Vestibular Anatomy, Physiology and Disorders (Pineda, 04/2026)
1/95
Earn XP
Description and Tags
Content directly from lecture slides and in-person instruction
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
96 Terms
(Concept) Role of the Vestibular System
A sensory system with motor implications, incorporating head movements and head position against gravity beyond what proprioception alone can provide to help us discern self motion from environment motion
(Concept) 3 sensory afferents for balance (The Triangle)
Vision
Vestibular
Proprioception
(Concept) Input and output of balance afferents
Inputs to: Cortex, Brainstem, Cerebellum, Spinal Cord
Output: motor adjustments
(Concept) Sensory Redundancy
Allows for the loss of function in one of the sensory afferents. The other two afferent systems compensate; e.g. limitations to proprioception in diabetic patients with neuropathy leads to increased reliance on the vestibular and visual afferents
(Concept) In different situations (e.g. head is in the same position but the body is not), the balance response is (the same)/(different)?
Different; sensory afferents each react differently depending on the situation
(Anatomy) The vestibular system is about the size of our _____
thumbnail
(Anatomy) Input to the vestibular system comes from the _____, which is followed by the _____, or CN VIII
vestibular apparatus; vestibular nerve
(Anatomy) CN VIII synapses on the ____, cerebellum, and _____
brainstem; cortex
(Anatomy) Outputs of the vestibular system include (5):
oculomotor, cervical spine, body, conscious perception, and autonomic response
(Anatomy) CN VIII synapses at the _____ junction, then synapses to the _____ nuclei and feeds information into the cerebellum and the cortex
pontomedullary; vestibular
(Anatomy) The End Sensory Organs of the Vestibular Apparatus/Labyrinth are comprised of the _____ organs and the _____ canals
otolith; semi-circular
(Anatomy) The Vestibular Apparatus/Labyrinth is embedded in the _____ bone, and is part of the _____ ear
temporal; inner
(Anatomy) The Vestibular Apparatus/Labyrinth has a bony exterior with a _____ inner labyrinth lining
membranous
(Anatomy) The _____ cells within the labyrinth have nerve endings that, when _____ transmit signals to communicate positional or movement changes
hair; deflected
(Anatomy) Within the outer bony lining is _____ fluid, with higher concentrations of _____
perilymph; Na+
(Anatomy) In the inner membranous labyrinth (including the canals) is _____ fluid, with a higher concentration of ____ instead of Na+ to _____ nerve conduction.
endolymph; K+; promote
(Anatomy) Hair cells are found within the fluid-filled _____ (which sit atop the crista (crista ampullaris) of the ampullae in each semi-circular canal) and in the _____ (of the otoliths)
cupula; macula
(Anatomy) The otolith organs consist of the _____ and _____, which contain maculae (sg. macula)
utricle; saccule
(Anatomy) Within maculae are the otolithic membranes that has a jelly-like consistency. Hair cells, or _____, are imbedded within the _____ membranes of the maculae and _____ (made up of calcium carbonate crystals) are free to move about within the otolithic membrane, responding to both positional and gravitational influence
stereocilia; basement; otoconia
(Anatomy) The otolith organs are responsible for detecting _____ acceleration/deceleration. The utricle and saccule lie _____ relative to each other
linear; perpendicular
(Anatomy) The utricle detects acceleration in the _____ orientation and the saccule detects acceleration in the _____ orientation.
horizontal; vertical
(Anatomy) The otolith organs are sensitive to changes in position because of their relationship to _____. In response to _____, the calcium carbonate crystals weigh down the gel membrane and deflect hair cells
gravity; movement
(Anatomy) The Vestibular Labyrinth includes the three _____ canals, each corresponding to a different direction. They provide information based on _____ or angular acceleration.
semi-circular; rotational
(Anatomy) One of each canal is oriented to the _____, _____ (superior), and _____ (lateral) planes.
posterior; anterior; horizontal
(Anatomy) To test the lateral canal, orient the head 20º _____. Each canal is oriented at _____ relative to each other
down; 90º
(Anatomy) To achieve bilateral symmetry, the canals work in pairs. The left and right _____ canals work together while the _____ posterior and anterior canals work together.
