Neoplasia & Neoplastic diseases (MODS-EXAM 1)
1/45
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
46 Terms
Define a tumor
An uncontrolled, abnormal growth of cells or tissues, also referred to as a nodule or mass
Define Neoplasia
Defined as "New Growth"
Define cancer
A disease in which abnormal cells divide uncontrollably and destroy body tissue.
Define oncology
The branch of medicine that specializes in the diagnosis and treatment of cancer
Define malignancy
The presence of cancerous cells.
Define metastasis
A pathogenic agent's spread from an initial or primary site to a different or secondary site.
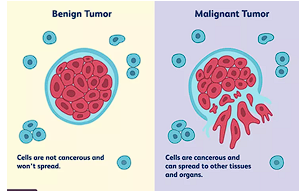
what is a benign tumor?
Describes a neoplasm that stays localized in one place. These cells are not cancerous and will not spread.
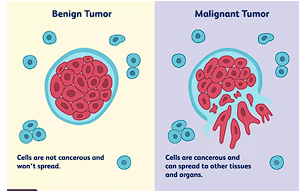
What is a malignant tumor
Describes a neoplasm that invades surrounding tissue and can metastasize to distant organs. These cells are cancerous and can spread to other tissues.
What are the terminologies that is related to microscopic appearance of neoplasms
Differentiation
Anaplasia
Dysplasia
Carcinoma in situ
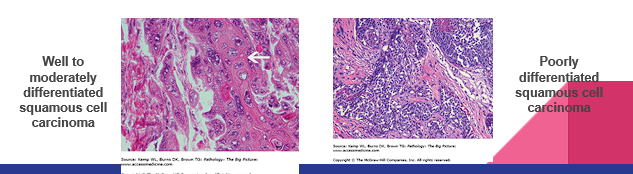
Describe differentiation in microscopic appearance of neoplasms
The extent to which a neoplastic cell resembles a normal cell from which it arose.
Classified as “well differentiated, moderately differentiated, poorly differentiated”
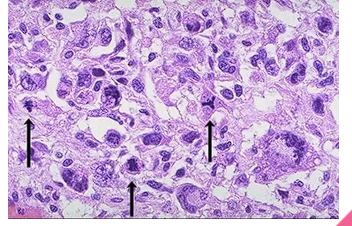
Describe Anaplasia in microscopic appearance of neoplasm
Meaning "to form backward," these are cells that lose their specialized characteristics and revert to a more primitive, embryonic state.
Describe Dysplasia in microscopic appearance of neoplasm
disordered growth of epithelium. There is a loss of cellular uniformity and architectural orientation. The cells may have an increased number of mitotic figures.
Doesn’t always form a mass or tumor therefore not always referring to a neoplasm
Can be reversible, if the inciting agent is removed
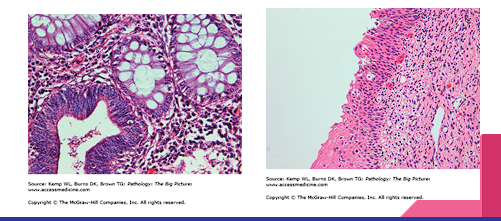
Describe carcinoma in situ in microscopic appearance of neoplasm
full thickness dysplasia of the epithelium
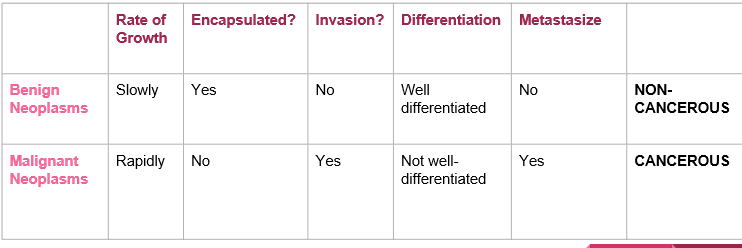
Discuss the features used to distinguish benign neoplasms from malignant neoplasms
Benign Neoplasms (NON-CANCEROUS)
Rate of Growth: Slowly
Encapsulated: Yes
Invasion: No
Differentiation: Well differentiated
Metastasize: No
Malignant Neoplasms (CANCEROUS)
Rate of Growth: Rapidly
Encapsulated: No
Invasion: Yes
Differentiation: Not well-differentiated
Metastasize: Yes
Describe the pre-clinical phase of cancer
This is the phase in which the patient may not demonstrate symptoms or physical examination findings consistent with the disease.
