Unit 3: Pulmonary System Pt 1
1/63
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
64 Terms
what is a healthy breaths per minute?
12-15 breaths per minute (approx 7 L of air)
what are the three 3 functions of respiration?
ventilation, gas exchange, and oxygen utilization/cellular respiration
what consists of external respiration?
ventilation and gas exchange in the lungs
what consists of internal respiration?
oxygen utilization and gas exchange in the tissues
describe the functions and characteristics of the conduction zone
1) warm and humidify, 2) distribute the air evenly 3) body’s defense system. has separate circulation: bronchial circulation, and no gas exchange. consists of the tracheal, bronchi, bronchioles, and terminal bronchioles. see much more cartilage in these structures compared to the respiratory zone
describe the respiratory zone
consists of the respiratory bronchiole, the alveolar duct, and the alveolar sac. here there is gas exchange via diffusion, have the alveoli, and a separate pulmonary circulation with an extensive capillary network
what are the highlights of the conduction zone?
filtration: mucus secreted by cells of the conducting zone traps small particles, and the mucus moves via mucociliary escalator to the pharynx, where is can be cleared by swallowing or expectorating (which is known as mucociliary clearance)
what might damage the mucociliary escalator?
smoking, since it can damage the cilia and reduce the mucociliary clearance
what is the pathway of air?
air travels down the nasal cavity to the pharynz, then to the larynx (via the glottis and the vocal cords), then to the trachea, to the right and left primary bronchi, to the secondary bronchi, to the tertiary bronchi, to the terminal bronchioles, then reach the respiratory zone and reaches the respiratory bronchioles, and final to the terminal alveolar sacs
describe the characteristics of the alveoli
are air sacs where the gas exchange occurs, around 300 million in the lungs, each is only 1 cell layer thick, and they form clusters at the ends of the respiratory bronchioles
what are the different types of alveolar cells?
type I where 95-97% of the gas exchange occurs, and type II which secrete pulmonary surfactant and reabsorb sodium and waters, preventing fluid buildup
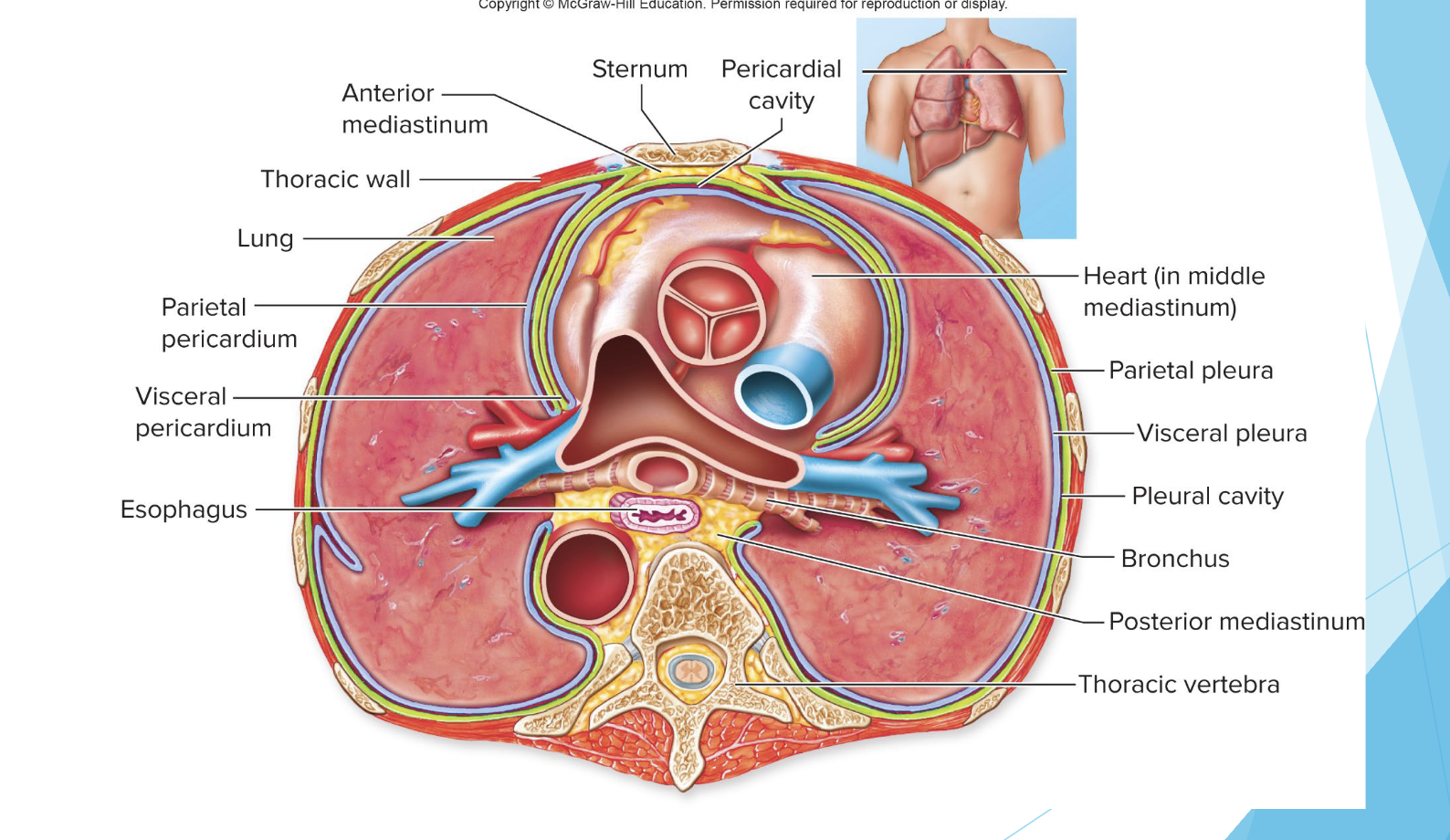
describe the bony anatomy of the pulmonary system
the thorax, the sternum, the ribs
what is the function of the thorax in the cardiopulmonary system?
covers and protects major organs of the cardiopulmonary system, provides skeletal framework for attachment of the muscles for ventilation
where would you ascultate to hear the apex of the lungs?
about an inch above the clavicle at the medial 1/3 of the clavicle
how many lobes are in the right versus the left lungs?
The right lung has three lobes (upper, middle, lower) while the left lung has two lobes (upper and lower) to accommodate the heart's position.
right lung is slightly shorter, why?
to accommodate the liver beneath it
what nerve supplies the diaphragm?
phrenic nerve