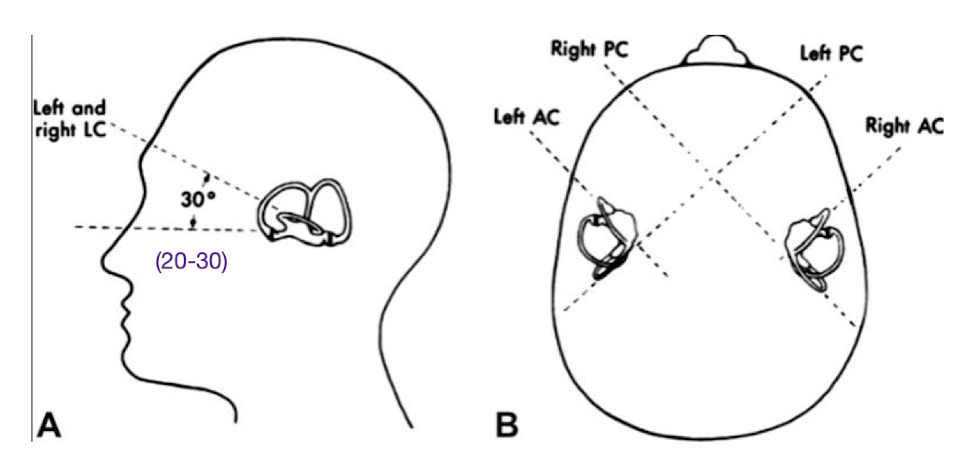
horizontal; contralateral
(Anatomy) The fluid within these canals moves (in the same)/(opposite to the) direction of the head because of inertia. Deflection of the hair cells can either be excitatory or inhibitory, depending on _____.
opposite; direction
(Anatomy) The canals (are)/(are not) continuous circle, hence “semi-circular.” They are interrupted by the _____
are not; ampulla
(Concept) Push-Pull Relationship: Head motion creates excitation on one side and inhibition on the other side. The brain interprets this firing _____ between sides as head movement; this process creates sensory _____.
asymmetry; redundancy
(Concept) Vestibular Dysfunction: Pathology can create changes in firing rates even without head movement; when these create _____ in firing rates they can create a sensation of _____ even without any movement. This stimulates the _____, causing reflexive eye movement and nystagmus
asymmetry; head-spinning; VOR (vestibulo-ocular reflex)
(Concept) The vestibular nerve’s signal travels from the hair cells deflected within the semi-circular canals or maculae –> vestibular ganglion (“_____ Ganglion”; cell body = bipolar neuron) –> vestibular branch _____ nerve (CN VIII)
Scarpa’s; vestibulocochlear
(Concept) The vestibular pathway begins at the vestibular branch of vestibulocochlear nerve, the enters the _____ at the pontomedullary junction before splitting off to reach the _____ nucleus and the _____
brainstem; vestibular; cerebellum
(Concept) There are 4 vestibular nuclei on each side of the caudal pons and rostral medulla. They then synapse onto second order neurons, to reach the medial _____ fasciculus, medial _____ tract, _____ vestibulospinal tract, and finally the _____ before reaching the vestibular cortex
longitudinal; vestibulospinal; lateral; thalamus
(Concept) The medial longitudinal fasciculus ascends to nuclei for CNs _____, _____, and _____ before reaching the superior _____
III; IV; VI; colliculus
(Concept) The medial vestibulospinal tract (and medial longitudinal fasciculus) connect to CN _____ and the _____ and _____ regions of the spinal cord
XI; cervical; upper thoracic
(Concept) The lateral vestibulospinal tract then descends into the _____ to provide control over _____ posture against _____
spinal cord; upright; gravity
(Concept) Following the thalamus the vestibular pathway synapses again at the vestibular _____ to facilitate cognition of _____ orientation, spatial _____, and _____ of self-motion
cortex; spacial; memory; perception
(Concept) The medial longitudinal fasciculus is a _____, highly specialized and heavily _____ nerve bundle responsible for extraocular muscle movements. These include the _____ reflex, _____ eye movements in smooth pursuit, and the vestibulo-ocular reflex (VOR)
paired; myelinated; oculomotor; saccadic
(Concept) The goal of the extraocular muscles is to coordinate eye movement based on _____ movement. The medial longitudinal fasciculus ascends bilaterally to synapse on the nuclei of CNs III, IV, and VI. These synapse onto third order _____ neurons
head; motor
(Concept) The third order motor neurons following CNs III, IV, and VI are in order the medial _____, the superior _____, and the _____ rectus as well as the contralateral CN III nucleus
rectus; oblique; lateral
(Concept) The vestibulothalamocortical pathway is _____; it follows from the vestibular nucleus into the ventral posterior nucleus of the thalamus before finally reaching the vestibular cortex. This provides conscious _____ of head position and movement while providing input into the _____ tract to influence _____ movement in response to head movement and balance changes
bilateral; awareness; corticospinal; voluntary
(Concept) The reflexes are the vestibulo-_____ reflex (head-righting), the vestibulo-_____ (balance and upright posture), and the vestibulo-ocular reflex (VOR; provides gaze _____ when the head is moved quickly)
colic; spinal; stability
