (≥7 symptoms and score of ≥20)?
Combination therapy with antidepressants and CBT
Which antidepressant class is generally preferred as first-line treatment for MDD?
SSRI's are preferred. SNRI and atypical antidepressants may be used an alternative
What side effects of SSRIs (Prozac, Zoloft, Lexapro) should be monitored during pharmacotherapy?
stomach upset, dry mouth, restlessness, sexual dysfunction, weight changes, and suicidality
When is an SNRI (Cymbalta, Effexor) preferred?
patients with comorbid pain disorders or experiencing side effects that impair compliance
When is Bupropion (Wellbutrin) preferred?
patients with ADHD or nicotine use; has no sexual dysfunction or weight gain but must be avoided in patients wtih seizure disorder
When is Mirtazapine (Remeron) preferred?
patients with significant insomnia and weight loss/lack of appetite
When is Trazadone perferred?
Significant insomnia because it is very sedating
What is the recommended minimum duration of pharmacotherapy for acute MDD?
At least 6 months to 1 year.
What is Treatment Resistant Depression (TRD)?
Depression unresponsive to 2 trials of antidepressant therapy (sufficient doses and durations)
What is the management of TRD?
Switch antidepressant or augment with atypical antipsychotics, bupropion, mirtazapine, or newer medications like esketamine
What are referrals for more severe forms of TRD?
Transcranial Magnetic Stimulation (TMS) and Electroconvulsive therapy which is the most effective treatment for TRD
What is the management for mild episodes of MDD in children/adolescents?
psychotherapy alone
What is the management for moderate-severe episodes of MDD in children/adolescents?
pharmacotherapy + psychotherapy
What is the first-line antidepressant therapy for children and adolescents?
Fluoxetine
What is the recommended treatment for TRD in children and adolescents?
Sertraline; refer to psychiatry if needed
How long must pharmacotherapy be used for to see mood improvement?
At least 6 weeks
What are the recommendations for monitoring of MDD?
Follow up in 2 weeks, then every 4-6 weeks. At every visit PHQ-9 is assessed, adherence to medications, adverse effects, and suicidality
What is Persistent Depressive Disorder?
Chronic, longstanding depressive symptoms that are less severe than major depressive disorder
What is the primary presentation of persistent depressive disorder?
Patients often cannot recall a time where they didn’t feel depressed: “I’ve always been this way”
What is the diagnostic duration requirement for Persistent Depressive Disorder in adults?
At least 2 years of depressed mood for most of the day, more days than not WITHOUT symptom free-periods that last longer than 2 months
What is the diagnostic duration requirement for Persistent Depressive Disorder in children?
1 year or more of depressed or irritable mood and at least two other symptoms
What other symptoms may in which two may be present for a diagnosis of persistent depressive disorder?
poor appetite, overeating, insomnia, hypersomnia, fatigue, low self-esteem, poor concentration, indecisiveness, feelings of hopelessness
What is the primary treatment approach for Persistent Depressive Disorder?
CBT combined with pharmacotherapy, typically using SSRIs.
What is Premenstrual Dysphoric Disorder (PMDD)?
physical and affective/psychologic symptoms that occur during the second half of the menstrual cycle (luteal phase)
What is the proposed pathology behind PMDD?
Serotonin dysfunction in response to estrogen and progesterone fluctuations in the last 14 days of menstrual cycle (luteal phase)
What are the diagnostic criteria for PMDD regarding symptom count?
1 affective symptom plus 5 other symptoms that consistently causes distress or interference in daily activities
Which symptoms in which 1 must be present are required for a PMDD diagnosis?
mood swings, sudden sadness, increased sensitivity to rejection, anger/irritability, hopelessness, tension and anxiety
Which symptoms in which 5 must be present are required for a PMDD diagnosis?
decreased concentration, change in appetite, decreased interest, fatigue, feeling overwhelmed, breast tenderness, bloating, weight gain, joint pain, insomnia/hypersomnia
What is the recommended treatment for PMDD?
SSRIs are first line that can be taken daily, during luteal phase, or at symptom onset until day 2-3 of next cycle
What is the alternative for SSRI treatment of PMDD?
Oral contraceptives
What is Seasonal Affective Disorder (SAD)?