which landmark marks the level of bifurcation of the trachea into R and L stem bronchi?
the sternal angle (angle of Louis)
which are the true ribs?
ribs 1-7 since they atttach via their costal cartilages to the sternum
which are the false ribs and floating ribs ?
ribs 8-10 since attach to the ribs above their costal cartilages, and ribs 11-12 since they end freely respectively
what are the layers of the lungs?
the parietal pleura and the visceral pleura
what are the types of pressure involved in ventilation?
atmospheric pressure, intrapulmonary/intraalveolar pressure (pressure in the lungs), and intrapleural pressure (pressure within the intrapleural space)
describe the pressure differences during inspiration
the intrapulmonary pressure is lower than the atmospheric pressure (subatmospheric/negative pressure, about - 3 mmHg)
describe the pressure differences during expiration
intrapulmonary pressure is greater than atmospheric pressure (about +3 mmHg)
describe the intrapleural pressure
is the pressure within the pleural cavity, which is always lower/negative compared to atmospheric pressure and intrapulmonary pressure, helping to keep the lungs inflated. this keeps the lungs against the thoracic wall and allows the lungs to expand during inspiration. increasing thoracic volume further decreased the pleural pressure, which then leads to the lungs to expand and fill with air
what is transpulmonary pressure?
is the difference between intrapulmonary pressure and intrapleural pressure, indicating the amount of pressure available to expand the lungs. It is crucial for maintaining lung inflation during breathing.
what is boyle’s law?
states that the pressure of a gas is inversely proportional to its volume- an increase in lung volume during inspiration will decrease intrapulmonary pressure to sub-atmospheric levels, then air goes in. a decrease in lung volume during expiration increases the intrapulmonary pressure above atmospheric levels, and air goes out
describes the process of inspiration
inspiratory muscles contract, then the thoracic cavity expands, then the pleural pressure becomes more negative leading to increased transpulmonary pressure, then the lungs inflate, the alveolar pressure becomes sub-atomspheric, and then air flows into the lungs until alveolar pressure equals atmospheric
what is lung compliance/distensibility?
the ability of the lungs to expand, the change in lung volume per change in transpulmonary pressure (change in V/change in P). this also refers then to the ease with which the lungs expand/inflate/stretch under pressure, and is reduced by factors such as infiltration of connective tissue proteins in pulmonary fibrosis
what is the elasticity of the lungs?
the ability of the lungs to return to the initial size after being stretched- since the lungs are stuck to the thoracic wall they are always under elastic tension, and tension increases during inspiration and is reduced by elastic recoil during expansion
what interventions can be done for patients with COPD or emphysema in which the lungs stay partially inflated?
