USMLE: Nephrology
1/254
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
255 Terms
CREST stands for?
Calcinosis
Raynauds
Esophageal dysmotiltiy
Sclerodactyly
Talangiectasias
What does the kidney start off as? (Renal embryology)
Pronephros
—disappears by week 4
Mesonephros
—fetal kidney during 1st trimester
—becomes part of male genital system
Metanephros
—becomes adult kidney
What renal embryology structure becomes adult kidney?
Metanephros
What embryologic structure gives rise to entire collecting system?
Ureteric buds
—induces Metanephros to differentiate into renal tubular structures
Without ureteric buds, you would get?
NO kidneys at all (bilateral renal agenesis)
—because stimulates Metanephros to become renal Tubular epithelium
What is Potter sequence?
Bilateral renal agenesis (kidneys do not form)
"POTTER" mneumonic
Pulmonary hypoplasia
Oligohydramnios
Twisted skin
Twisted face
Extremities
Renal agenesis
Horshoe kidney is?
When inferior parts of kidneys fuse to form one kidney, and as it ascends during development, will get hung up under inferior mesenteric a.
What artery traps Horshoe kidney?
Inferior mesentaric
What disorder is associated with Horeshoe kidney?
Turners
Blood flows into kidney through?
Renal a
Peripheral part of kidney?
Cortex (where glomeruli found)
What brings blood into glomeruli?
Afferent arteriole
Blood brain barrier layers?
Capillary endothelium
Basement membrane
Astrocyte foot processes
Glomerular filtration barrier layers? (Tufts of caps in glomeruli)
Capillary endothelium
—fenestrated
Basement membrane
—negatively charged to keep proteins from leaving caps
Podocyte foot processes
What is tufts of capillaries in glomeruli covered by?
Bowmans capsule
What is path of blood through glomeruli starting with afferent arteriole?
Afferent —> goes to glomerular capillaries (within Bowman's capsule) —> plasma, electrolytes, aa, glucose (protein CANT) ooze through caps and ends up in Bowmans space —> now called filtrate which goes to proximal convoluted tubule after this
What cant diffuse through glomerular capillaries?
Protein
RBC
Platelets
—exits through efferent arteriole
Where are juxtaglomerular cells located?
Afferent arteriole within the Juxtaglomerular apparatus (along with Macula densa)
What does the macula densa do?
Senses sodium in the distal convoluted tubule (which is touching afferent arteriole)
—if sodium gets too low, tells Juxtaglomerular cells to secrete renin
What stimulates JG to release renin?
Sympathetics (B adrenergic stim)
Low Sodium in Distal convoluting tubule (Macula densa)
Low pressure in afferent arteriole
What is the difference between cortical and juxtaglomerular nephrons?
Cortical
—start higher up in cortex, only a small portion of loop of henle dips into medulla
—NO vasa recta
Juxtagolmerular
—start LOW in cortex, and loop on henle penetrates deep into medulla
—also have vasa recta that wrap around loop of henle (supply nutrients to medulla and provide osmotic gradient)
Nephrons drain into?
Collecting tubules —> minor calyces —> (2 or 3 minors converge) major calyces —> Renal pelvis —> Ureters
What is the renal pyramid?
Within renal medulla composed of both nephrons and collect duct
—base toward cortex, apex (papilla) directed toward minor calyces (which it dumps into)
Where do the ureters join bladder? What is important to know of this location?
Ureterovesicular Junction (UVJ)
—common place for kidney stones to get stuck
Ureter pass under?
"Water (urine) under the bridge"
Women
—under uterine artery
Men
—under vas deferens
Intracellular fluid comprises?
28 L
Extracelluar fluid comprises?
14 L
10.5 — interstitial
3.5 — plasma
What percentage are people water?
60%
2/3 of such is Intracellular (40% of body weight)
1/3 extracellular
Where are the two places renal blood flow can go to?
Glomerulus
Renal tubules
If a substance has a clearance greater than GFR, what does this mean?
Some of substance in the blood is also being secreted by the tubules
Clearance?
"UV over P"
(Urine concentration of a particular substance) x (urine flow rate) / plasma concentration
measures in volume over time (mL/min)
Which substance is freely filtered by glomeruli, and its clearance as a result = that of GFR?
Inulin
—not secreted OR reabsorbed by renal tubules
GFR normal range?
90-120 ml/min (think 100)
If a substance has a clearance less than GFR, what does this mean?
Some of substance in blood is being reabsorbed by tubules
Creatinine is?