Recurrent episodes of major depression, mania, or hypomania with seasonal onset and remission
Which disorders is SAD a subtype of?
Unipolar major depression (major depressive disorder), Bipolar I and II
What is the most common presentation of SAD?
Recurrent episodes of unipolar depression beginning in the fall or winter and remit in the following spring/summer
What is the diagnostic requirement for the seasonal pattern in SAD?
Onset and offset at a characteristic time of year for the last 2 years, with no nonseasonal episodes
What is the first-line treatment for Seasonal Affective Disorder?
A combination of SSRIs and light therapy.
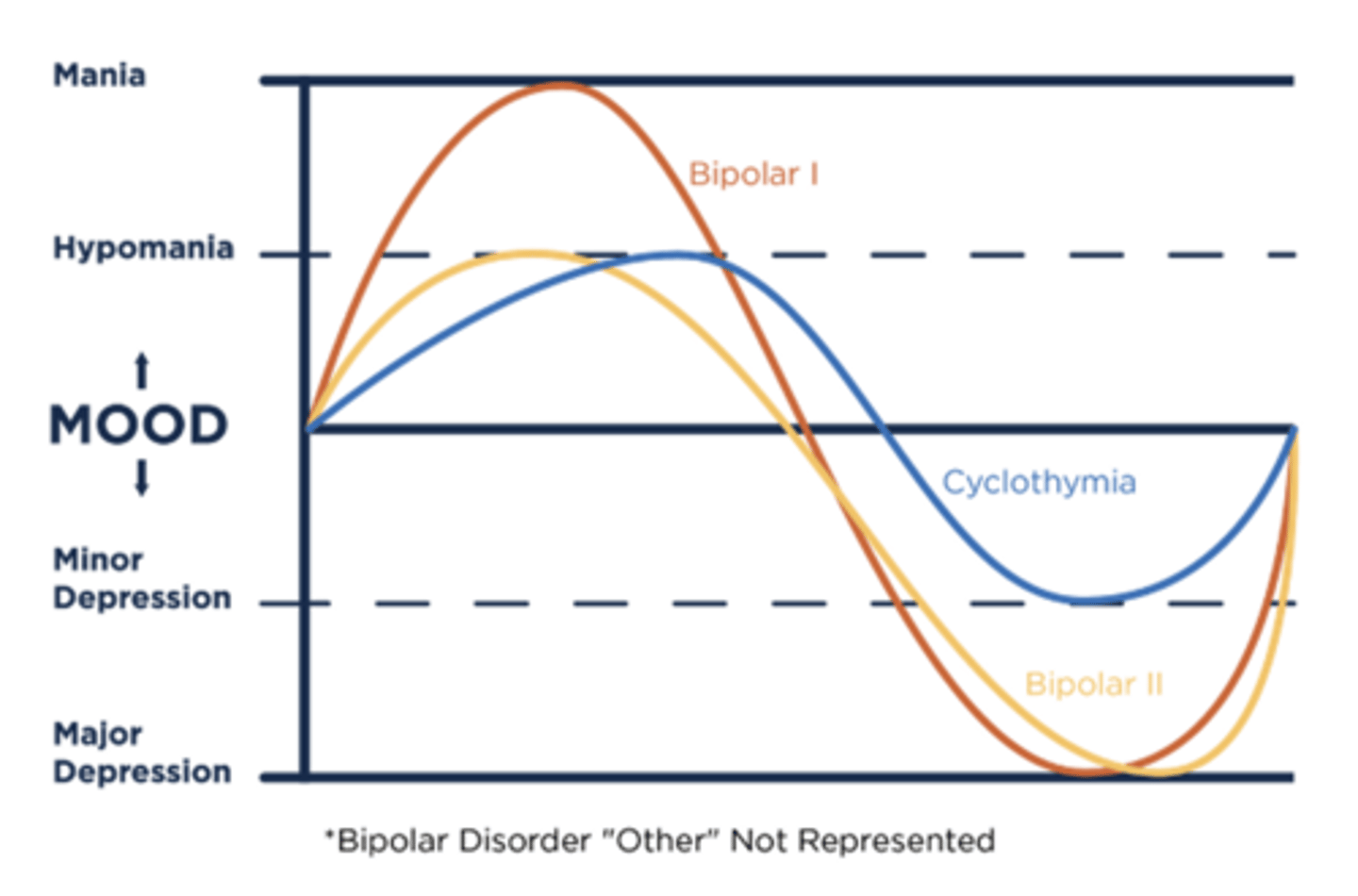
What are Bipolar Disorders?
characterized by mania and/or hypomania that may be combined with distinct major depressive episodes
What is the key difference between Bipolar I and II?
