OMM Practical
1/24
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
25 Terms
Describe the movement of:
Pump Handle
Bucket
Caliper
Pump Handle:
R1-6
Inhalation = Ant + Sup.
in sagital plane
Best felt in mid-clavicular
Axis of motion: transverse (along the costovertebral/costotransverse line)
Bucket:
R7-10
Inhalation = Lat + sup
In Coronal Plane
Felt at Mid Ax. Line
AOM: AP
Caliper:
R11/12
Inhaltion = Post + Lat
Transverse Plane
Felt @ 2-5cm lat. to transverse process
Axis = vertical line
Which Ribs are A/Typical
What makes the ribs atypical
Typical: 3-9
Atypical: Rest
Atypical:
1:
only one facet that articulates with T1.
Has internal tubercle for attachment of anterior scalene muscle.
no angle.
2:
large tuberosity on shaft for the serratus anterior muscle.
10:
only one facet that articulates with T10.
Ribs 11 and 12:
articulates with only one vertebra
lacks tubercles and subcostal grooves.
how does the rib articulate w/ the vertebra
Rib articulation:
@ 3 points:
Costotransverse facets
Sup/inf. costovertebral joint?
Inf/Sup facts
NOTE: Rib 3 articulates w/ Vertebra 2/3
Differentiate between respiratory and structural ribs
Structural:
non-physiologic
affects single rib
treated before respiratory
Superior/Ant/Post Somatic Dysfunction
respiratory:
Physiologic
In groups
Treated after structural
Inhalation/Exhalation Somatic Dysfunction
Describe procedure for Structural ME
Rib 1 Superior:
Knee on table, pt arm across knee on Contralateral side
Pull trap posteriorly; push down and anteriorly on the First Rib
Tilt Head towards affected side; Pt push contralateral side
Reciprocal Inhibition
Anterior:
Patient Arm is flexed/adducted
Thumb = medial to Angle → Pushed Laterally
Patient will push laterally or Inferiorly
Posterior:
Pt. Arm is flexed/adducted
Thumb = Lat to angle → Pushed Medially
Patient will push Medially or Superiorly
What type of muscle energy technique is used to treat posterior/anterior ribs
joint mobilization using muscle force
What is the Key?
Jordan
Inhalation SD = Lowest Rib
Exhalation SD = Highest Rib
Which Muscles are treated for exhalation SD for each rib?
Anterior and Middle Scalenes = Rib 1
Posterior Scalene = Rib 2
Pec Minor = Ribs 3-5
Serratus = Ribs 6-8 (although it attaches to all 1-8)
Lats = Ribs 9-12
AMP targeted Minors using a Serrated knife in LA(T)
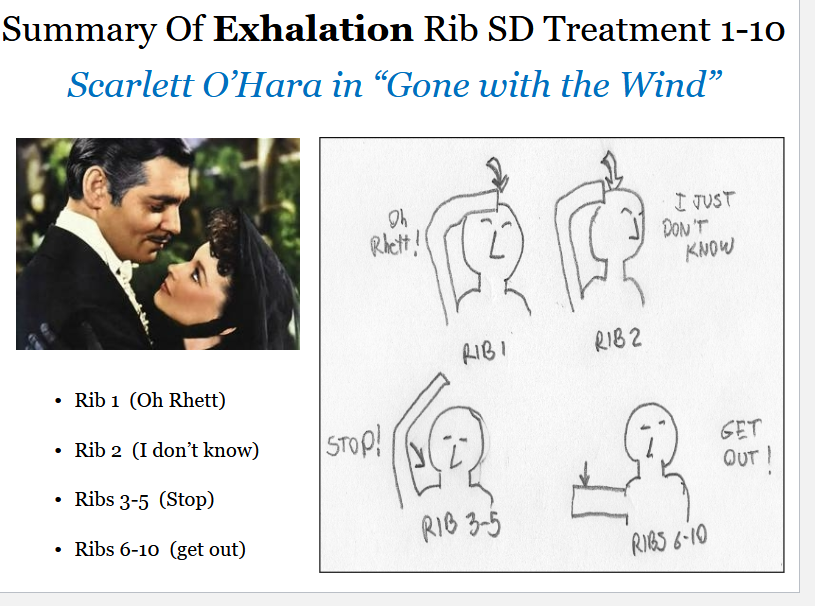
Explain how you would treat exhalation SD
How would you treat Inhalation SD
1: Flexed Neck
2-6: Neck/Shoulders Flexed and sidebent TOWARDS
6-10: Entire Pt is side bent TOWARDS
Describe type of muscle energy used for Inhalation/Expiration ribs
Inhalation: Respiratory Assist
Exhalation: Direct + Joint Mobilization
Define Articulatory Tech
How do You disengage the two joints
Where are your finger tips?
Low velocity, moderate to high amplitude technique where a joint is carried through its range of motion engaging a restrictive barrier
repeatedly with the goal of increasing that range of motion to the physiologic barrier
CostoTransverse: Disengage by pushing down using the fulcrum
Costovertebral: Apply lat. traction to rib angle as cage is lifted
Finger tips = medial to Angle
How to perform HVLA for posterior Ribs
NOTE: how do you localize?