(Concept) The vestibulo-ocular reflex (VOR) is triggered when maintaining the eyes on a target ahead, with a _____ ratio for head movement in one direction to eye movement in the _____ direction. For example, if the head moves 15º right, the eyes move 15º left to keep the object in _____. This is the result of input to CNs III and VI from the vestibular nucleus
1:1; opposite; focus
(Concept) The vestibuloreticular pathway sends information to the _____ formation (in charge of sleep/wake, habituation, pain modulation, and muscle activity). This includes _____ responses like nausea and vomiting; in the case of a brain _____ it contributes to an altered consciousness. This pathway influences the _____ tract (spinal reflex arcs and muscle tone in standing/walking)
reticular; autonomic; injury; reticulospinal
(Concept) The goal of the vestibulocerebellar pathway is to influence coordination of _____ muscles, head movement, and impacts the magnitude of _____ movements (in the body, head, and eyes). The vestibular nerve is routed to the _____ nucleus which sends output to: the vestibular nucleus into the medial and lateral vestibulospinal tracts, the spinal cord via the medial corticospinal tract, and the reticular formation via the medial reticulospinal tract
postural; reflexive; fastigial
(Concept) In summary, the vestibular pathway follows this:
vestibular apparatus
vestibular nerve
cerebellar and vestibular nuclei
cerebellar output to fastigial nucleus, then vestibular nucleus
vestibular nucleus (5 outputs)
reticular formation
medial longitudinal fasciculus (ascend to CNs III, IV, VI for eye movements)
medial vestibulospinal tract (in the descending medial longitudinal fasciculus for head/neck equilibrium)
lateral vestibulospinal tract (spinal cord)
and finally, the cortex (conscious pathways)
(Concept) Vestibular signs/symptoms can occur with injury/lesion to any of the following:
vestibular _____
vestibular _____
pons/medulla at the level of the _____
disruption of the medial longitudinal fasciculus
disruption of the lateral vestibulospinal tract
_____
apparatus; nerve; nuclei; cerebellum
(Concept) Vestibular signs/symptoms include the following:
disequilibrium/_____
_____ of the trunk
_____ (repetitive jerk/fixation of the eyes)
_____ (subjective; conscious awareness of dizziness; may include sensations of spinning)
imbalance; ataxia; nystagmus; vertigo
(Concept) Vestibular nystagmus will always beat _____ the relatively more excited side. Direction is named for the _____ phase (from the _____’s perspective. _____ goggles can be used to remove visual fixation and help identify nystagmus
toward; fast; patient; Frenzel
(Concept) Peripheral vestibular disorders include benign _____ positional vertigo (BPPV), unilateral vestibular _____ (UVH, which can be due to a neuritis or a _____), and _____ vestibular hypofunction (BVH)
paroxysmal; hypofunction; labyrinthitis; bilateral
(Concept) BPPV is the _____ common peripheral vestibular disorder. It occurs when the otoconia are _____ from the utricle and enter one or more of the semicircular canals. Causes include _____, aging (fluid thickens/dries up), viral infection, vitamin D _____, and often can be idiopathic. Different timing/triggers can result in episodes of dizziness, often triggered by head position changes
most; dislodged; trauma; deficiency
(Concept) The timing of BPPV episodes can further classify the BPPV as _____ for episodes lasting less than 1 minute and _____ for episodes lasting longer than 1 minute. In the first, the otoconia are _____ in the canal, whereas in the second the otoconia are _____ to the cupula
canalithiasis; cupulolithiasis; free-floating; stuck
(Concept) To determine which canal is involved, perform either the _____ or _____ tests which check for posterior vs. anterior canal involvement
Dix-Hallpike; side-lying
(Concept) When in doubt, treat _____ canalithiasis (if they have very slight symptoms during Dix-Hallpike with slight or no nystagmus). This is the most common canalithiasis, with the least common being _____ canal cupulolithiasis. In Dix-Hallpike testing, _____-beating means the posterior canal is involved, whereas _____-beating means the anterior canal.