Bipolar I has mania episodes whereas Bipolar II has hypomania episodes
What labs should be obtained for new onset mania?
CBC, CMP, TSH, T3/T4, urine tox, syphilis screen
What are physical signs of mania?
disheveled, hyperactivity, euphoric, loud, uncooperative, agitated, labile, delusional thought content
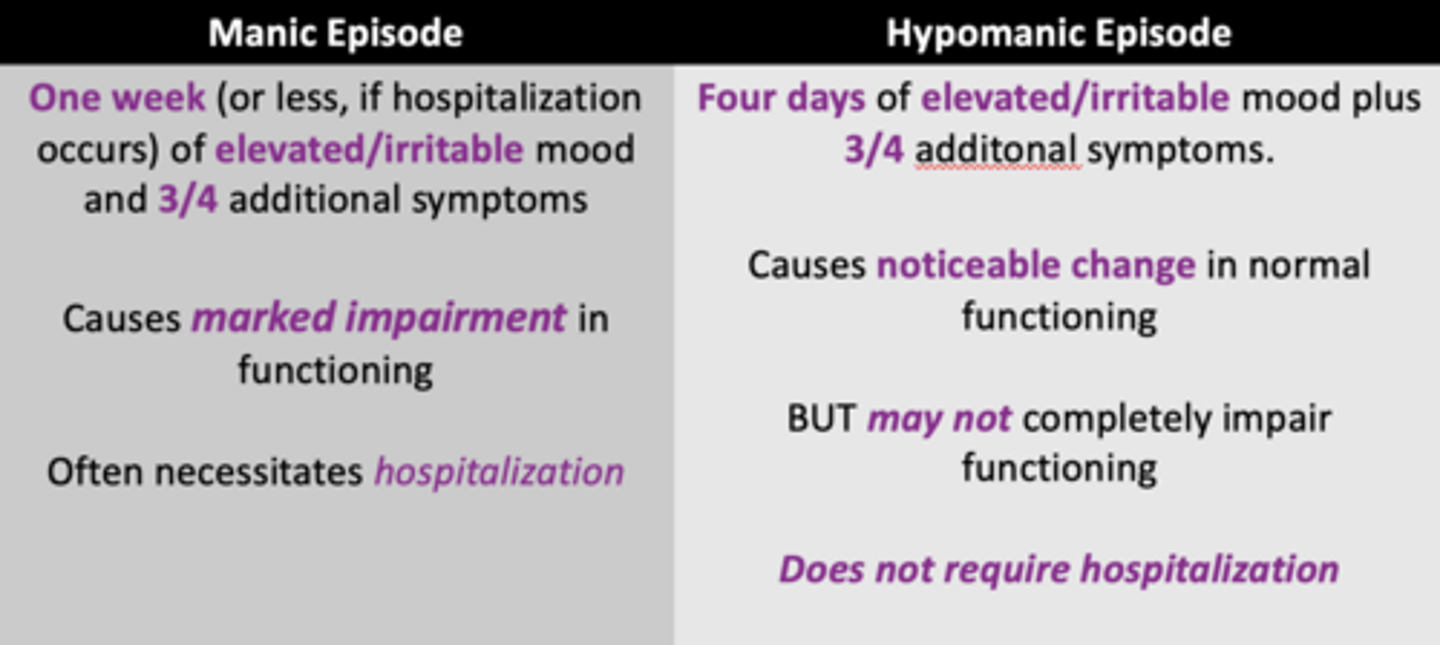
What is the diagnostic criteria for a manic episode?