pursed lip breathing, other techniques to increase the intrathoraic pressure to help to force out the air in the lungs. also it may help for some patients to kind of lean forward or stand hunched to help them breathe
what is the surface tension of the lungs?
the force that resists distension/compliance of the lungs. is exerted by fluid secreted by the alveoli, and the fluid is absorbed by active transport of Na+ and secreted by active transport of Cl-, this raises the pressure of the alveolar air as it acts to collapse the alveolus
what is the law of the laplace?
says that pressure (P) = 2 x surface tension (2T) / radius. this means that the pressure is directly proportional to the surface tension and inversely proportional to the radius of the alveoli, small alveoli would be at a greater risk of collapse without surfactant
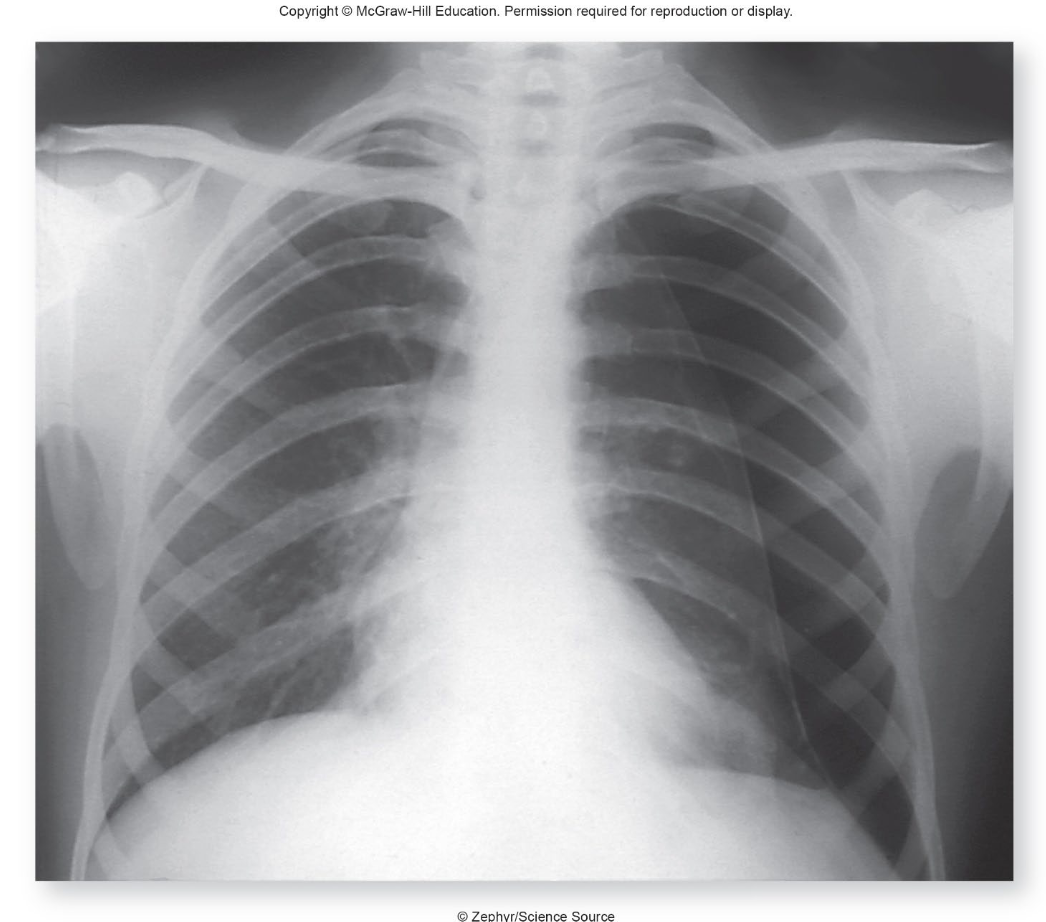
what is pneumothorax?
a condition where air enters the pleural space, leading to lung collapse due to pressure imbalance. It can be caused by trauma, disease, or spontaneously. when looking at imaging the collapsed side with be darker due to more air in the lungs
what produces the pulmonary surfactant?
Type II alveolar cells produce pulmonary surfactant, a substance that reduces surface tension in the lungs, helping to prevent alveolar collapse.
what are the muscles of inspiration?
diaphragm, external intercostals, scales, SCM, parasternal intercostals
what are the muscles of expiration?