posterior; horizontal; up; down
(Concept) If you suspect one side, clear _____ first. This way it is less _____ and you can move straight into treatment after confirmation
opposite; aggravating
(Concept) Right posterior canal = _____ torsion and is _____-beating
right; up
(Concept) Left posterior canal = _____ torsion and is _____-beating
left; up
(Concept) Right anterior canal = _____ torsion (possibly brief or not observed) and is _____-beating
right; down
(Concept) Left anterior canal = _____ torsion (possibly brief or not observed) and is _____-beating
left; down
(Concept) True or False: In posterior canal BPPV, you should expect nystagmus.
True
(Test/Measure) BBQ/Horizontal Roll Test:
begin with the patient in _____
flex the head to _____
rotate the head opposite from suspected side (rule out) and hold for slightly over 1 minute. Return head to neutral and hold 1 minute before testing other side
_____ nystagmus occurs in canalithiasis and beats towards the ground, with the affected side having worse symptoms
_____ nystagmus occurs in cupulolithiasis and beats away from the ground, with the affected side having less symptoms
supine; 30º; geotropic; apogeotropic
(Test/Measure) Deep Head Hanging Maneuver:
following the _____/horizontal roll test, instruct patient to roll into _____
patient pushes up into their elbows (hips down) and maintains their head position _____, holding for 1 minute
assist patient into sitting, maintaining _____ until transition is completed
BBQ; prone; down; chin-tuck
(Concept) True or False: Posterior BPPV cannot turn into horizontal BPPV based on head turns and canal anatomy.
False; it can
(Concept) True or False: With geotropic canalithiasis BPPV you treat the same side, whereas with apogeotropic cupulolithiasis BPPV you treat the opposite side.
True
(Concept) BPPV is named directionally by identifying the _____ side. So, with apogeotropic nystagmus lasting >1 minute that is less severe while laying on the right, we would call it _____ horizontal canal _____ BPPV
worse; left; cupulolithiasis
(Concept) True or False: Patients who have BPPV once are less likely to have it again at some point
False; more likely
(Concept) True or False: In the following 24 hours after BPPV treatment, patients may feel postural instability and should be careful to avoid large, triggering motions.
True
(Concept) Vestibular hypofunctions are a result of _____ of the vestibular nerve causing a _____ in signal transmission on that affected side. This impairs the _____ and is often due to a form of _____ infection
inflammation; decrease; VOR; viral(Concept)
(Concept) The viral infections that cause vestibular hypofunctions can be a _____, which is the most common. In cases of vestibular _____ it can impact _____. Unilateral vestibular hypofunction affects only one side
neuritis; labyrinthitis; hearing
(Concept) Key findings of vestibular hypofunction include an initial experience of “vestibular crisis,” defined by _____ nystagmus towards the _____ ear (e.g., R nystagmus = L unilateral vestibular hypofunction). Nystagmus will follow _____ Law
spontaneous; healthy; Alexander’s
(Concept) Alexander’s Law states that the amplitude of nystagmus _____ when the eye moves in the direction of the _____ phase (does not change direction), and that it _____ while looking in the _____ direction. Nystagmus is greater with fixation blocked (use Frenzel goggles!) and less with fixation
increases; fast; lessens; opposite
(Concept) Peripheral vs. Central nystagmus:
peripheral (follows)/(does not follow) Alexander’s Law
nystagmus is inhibited
mixed patterns of torsion with verticality (e.g. R/L with up/down-beating)
patients report feelings of _____
central may be _____
nystagmus may increase or not change
the patient _____ has a pure vertical or torsional
patients report no vertigo even with intense nystagmus
follows; vertigo; direction-changing; always
(Concept) Unilateral vestibular hypofunction timing (_____)
Their history of present illness (HPI) will include initial c/o spontaneous and constant _____ (can be spinning), usually with nausea/vomiting, unsteadiness, vision _____ especially with head movements (feelings of inability to leave bed; feeling like they are having a stroke). While the dizziness is usually present at rest and worsens with movement, they may _____ over a few days. With initial onset, patients may have felt a need to be seen in the _____; if they seek medical help they may be put on vestibular _____.