Product of the breakdown of creatine in muscles
—found in plasma naturally
freely filtered
—not reabsorbed
—only time amount is secreted by tubules
What is used to estimate GFR?
Creatine clearance
—because found naturally in blood and freely filtered, not reabsorbed, and only TINY amount secreted form tubules
Filtration fraction?
Portion of blood going to kidney that is filtered through glomerulus
FF = GFR/RPF
—normally 20%
How is renal plasma flow different than GFR?
Renal plasma flow takes in blood to glomeruli AND blood to tubules
What do we use to estimate renal plasma flow?
PAH
—all of PAH that makes it to kidney will end up in urine and be excreted
T/F All the blood that goes to kidneys is filtered by glomerulus.
F; some of it goes to renal tubules
What is NSAIDs effect on filtration fraction?
Constrict afferent arteriole
RBF down
GFR down
FF no net change
What is Angiotensin II effect on filtration fraction?
RBF down
GFR up
—bc back flow into caps and more blood is then going through glomeruli filtration barrier
FF goes up
Pathway of blood from renal aa to renal vein?
Renal artery —> afferent arterioles —> glomeruli capillaries (from here can squeeze through and become filtrate or continue on) —> efferent arterioles —> renal tubules (wrap around nephron) —> renal vein
What is ACE inhibitors effect on filtration fraction?
Dilate efferent arterioles
—so RBF goes up
FF goes down
If you have ureter stone obstruction or increase in serum protein, effect on filtration fraction?
GFR
—down
RBF
—stay same
FF
—DOWN
Reabsorbed equation?
Filtered - excreted
Hartnup disease?
Defiency in aa transporter for NEUTRAL aa's (tryptophan)
—unable to make niacin, and get pellagra as result
Excretion rate =
Urine concentration x urine flow rate
How are glucose and aa cleared?
Freely filtered in glomeruli SO HAVE to be reabsorbed by renal tubules
—Na glucose co transporter in Proximal Tubules that allows for glucose reuptake
—Na dependent transporters in PCT that allows for aa reuptake
Where does most reabsorption in nephron?
Proximal tubule
What is the limit to where nephron can reabsorb glucose in proximal convoluted tubule?
Plasma glucose over 160
—exceeds body's capacity to reabsorb and glucose is LOST in urine
For aa reabsorption in nephron, what allows this?
Na dependent transporters in PCTs
For:
—positve
—negative
—neutral
What does the proximal tubule do?
Glucose and aa reabsorbed
2/3 of fluid and electrolytes are reabsorbed
Fluid is reabsorbed isotonically
—electrolytes reabsorbed and water follows
How does glucose and amino acids specifically get reabsorbed into interstitial?
Sodium co transported —> which brings into tubule
Then Na/K pump uses ATP to drive either glucose or aa out into interstitium
What is primarily being reabsorbed in FIRST half proximal tubule?
Bicarb
Sodium
How is bicarb reabsorbed in FIRST half of proximal tubule?
Use of carbonic anhydrase within lumen AND within the proximal tubule cell
—H+ goes back into lumen
—Bicarb goes to interstitium
How is sodium and chloride being reabsorbed in proximal tubule?