(mostly of forced) internal intercostals, the abdominal muscles (transversus abdominis, rectus abdominis, external obliques, and internal obliques)
what does movement of air require?
airtight chest and respiratory muscles
how does the thorax change during inspiration?
the diaphragm contracts and pushes abdominal the contents downward, the ribs are pushed outward, and in forced inspiration the accessory muscles pull ribs change upward and outward
how does the thorax move with expiration?
the diaphragm relaxes and return to the dome shape, the rib cage lowers, and during force expiration the intercostals pull the rib cage downward and inward and pull the rib change downward (compressing the thoracic volume)
how might positioning affect diaphragm motion?
posture determines the position of the diaphragm- kyphosis or lordosis can restrict movement. when supine the resting level of the diaphragm rises and the lung volumes are decrease. when sitting the dome is pulled down which allows for larger lung volume
what positioning would be helpful for patients with pulmonary disease?
Upright or semi-upright positions can enhance lung expansion and facilitate breathing. Positions such as sitting or leaning slightly forward may help to improve diaphragm function and oxygenation.
in a healthy person, how is the compliance of the apex of the lungs compared to the base?
it is less than that at the base due to gravity, gravity also causes lower pleural pressure at the apex than at the base (leading to greater transpulmonary pressure a the apex)
what is alveoli compliance like at the apex and base at low lung volumes?
alveoli compliance is greater at the apex versus the base
what are the pressures like in the lung during low lung volumes?
the pleural pressure at the base of the lungs exceeds the pressure inside the airways, leading to airway closure. ventilation at the base then is impossible until the pleural pressure falls below atmospheric pressure. the apex of the lung is more compliant therefore air enters the alveoli in the apex and is better ventilated that the base
what are some of the pulmonary function tests?
spirometry, and lung volume measurements, as well as lung capacity measurements
what is spirometry?
test that measures lung volumes and airflow during inhalation and exhalation, makes a volume-time curve, has multiple components, and can be used to diagnose restrictive and disruptive lung disorders
describe the lung volume measurements
include tidal volume (the amount of air expired/inspired in quiet breathing), expiratory reserve volume (amount of air that can be forced out after tidal volume), inspiratory reserve volume (amount or air that can be forced in after tidal volume), residual volume (amount of air left in lungs after maximum expiration)
what are lung capacity measurements
vital capacity (max amount of air that can be forefully exhaled after a max inhalation), total lung capacity (amount of gas in the lungs after maximum inspiration), inspiratory capacity (amount of gas that can be inspired after a normal expiration), functional residual capacity (amount of gas left in lungs after a normal expiration)
what is the relationship between vital capacity and lung volumes?
vital capacity = inspiratory reserve volume + expiratory reserve volume + tidal volume
what is the relationship of functional residual capacity and lung volumes?
Functional residual capacity = expiratory reserve volume + residual volume.
what is total minute volume?
total minute volume = tidal volume x breaths per minute (approx 6L/min)
definition of lung volumes
the four nonoverlapping components of the total lung capacity
definition of lung capacities
measurements that are a sum of two or more lung volumes
what are restrictive disorders?
lung tissues is damaged, vital capacity is reduced, but forced expiration is normal (inspiration is affected). Ex: pulmonary fibrosis and emphysema
what are obstructive disorders?
lung tissue is normal. vital capacity is normal but forced expiration is reduced (inspiration is normal). ex: asthma and chronic obstructive pulmonary disease (COPD).
describe asthma
one of most common obstructive disorders. caused by inflammation, mucus secretion, constriction of bronchioles. aka airway hyperresponsiveness. Allergic asthsma is triggered by allergens stimulating T lymphocytes to secrete cytokines and recruit eosinophils and mast cells, which contribute to inflammation. Additionally, can be caused by cold or dry air, exercise, aspirin. causes production of IgE antibodies
what can reverse asthma?
bronchodilator such as albuterol
what are symptoms of asthma?
dyspnea and wheezing
what is emphysema?
the destruction of alveoli that reduces the SA for gas exchange, with fewer alveoli to put pressure on the bronchiles, they collapse during expiration (vicous cycle)
what is the most common cause of emphysema
cigarette smoking since it triggers inflammation and destruction of alveoli by immune cells
what is chronic obstructive pulmonary disease (COPD)?
chronic inflammation, narrowing of the airways, and alveolar destruction. Includes emphyema an dchonric obstructive bronchitis, accelerated decline in FEV1, and excessive mucus production and inflammation triggered most often by smoking
what might COPD patients develop?
cor pulmonale: pulmonary hypertension with hypertrophy and eventual failure of RV
what is pulmonary fibrosis?
the accumulation of fibrous connective tissues proteins in the lungs, when alveoli are damaged. this may be due to inhalation of small particles (black lung in miners)