Patient supine. Stand on the side opposite the posterior rib
Cross patient’s arms with the dysfunction side arm superior and their elbows close together.
Rotate patient’s dysfunction side shoulder toward you using your cephalad hand
Reach under your partner with your caudad hand’s thenar eminence to contact the rib angle
Roll patient back onto your thenar eminence.
Place patient’s crossed elbows in your abdomen (not rib cage or sternum)
Lift head and neck and flex partner down to the level of the dysfunctional rib
Side bend patient away from the dysfunction (toward you) to the level of the dysfunctional rib to open costovertebral joint
Further fine tune localization forces to the costovertebral articulation by applying force with your abdomen, through the patient’s arms. The angle needed to localize will vary between patients (in the direction you found previously).
With each respiration, take up the “slack” and compress more until you are firmly at the barrier.
With all planes of available motion localized at the barrier of rib motion, at the end of partner’s exhalation, thrust posteriorly from your abdomen onto the dysfunctional rib. The direction of thrust matches that which you needed to localize at the fulcrum hand.
Localization:
Shift Body until elbow in abdomen → Vector = Superiorly (inhalation SD) or Inferiorly (Exhalation SD)
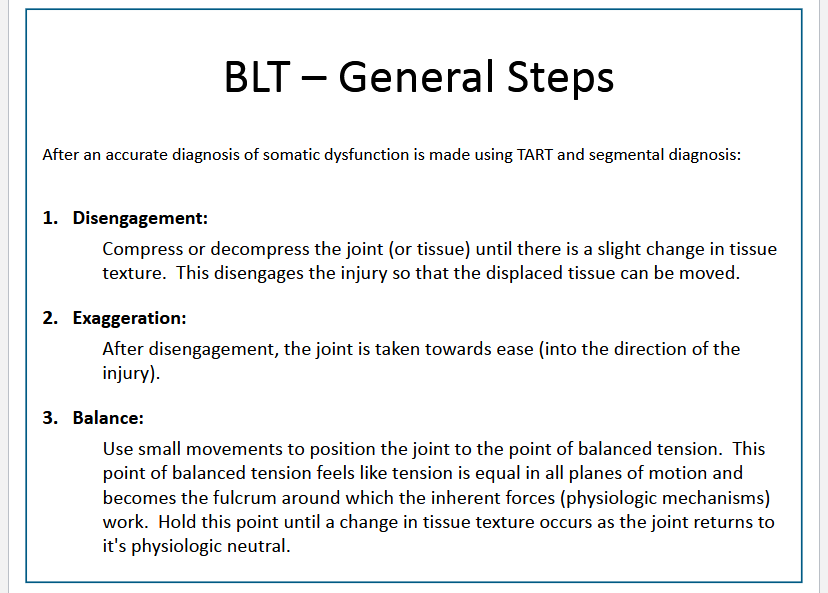
[REVIEW] BLT general Steps
Describe how to do BLT on Ribs
2-11:
Pt supine → Physician on side w/ dysfunctional rib.
stabilizes rib by grasping the rib shaft one hand anteriorly and one hand posteriorly.
arm of the patient lies between the physician’s arms.
anterior and posterior compression is added to the dysfunctional rib to create disengagement.
Then a lateral traction is added with both contacts.
BLT time
12:
Pt Supine:
apply both middle fingers under the tip of the 12th rib.
Disengage @ both joints by applying inferiolateral traction
BLT time
Differentiate between type 1 and type 2 dysfunctions
Type 1: Neutral
Type 2: FRS/ERS
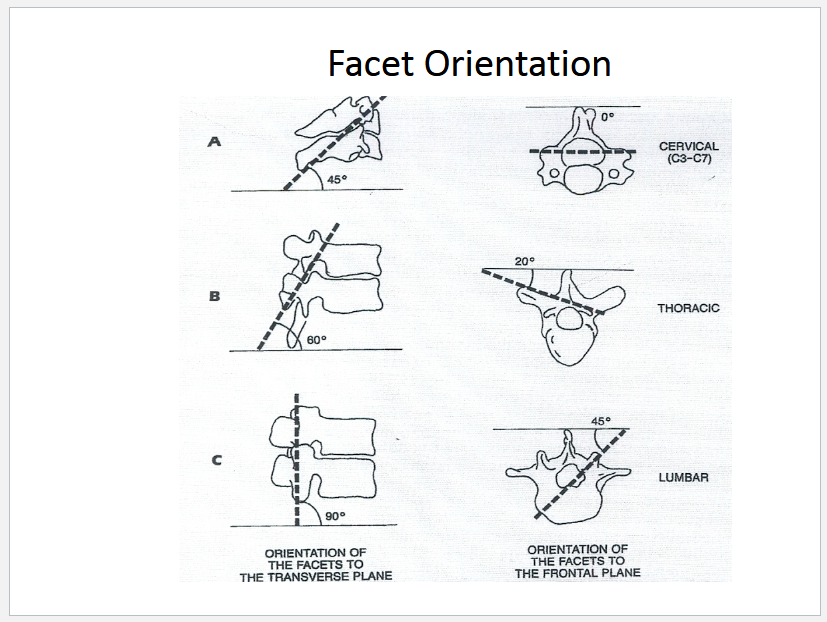
Describe the orientation of the articulation w/ the superior articular facets of various vertebras
Does a type 1 SD consist of one vertebral segment or multiple adjacent vertebral segments?