May be identified by screening interventions.
Examples include polyps in the colon for colon cancer, and proliferative abnormalities in the breast for breast cancer.
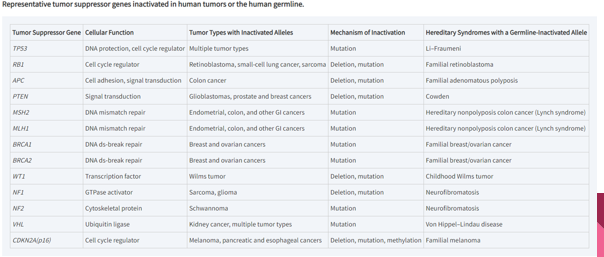
Describe the functions and methods of inactivation of tumor suppressor genes.
Functions: Help control cell growth by acting as a "braking signal". When functioning properly, they can prevent and inhibit the growth of tumors.
Methods of inactivation: They can be inactivated through deletion, mutation, or methylation. When altered or inactivated, they lose the ability to control cell growth, which leads to cancer.
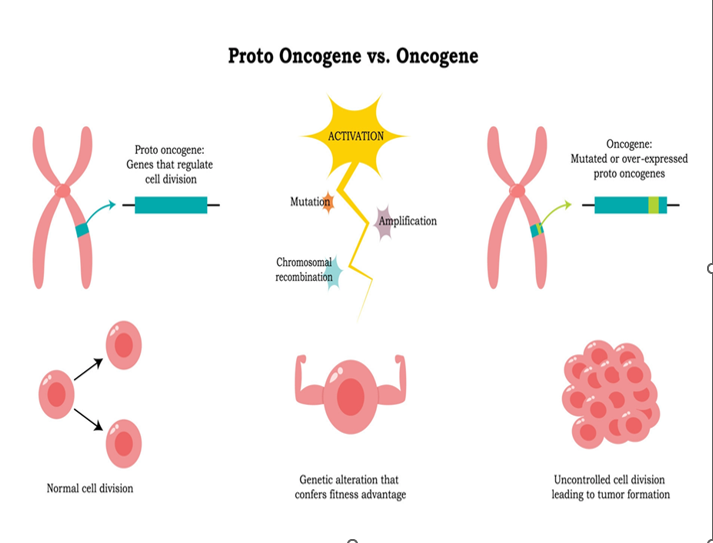
Describe the functions and methods of activation of proto-oncogenes.
Functions: A normal cellular gene that promotes cellular growth and division.
Methods of Activation (Conversion to Oncogenes):
Overexpression of the gene.
Amplification of the gene.
Point mutation in the gene.
Translocation of the gene to another region with a strong promoter of the
gene.
Describe RAS and their connection to clinical oncologic disorders
An oncogene where mutations lead to cellular division. It is connected to colon cancers.
Define KRAS and their connection to clinical oncologic disorders
An oncogene that is another member of the RAS family. It is connected to lung, colon, and pancreatic cancers.
Define HER2 and their connection to clinical oncologic disorders
An oncogene that synthesizes growth factor receptors. It is connected to breast cancers.
Define APC gene and their connection to clinical oncologic disorders
A tumor suppressor gene. Disruption of this leads to adenomas (non cancerous polyps) which then lead to colon cancer.
Define P53 and their connection to clinical oncologic disorders
A tumor suppressor gene. It is inactivated in many cancers and cannot repair DNA or lead to apoptosis. It is connected to leukemias.
