15- Procedures for Delivery
1/23
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
24 Terms
When do you make the remount casts?
After you finish and polish the bases, prior to the delivery appointment. The natural teeth must be represented on an RPD remount cast in order to adjust the occlusion
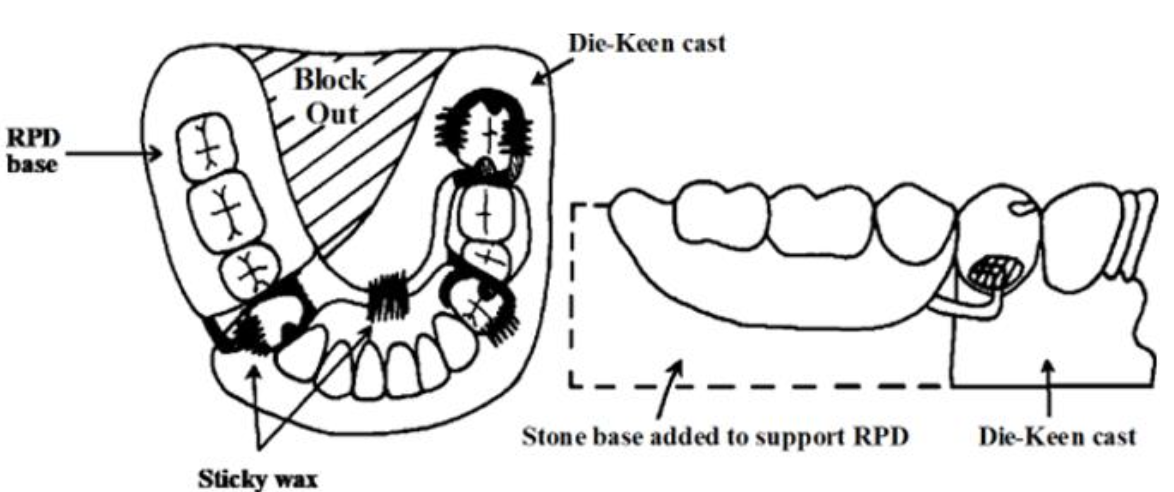
Why would you remove the free-end/distal extension area in a remount cast
Soft tissues cannot be duplicated accurately enough to assure proper seating of the denture on the remount cast
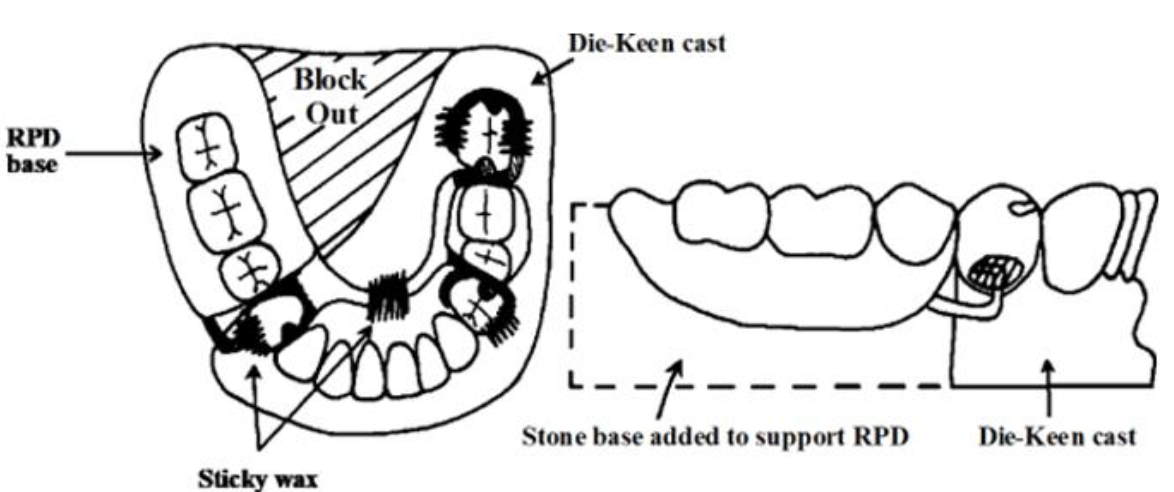
What should actually touch the remount cast?