By Na/K pump
What things are reabsorbed faster than water? (NOT ISOTONIC)
Phosphate
Amino acids
Glucose
—sodium and potassium are isotonic because water is reabsorbed with them at about same rate
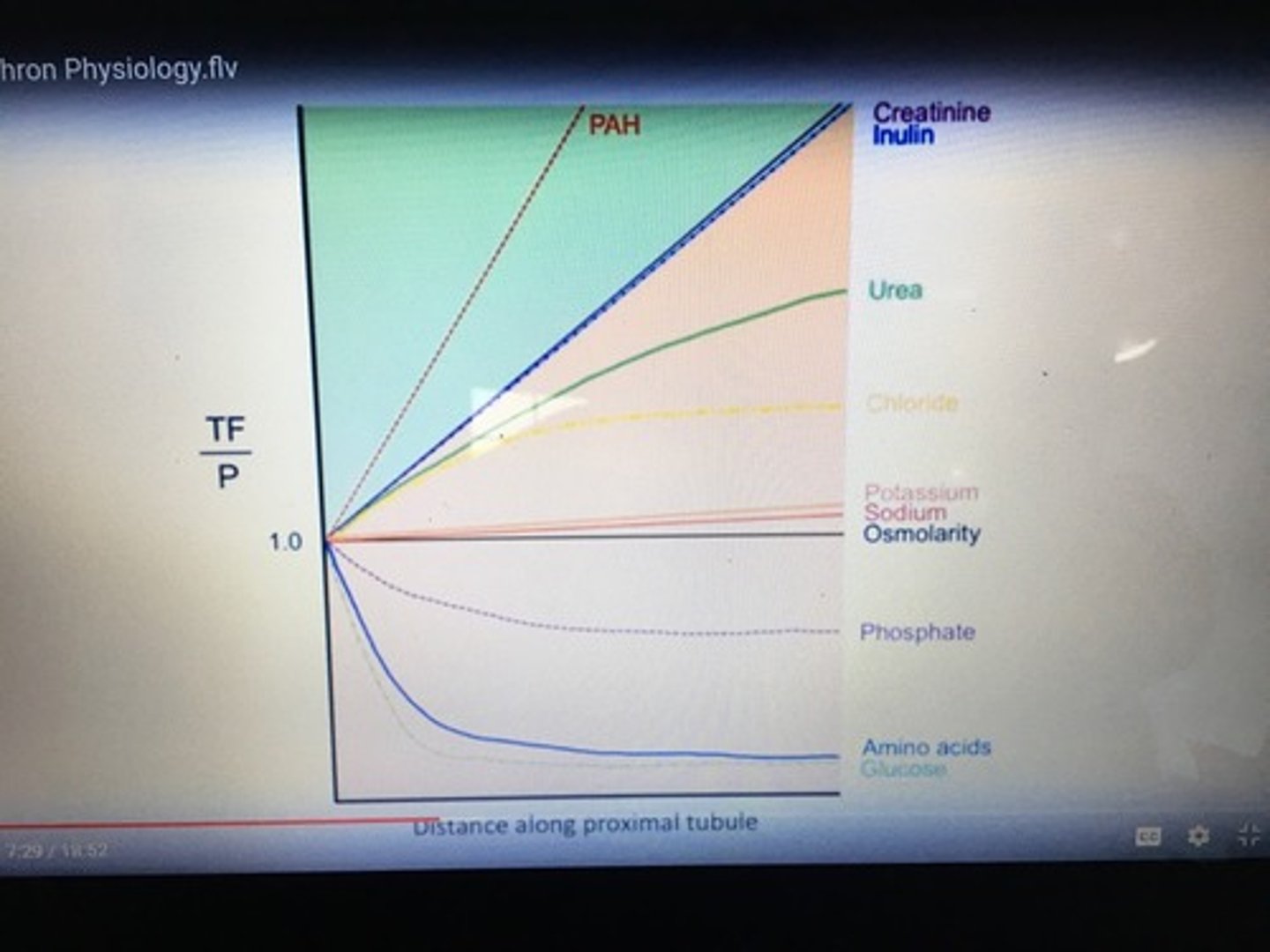
Need to know this graph
PAH is so high up because it is being filtered and secreted, so increasing relative to plasma because water is being reabsorbed while it stays the same in tubular fluid (so tubular fluid high/plasma low)
Phosphate and AA/glucose are below because they are being reabsorbed faster than water into plasma, so concentration of them in tubular fluid is decreased as go on (why it is so low)
In 1st half of proximal tubule, sodium reabsorption associated with? What about 2nd half?
1st half
—bicarb
2nd half
—cloride
Thick ascending limb responsible for?
Na/2Cl/K symporter
—ACTIVELY reabsorbing sodium, potassium and chloride (was more passive in proximal tubule)
Impermeable to water
Calcium and Magnesium reabsorption
Pathway of Glomeruli to Collecting tubules?
Glomeruli —> PCT —> Loop of Henle (thin descending limb and then thick ascending limb) —> DCT —> Collecting tubules
Thin descending limb responsible for? How?
Water reabsorption
—impermeable to sodium
Interstitum is hypertonic so has water pass because of osmotic gradient
What Inhibits the Na/2Cl/K symporter in the thick ascending limb?
LOOP diuretics
Thin descending and Thick ascending limb effects on urine?
Thin descending
—concentrating bc only permeable to water (NOT sodium)
Thick ascending
—diluting bc NOT permeable to water but sucking up ions (sodium, chloride, potassium)
In early part of Distal tubule, what is going on?
Active reabsorption of sodium and cloride
NOT always impermeable to water
**Calcium reabsorption is under control of PTH**
What types of cells compose the collecting duct and the last segment of DCT? What do they do?