Define BRCA 1 and BRCA 2, and their connection to clinical oncologic disorders
Tumor suppressor genes involved in DNA repair. Mutations are related to both breast and ovarian cancers.
Define Hepatitis B virus and their connection to clinical oncologic disorders
An oncogenic virus associated with hepatocellular carcinoma. It works through chronic inflammation and by HBV protein binding to p53, interfering with its function leading to cancer.
Define Helicobacter pylori and their connection to clinical oncologic disorders
Associated with MALTomas of the stomach (neoplasm of mucosa-associated lymphoid tissue).
What is human herpes virus 8 connection to clinical oncologic disorders
Associated with primary effusion lymphoma and Kaposi sarcoma.
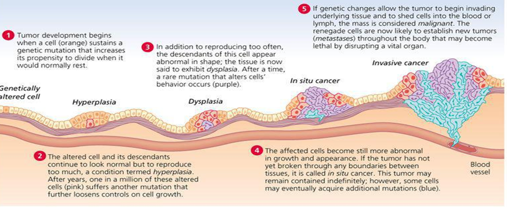
Describe examples of early, middle and late changes in the progression of neoplasia.
Early Changes (Initiation and Early Hyperplasia)
Middle Changes (Dysplasia and Benign Tumor Growth/ In situ cancer)
Late Changes (Malignancy, Invasion, and Metastasis)
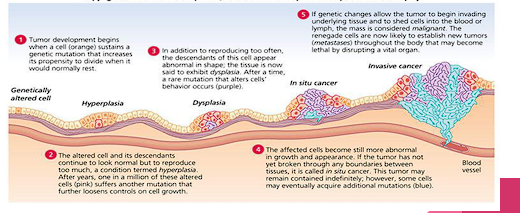
Describe examples of middle changes in the progression of neoplasia.
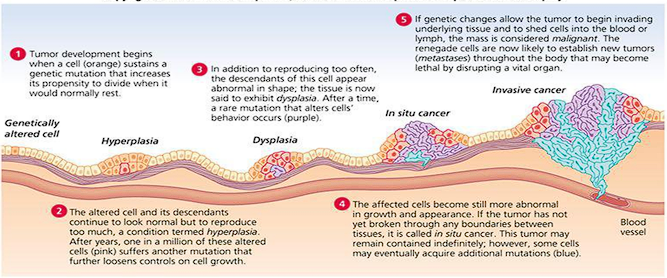
Descendants of the cell appear abnormal in shape, leading to dysplasia (intermediate adenoma). Growth and appearance become more abnormal forming an in situ cancer (late adenoma) that has not broken boundaries.
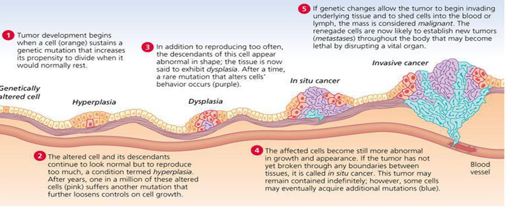
Describe examples of late changes in the progression of neoplasia.
Genetic changes allow the tumor to invade underlying tissue (invasive carcinoma), and shed cells into the blood or lymph to establish new tumors throughout the body (metastatic carcinoma).
Describe the classifications of neoplasia based upon their embryonic origins, Carcinoma and Sarcoma:
Carcinoma: Derived from ectodermal and endodermal tissue. It is the most common type of cancer and includes epithelial tissue cancers like lung, colon, breast, and prostate cancer.
Sarcoma: Originates from mesodermal tissue. It arises from mesenchymal cell types in connective tissue, such as fat, cartilage or bone.
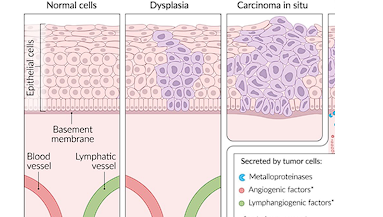
Describe the phenotypic changes in the progression of neoplasia.