acute; dizziness; blurring; improve
(Concept) Unilateral vestibular hypofunction timing (_____)
Typically these patients will go to PT. They will have continued c/o _____ vision with head movements (feeling that things “_____” around). Patients often still have unsteadiness and feelings of motion _____
chronic; blurred; jump; sensitivity
(Concept) The vestibular exam includes looking for spontaneous and gaze-holding nystagmus; a few beats of gaze-holding nystagmus is _____. Typically these resolve within _____ days; afterwards we use further tests to show vestibular loss, including:
using Frenzel goggles
Head shake test (20x at 2Hz or greater, with goggles or eyes closed)
Head thrust/_____ test (HIT; if unable to maintain gaze with turning head to one direction, that side has a deficit)
VOR (cancellation phenomenon)
DVA (dynamic visual acuity)
_____ measures (mCTSIB, CTSIB, FGA)
normal; 7-10; impulse; balance
(Concept) Medical management of vestibular hypofunction includes _____, vestibular suppressants and anti-_____ acutely (not a lont-term solution). If your patient is on suppressants (most common = _____), findings will be altered as nystagmus is suppressed. Long-term use of suppressants interferes with recovery, and it is recommended that patients are off of their medication for at least _____ hrs before exam
corticosteroids; nausea; Meclazine; 48
(Concept) Bilateral vestibular hypofunction (BVH) results from inflammation or damage to both vestibular nerves. This is often due to a _____ cause, including _____. This can result from _____ including Gentamycin and Vancomycin, as well as receiving _____ for cancer
systemic; ototoxicity; drugs; chemotherapy
(Concept) CALM EAR mnemonic for ototoxic drugs:
C: Cisplatin and Carboplatin
A: _____ (Gentamycin and Tobramycin)
L: Loop diuretics
M: _____ drug (Quinine)
E: Erythromicin
A: _____
R: _____ Syndrome (Vancomycin)
Aminoglycoside; Malaria; Aspirin; Reman
(Concept) Bilateral vestibular hypofunction often has an _____ onset (but sometimes linked to medication use). Patients (have)/(do not have) complaints when still/seated if the bilateral loss is symmetrical. While _____ is a common complaint, most patients with BVH will complain of _____, or bouncy vision
insidious; do not have; unsteadiness; oscillopsia
(Concept) True or False: Patients with unilateral vestibular hypofunction (UVH) often refer to themselves as “Wobblers,” as they can have normal equilibrium with open eyes and slow movements. However, with rapid movement and/or closed eyes, equilibrium is lost and results in a characteristic “wobbly” gait.
False; bilateral, BVH
(Concept) For patients with bilateral vestibular hypofunction (BVH), you can expect _____ findings for nystagmus or spinning sensation (assuming they have a _____ hypofunction). The head thrust/impulse test (HIT) is positive _____, and patients present with a severe _____
negative; symmetrical; bilaterally; imbalance
(Concept) Following initial examination of a patient with a possible bilateral vestibular hypofunction (BVH), you can determine the cause and treat or decide on necessity of referral for _____ management. In terms of vestibular rehab, oscillopsia can be treated with with gaze _____ exercises and imbalance can be treated with _____ training, sensory _____, and safety education
pharmacological (or medication); stabilization; balance; substitution
(Concept) Central vestibular disorders result from dysfunction in the _____ that interferes with transmission, processing, and/or integration of vestibular input. This often comes from lesions within the _____ or the _____. Important: vertical nystagmus is _____ a central disorder (not BPPV)
central nervous system (CNS); brainstem; cerebellum; always
(Concept) True or False: In a tertiary interdisciplinary outpatient dizziness unit, central vestibular disorders, including vestibular migraine, comprise about 25% of the established diagnoses
True
(Concept) The 5 D’s of Central Vertigo:
_____ (speech difficulty)
_____ (double vision)
dysmetria (past moving; difficulty w/ movement)
_____ (difficulty with rapid, alternating movements)
_____ (difficulty swallowing)
dysarthria; diplopia; dysdiadochokinesia; dysphagia
(Concept) Possible causes of central vestibular disorders include stroke (CVA), multiple sclerosis (MS), _____ brain injury (TBI), transient _____ attacks (TIA), cerebellar degeneration, _____, and vestibular migraines. Another disorder that may be tied to stroke and/or other lesions resulting in central vestibular disorder is known as _____ syndrome, in which patients lose their orientation to pure vertical and believe they are upright
traumatic; ischemic; concussions; Pusher
(Concept) The vestibular exam for central disorders finds _____ nystagmus (especially down-beating or pure torsional), _____ nystagmus (that does not follow Alexander’s Law), impaired ocular motility (CN deficits), impaired smooth pursuits (jerky eye movements and/or saccadic intrusions), impaired saccades (hyper- or hypometric), and complaints of motion sensitivity, imbalance, and gaze _____. If the PMHx does not account for any of these findings, you MUST _____ as this may be urgent
spontaneous; direction-changing; instability; refer
(Concept) In the case of a central vestibular disorder finding, you must refer to the proper physician; the most appropriate physician referral would be an _____, nose and throat specialist, or ENT. They are vestibular specialists and can confirm your findings with special vestibular testing. Another appropriate referral would be a _____.