Multiple
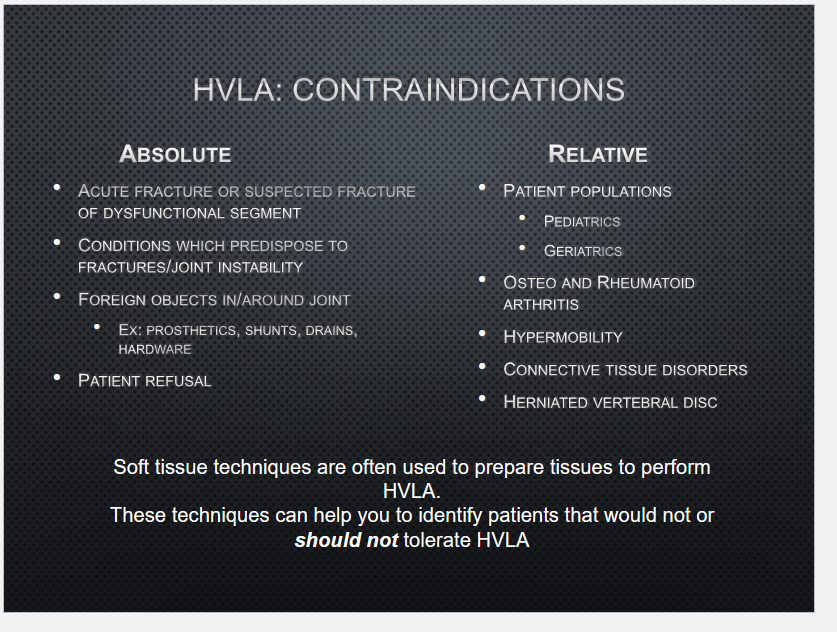
[REVIEW] Contraindicatiosn of Lumbar HVLA
How do you do HVLA of the Lumbar
L2-FRS Left:
Pt lies on LEFT SIDE ( SAME SIDE THE PATIENT IS SIDEBENT TOWARD)
Phy monitors the interspinous space between L2 and L3
Phy induces extension @ interspinous space using the lower and upper extremeties (note, one hand has to be monitering space @ all time)
Pt. straighten bottom leg and right foot is placed in popliteal fossa
Pt. LEFT arm is used to pull left shoulder anterioly → Right rotation of Torso down to dysfunction segment
Phy grabs Pt Left Elbow → pulled cephalid → Right Side Bending above apex of dysfunction
NOTE: @ this time, pt is right rotated, right side bend, and extended
PHY places right forearm on anterior aspect of the patient’s right chest/shoulder .
PHY places left forearm on inferior aspect of the patients right iliac crest
HVLA TIME: Left FA → Ant + Sup Force; Right FA = counterforce
How do you do BLT of Lumbar Vertebra
BLT:
Disengage ligament articular structures by adding a slight compressive force
Stabilize Inferior Vertebra; move Superior vertebra (the one messed up):
Flexion: Move spinous process superiorly
Extension: Move spinous process inferiorly
Rotattion: (spine to right = left rotation)
BLT time
What is the structural relationships of the AL5 counterstrain point
The obturator nerve (L2-4) courses anterior of the transverse processes of L3-L5 and pierces through the iliopsoas muscle. The posterior nerve bundle eventually pierces through the obturator externus muscle.
This nerve can become compressed in this muscle and generate altered sensation to the pubic region via the cutaneous branch, a condition termed obturator syndrome.
Describe how to do Counter Strain
Anterior L1:
Medial to ASIS
Flexion to spinal level + Pelvis + ankles rotate towards (to sidebend towards)
This rotates Spinal Level AWAY
Anterior L2-4:
L2 = Medial to AIIS
L3 = Lateral
L4 = Inferior
Flexion to spinal level + pelvis + ankles rotates away (sidebends away)
This rotates spinal level TOWARDS
Anterior L5:
Ant surface just below superior pubic rami
Flex to spinal level + Pelvis Rotates Towards + Ankles Rotates Away (sidebends away)
This rotates spinal level AWAY
Posterior L1-5:
Inf. Lat side of spinous process
Extension to spinal level by lifting thigh or pelvis
Rotates pelvis towards point and spinal level away
Upper Pole:
Superior Medial of PSIS
Extension + adduction w/ fine tuning of int/ext rotation of hip
Lower Pole:
2 cm below PSIS
Hip flexion + adduction + int. rotation
[REVIEW] Rule of 3’s
T1-3 + 12:
Spine and transverse = same level
T4-6 +11:
Spine = ½ below transverse
T7-9 +10:
Spine = 1 below Transverse