Principal cells (most of collecting tubule)
—reabsorb water and sodium
—secrete potassium
Intercalated cells (types Alpha and Beta)
—secrete either H+ (alpha) and bicarb (beta)
—reabsorb potassium
How does PTH cause increase in serum calcium?
Stimulates bone resorp
Stimulates kidneys to activate Vitamin D
Stimulates kidneys to reabsorb more Calcium (at early DCT)
What determines how much water is reabsorbed in distal tubules and collecting ducts?
ADH (vasopressin)
DCT/collecting duct function?
Concentrate urine
—can be greatly affected by ADH
How does ADH cause reabsorption of water in DCT/collecting ducts?
Binds to V2 of Principal cell
—tells cells to insert aquaporins into luminal surface of cells
—these aquaporins allow water to be reabsorbed
What kind of potassium sparing diuretics are aldosterone antagonists?
Spironolactone
Eplerenone
What class of diuretics directly affects principal cells?
Potassium sparing diuretics
What kind of potassium sparing diuretics inhibit epithelial Na channels?
Triamterene
Amiloride
What is the effect of aldosterone on principle cells and intercalated cells of collecting duct?
Principle cells
—increases Na reabsorption, and secretes potassium
Intercalated
—stimulates secretion of H+ ions
Site of secretion of organic anions and cations?
Proximal tubule
What diuretic works at the PCT?
Acetazolamide
Mannitol
Permeable to water ONLY in the presence of ADH?
Late DCT and Collecting Duct
What are ADRs of Acetazolamide?
Sulfa drug
Metabolic acidosis
—losing bicarb
Acetazolamide MOA? Used for?
carbonic anhydrase inhibitor
—increases removal of water but more over bicarb in urine
Altitude sickness
—get rid of bicarb
Alkalinize urine
Chronic glaucoma
What draws aqueous humor into eye?
Bicarb
Mannitol MOA
Osmotic diuretic causing osmotic load that stays in filtrate and prevents reabsorption of free water in PCT
What are your sulfa LOOP diuretics?
Furosemide
Bumetanide
Torsemide
Ethacrynic acid
—NOT sulfa, would use if pt has sulfa allergy
What two diuretics can work for glaucoma?
Mannitol
—acute angle closure glaucoma
Acetazolamide
—chronic glaucoma
Loop diuretics MOA?
Inhibit Na/2CL/K symporter in thick ascending loop of henle
Thiazides are used for?
FIRST LINE for essential HTN
—not really for CHF (would use loop for this)
Loop diuretics vs Thiazides?
Loops lose calcium
Thiazides do NOT, and more commonly for HTN over loop
When do we use Loop diuretics?
When you want to get rid of water quickly
—CHF
—pulmonary edema
—nephrotic syndrome
—cirrhosis
Loop diuretics ADR?
Ototoxicity
Nephrotoxic
Hypokalemia
What are examples of your thiazide drugs?
Hydrochlorothiazide
—most commonly used
Chlorothiazide
Chlorthalidone
Metolazone
Thiazide MOA
Inhibit Na+/Cl- cotransporter therefore inhibiting Na+ reabsorption in the DCT
—retain CALCIUM (good if pt has osteoporosis with HTN)
Thiazides ADR?
Low potassium
Low sodium
High glucose
High lipids
High calcium
SULFER drugs
Someone with chronic CHF needs what 3 meds?
B blocker
ACE inhibitor (or ARB)
Aldosterone antagonist
T/F Thiazides are not sulfa drugs.
F; they are, so would not use with sulfa allergy
What are your potassium sparing diuretics?
"Potassium please have a SEAT" (cause you want to retain potassium)
Spironolactone
Eplerenone
Amiloride
Triamterene
—bold are aldosterone antagonists
For diuretics as a whole, what are ADRs? Name the exceptions
Increased urinary sodium and chloride
—except Acetazolamide
Increased urinary potassium
—except potassium sparing diuretics
Acidosis
—carbonic anhydrase inhibitors cause this
Alkalosis
—loops and thiazides cause this
Potassium sparing diuretics ADR?
High potassium
Gynecomastia
What produces 1,25 Dihydroxycholecalciferol (active Vitamin D)?
Enzyme 1a hydroxylase which is induced by PTH in the kidney
What hormones are produced from the kidney?
Renin
Vitamin D (1,25 Dihydroxycholecalciferol)
—by PTH
Erythropoietin
Prostaglandins
ANP by the atria in response to stretched walls, does what to increase water and sodium excretion?
Constricts efferent arterioles and dilates the afferent arterioles