ear; neurologist
(Concept) Vestibular migraines are a growing diagnosis within the last few decades, and can respond to regular, preventative treatment for migraines. Diagnosis is marked by a migraine w/ or w/o auras and vestibular symptoms intense enough to interefere with or prevent _____, lasting between 5min to _____ hrs. These are linked with other pain, inflammatory, autonomic and connective tissue _____. Patients may not even complain about a headache, and some may even present with gait _____
I/ADLs; 72; comorbidities; ataxia
(Concept) True or False: Vestibular migraines can be misdiagnosed as functional neurologic disorder (FND), which has different triggers including stress. Martin Luther is an example, who recorded and described having vertiginous symptoms that were triggered by stressful situations.
True
(Concept) “AMIGUITAS” mnemonic for populations that may be more _____ to vestibular migraines:
A: _____ problems (POTS, orthostatic hypotension, unexplained syncopes)
B: migraine associated symptoms (photo/phono/osmophobia, allodynia)
I: _____ (asthma, rhinitis, thyroid disease, allergies)
G: gastro-intestinal (GERD, gastritis, hiatus hernia, IBS, intestinal inflammatory disease)
U: uterine problems (endometriosis, polyps, myomas, hysterectomy)
I: incontinence (hyperactive bladders, frequent cystitis)
T: tissue (hypermobility, EDS, RA, SLE, scleroderma, PMO/DMM, Sjorgen)
A: -_____ (fibromyalgia, chronic back/pelvic pain, joint pain, chest pain)
S: skin problems (urticaria, psoriasis, eczema, rashes, atopy, hives)
predisposed/susceptible; autonomic; inflammatory; algias
(Concept) Vestibular migraines present differently among patients, so it is important to confirm _____. Oftentimes a recent cold or _____ infection can precede bouts of _____, however with no coordination deficits. Migraine triggers can be work _____, with reports that “nothing is out of the ordinary”
timing; sinus; hypofunction; stress
(Concept) PTs are the _____ provider to treat vestibular migraines, and vestibular rehabilitation depends specifically on the Dx:
BPPV is treated with maneuvers based on the side, canal, and type of BPPV
Gaze instabilities are often _____ but induce adaptation
UVH is treated with adaptation gaze stability exercises
BVH is treated with substitution gaze stability exercises
Central is usually treated with substitution
Motion sensitivity is treated with _____ training
Unsteadiness is treated with balance training for specific _____, along with patient education for fall safety and assistive device use
primary; uncomfortable; habituation; impairments
(Concept) The HINTS exam is used to distinguish between vertigo and a life-threatening diagnosis and is a rapid bedside exam with _____ specificity within the first 24-48 hours, able to rule-out a stroke better than a negative _____ with diffusion weighted imaging (DWI). It was created to supplement traditional _____ scans which can _____ 60-90% of ischemia in the posterior fossa
high (96%); MRI; CT; miss
(Concept) The HINTS exam is comprised of:
Head Impulse test
peripheral vertigo = abnormal (positive) test
central = normal (negative) test
reassuring finding = abnormal (corrective _____)
_____
peripheral vertigo = unidirectional, horizontal nystamus
central = rotary or vertical nystagmus, or direction-changing horizontal nystagmus (+ Alexander’s Law)
reassuring finding = unidirectional, horizontal
Test of _____
peripheral = no skew deviation
central = may have skew deviation from alternate eye cover testing
reassuring finding = no skew deviation
Overall, reassuring findings support _____ vertigo.
saccades; Nystagmus; Skew; peripheral
(Concept) Overall, vestibular rehabilitation is dynamic and emerging, and PTs should stay on top of updated _____ if you are treating vestibular patients consistently. The Academy of Neurologic Physical Therapy (ANPT) is a great resource, with a vestibular _____ (SIG), various provider and patient education handouts, podcasts and other resources
evidence; special interest group