≥ ONE week (or less if hospitalization required) of persistently elevated, expansive, or irritable mood AND
increased energy and activity
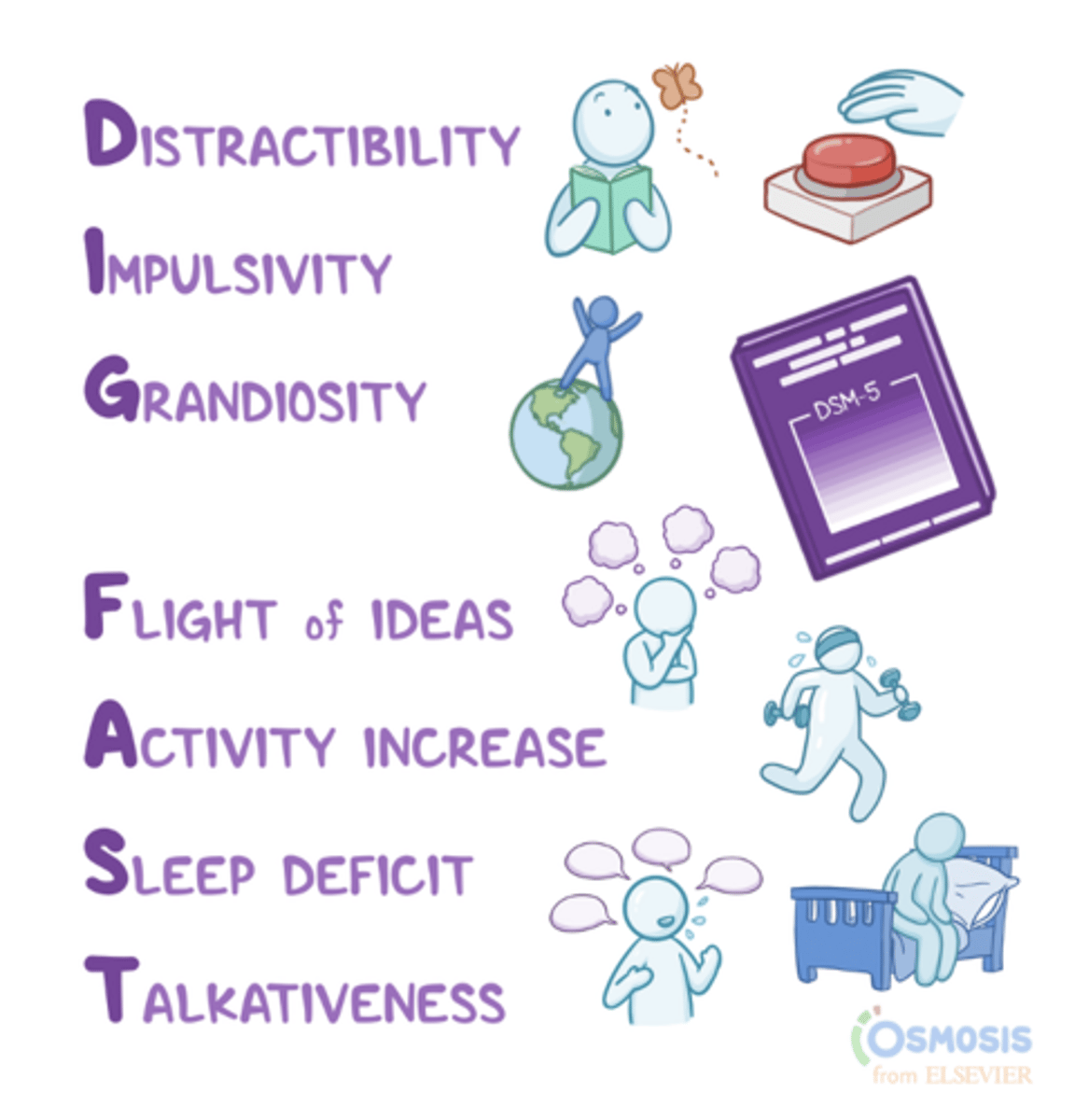
What other symptoms in which three (four if mood is only irritable) must be present for diagnosis of a manic episode?
grandiosity, decreased need for sleep more talkative than usual, flight of ideas, distractibility, increased goal-directed activity, excessive risk taking behavior
What is the diagnostic criteria for a hypomanic episode?