Only the metal framework should touch the cast, and only on the abutment teeth
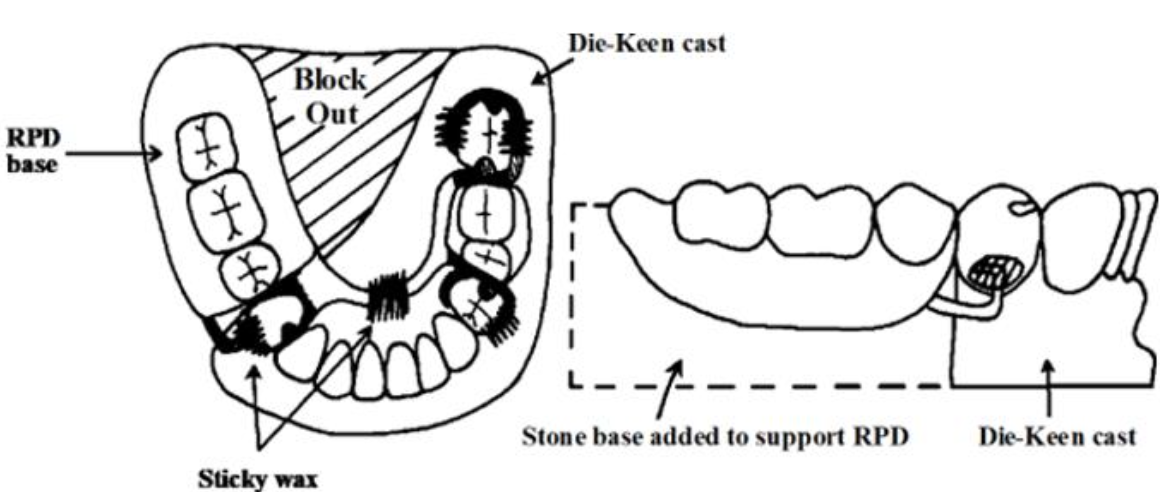
What should you use to secure the framework to the cast and block out undercuts in the base.
Sticky wax
Why is the distal extension ridge removed but white stone added beneath the RPD base?
The denture base still needs support during remounting and occlusal adjustment. Unite it to the Type IV stone cast
If you forgot to make an alginate impression of the natural teeth at the wax try-in, what are some steps you should take?
Use PIP to make sure the RPD fits properly
Use an oversized rimlock tray to make an alginate impression over the RPD, seating in the mouth
Remove impression with RPD still in impression
Remove excess moisture and block out undercuts
Pour with fast-set stone
Recover cast in 5-10 min, trim, and proceed with jaw relation record
What kinds of irregularities are you checking for
Little defects like sharp acrylic, bubbles, resin nodules, and resin flash. These can hurt the patient or prevent seating
What is the point of using PIP?
Put PIP inside denture
Seat denture
Look where paste is rubbed away
Adjust slightly
Repeat
What should you check for when evaluating border extensions?
Are the flanges too long or too short? The buccal flanges should reach the depth of the vestible to prevent food collection. The lingual flange coverage needs to be adequate, it can be shorter and thinner than complete denturesI
Is border seal required?
Usually no since most lateral stability comes from the teeth. The patient should not have the annoyance of large lingual flanges unless few teeth remain and maximum direct retention of the base is required
What are some reasons why the metal framework would not seat properly?
Resin flash inside a clasp assembly, framework was incompletely seated during altered cast impression, framework inadvertently was lifted away from master cast during final wax-up
In most NAT/RPD cases, how is occlusion adjusted?
Intraorally. Dry the mouth and use articulating paper. Prematurities may cause a distal extension RPD to shift and give false markings
In all CD/RPD cases, how is occlusion adjusted?
It must be remounted, regardless of class of RPD. Attach the Aluwax to maxillary denture or the /RPD if it has long bases on both sides. The teeth should lack contact by 1-2mm at the completion of wax record
What is the first step in occlusal adjustment of CD/RPD?
Centric occlusion. Use red articulating paper to mark the prematurities (usually the one that has an unmarked center: “eye.”
Why do you reduce the fossa and not the cusp?
Because grinding away cusps destroys anatomy and balance
What is the anterior contact for a CD/RPD case?
No contact between upper artificial anterior teeth and lower natural anterior teeth in centric in order to help preserve the premaxilla, they should contact in eccentric
After checking centric occlusion, check eccentric occlusion. How is the working side adjusted?
Using the BULL rule: Inner inclines of buccal upper and lingual lower cusps
When instructing patients on insertion and removal, what are some important guidelines when demonstrating?
Never seat the RPD by biting it into place because it can cause needless clasp adjustment and repair. They should seat it by hand
Some soreness is expected. When are postinsertion visits to check how the pt is adjusting to the denture?
3,7,14 days and 6 weeks. Advise the pt to attempt only easy-to-chew foods
What are some ways the patient can overcome any speech problems caused by the RPD?
Reading aloud to train the tongue and other oral structures to regain acceptable speech. Crowding of the tongue and gagging are rarely a problem with properly contoured border extensions
If a patient fails to maintain plaque control, what can happen?
The longevity of the appliance is directly related to the level of home care. Daily application of stannous fluoride can help to prevent caries
Why should an RPD not be left out for several days?
Tooth movement may occur, but it is recommended to just take it out at night.
Why should you not use Calgon-Clorox to clean dentures?
It can corrode the metal. Fixodent works best
It is important that the patient return once a year for a check up. Data collection showed that caries occured within two years of denture placement. How often do distal extension RPDs need a reline
By 3 years, if not sooner