≥ FOUR days of persistently elevated, expansive, or irritable mood AND
increased energy and activity
What other symptoms in which three (four if mood is only irritable) must be present for diagnosis of a hypomanic episode?
grandiosity, decreased need for sleep more talkative than usual, flight of ideas, distractibility, increased goal-directed activity, excessive risk taking behavior
What other differentiating factors does a hypomanic episode present with?
causes unequivocal change in functioning that is noticeably observed by others
What is the primary difference between a manic episode and a hypomanic episode?
Severity and duration; mania causes marked impairment or requires hospitalization, while hypomania does not.
What often precedes mania or hypomania?
a major depressive episode which may cause misdiagnosis of MDD prior to manifestation
What are the risk factors for bipolar disorders?
average onset of 18-20 years old, family history in first degree relatives, and comorbid psychiatric condition
What are some common outpatient chief complaints for patients with Bipolar Disorder?
Depression, racing thought, insomnia, impulsive behaviors, paranoia, delusions, and hallucinations
What physical exam findings might suggest a Bipolar Disorder presentation?
Poor self-care, intense affect, inability to concentrate, erratic speech, or significant anxiety.
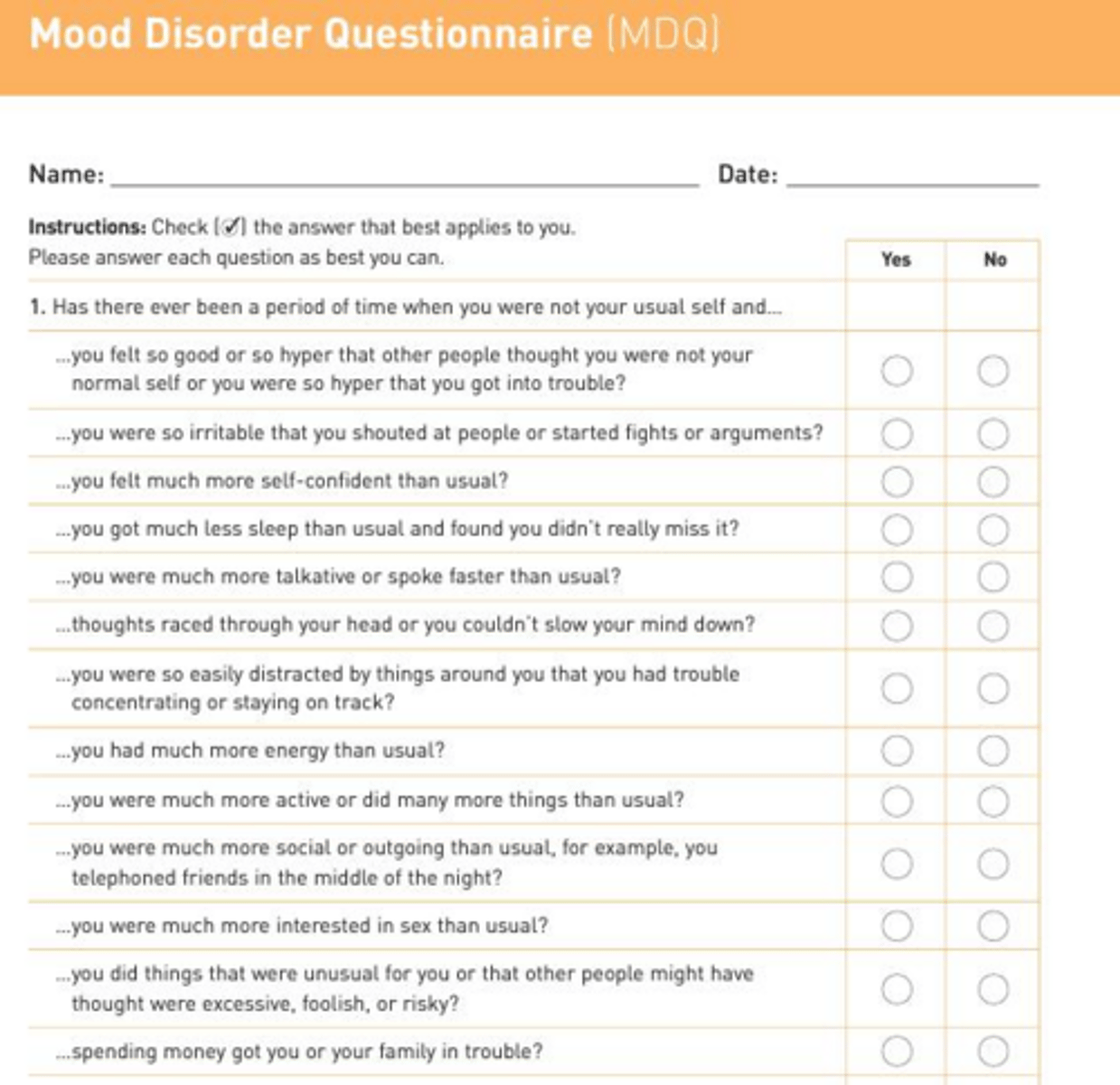
What can be used to help diagnose bipolar disorders?
The Mood Disorder Questionnaire (MDQ)
What is the diagnostic criteria for Bipolar I Disorder?
Any presence of a manic episode ≥ 1 week or with hospitalization
What is the diagnostic criteria for Bipolar II Disorder?
Major depressive episodes alternating with hypomanic episodes; must NEVER have a manic episode
What is rapid cycling in bipolar disorder?
≥ 4 distinct mood episodes in 12 months that must be separated by full/partial remission (at least 2 months) or a switch to the opposite pole
What are the associations with rapid cycling?
more severe illness course, increased functional impairment, higher suicide risk, and more difficult treatment response
What is the general recommended pharmacotherapy to treat mania and depression for Bipolar I?
1) Lithium
2) Valproate
3) Quetiapine, aripiprazole
What is the general recommended pharmacotherapy to treat mania and depression for Bipolar II?
1) Quetiapine
2) Lithium
3) Lamotrigine
What is the first-line treatment for acute mania?
Lithium with close monitoring at onset and during treatments (q2-3 months for 6 months) of calcium, creatinine/GFR, TSH, and T4
What is the advantage of using lithium for Bipolar management?
Very effective for bipolar major depressive episodes and decreases suicide risk
What is the target serum level for lithium in bipolar disorder?
0.8 - 1.2 mEq/L.
What are the alternative treatments for acute mania?
Valproate and Carbamazepine; neither can be used in pregnancy!
Which mood stabilizer is a first-line maintenance treatment for bipolar II with prominent depression?
Lamotrigine; black box warning for SJS and TEN (monitor at initiation)
Which second-generation antipsychotic is specifically approved for acute mania and depression?
Quetiapine (Seroquel)
Which two second-generation antipsychotics are only used for bipolar major depression?
Lurasidone (Latuda) and Lumateperone (Caplyta).
What is the recommended dual therapy for severe mania?
Lithium or valproate (mood stabilizer) PLUS antipsychotic
What are the most common extrapyramidal symptoms while using second-generation antipsychotics?
Akathisia (MC), Dystonia, Parkinsonism, Tardive Dyskinesia
What is the management of Tardive Dyskinesia?
Needs ASAP recognition to prevent permanent effects; administer VMAT2 inhibitors like Valbenazine and Deutetrabenazine (avoid benzotropine)
What can be used as an adjunct therapy for treatment of bipolar disorder?
SSRI and SNRI for bipolar major depressive episodes ONLY in combination and should be discontinued if polarity switch occurs
What is the first-line adjunctive psychotherapy for bipolar disorder?
Group psychoeducation.
What are the differences in presentation of bipolar disorder in pediatrics?
more irritability, labile/erratic mood changes, mixed features of psychotic symptoms, rapid cycling high comorbidity of ADHD/disruptive disorder
What are the first line treatments for pediatric bipolar disorder?
Lithium, atypical antipsychotics, psychoeducation and family-focused therapy
What are the diagnostic criteria for Cyclothymic Disorder regarding duration?
At least 2 consecutive years of mood elevations/depressions that do not meet full criteria for hypomanic or major depressive episodes.
In Cyclothymic Disorder, what is the maximum duration a patient can be without symptoms?
No more than 2 months.
What are some key differentiating factors of Cyclothymic Disorder from Bipolar disorders?
Chronic, fluctuating mood disturbances without clear delineation of episodes that persist over years
What is the treatment for Cyclothymic Disorder?
Mood stabilizers (lithium, lamotrigine, valproic acid) OR second generation antipsychotics