Genetically altered cell that sustains a mutation increasing its propensity to divide.
Hyperplasia: The cells look normal but reproduce too much.
Dysplasia: The cells appear abnormal in shape.
In situ cancer: Affected cells become more abnormal in growth and appearance but remain contained without breaking boundaries.
Invasive cancer / Metastases: The mass becomes malignant, invading underlying tissue, shedding cells into the blood or lymph, and establishing new lethal tumors throughout the body.
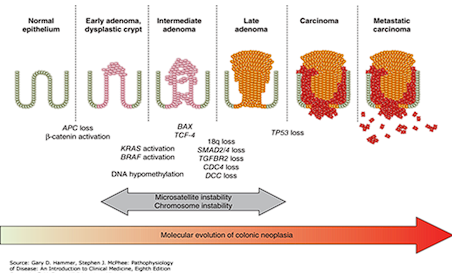
Describe colon carcinoma and what type of classification of neoplasia is it ?
Progresses from normal epithelium to adenomas and eventually to invasive and metastatic carcinoma.
mutated APC gene (tumor suppressor gene)
Epithelial
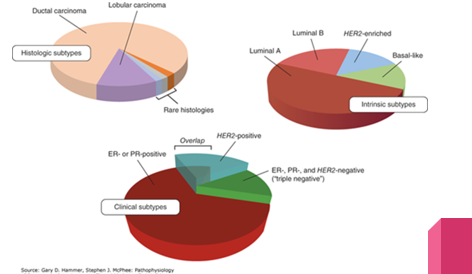
Describe breast carcinoma and what type of classification of neoplasia is it ?
Can be classified by histologic subtypes (ductal or lobular), clinical subtypes based on hormone receptors (ER, PR, HER2), or intrinsic molecular subtypes (Luminal A, Luminal B, HER2-enriched, Basal-like).
Epithelial
Define Neuroendocrine
derived from cells that may have developed enzymatic capabilities and secretory functions found in the endocrine and nervous systems
•Ex: Carcinoid tumor, pancreatic neuroendocrine tumor
Define Germ cell
arise within testes or in extra gonadal sites through which germ cells migrate during development
•Ex: Testicular germ cell cancer
Define Mesenchymal
cells that develop into connective tissue, blood vessels, lymphatic tissue
•Ex: Sarcomas
Describe carcinoid tumors and what type of classification of neoplasia is it ?
Low grade neuroendocrine tumors (NET) that derive from cells with enzymatic and secretory functions
NETs can secrete vasoactive substances (EX: serotonin, ADH)
Secretion of serotonin can cause:
Flushing (vasodilation)
Secretory diarrhea
Wheezing
Excessive salivation or lacrimation
Neuroendocrine
Describe Testicular germ cell cancer and what type of classification of neoplasia is it?
Arises within the testes from germ cells that normally give rise to spermatozoa.
germ cell
Describe sarcomas and what type of classification of neoplasia is it?
Arise from mesenchymal connective tissues like bone, muscle, or cartilage.
Metastasize via systemic blood vessels (most often to lung)
More common in childhood; rare in adulthood <1%
Examples:
Osteosarcoma (sarcoma of bone)
Rhabdomyosarcoma (skeletal muscle)
Leiomyosarcoma (smooth muscle)
Liposarcoma (fat cells)
Gastrointestinal stromal tumors (GISTs)
Kaposi Sarcoma (HHV-8) in HIV patients
Mesenchymal
Describe lymphomas and what type of classification of neoplasia is it?
Affect the lymph nodes and blood
Indolent (less active) or Aggressive
EX:
Hodgkin lymphoma (mix of malignant and benign inflammatory cell types)
Non-Hodgkin lymphomas
Chronic Lymphocytic Leukemia (CLL)
Hematologic
Describe acute and chronic myelogenous leukemia and what type of classification of neoplasia is it?
Myeloproliferative neoplasms feature proliferation of myeloid lineages (granulocytes, erythroid cells, megakaryocytes)
Chronic myelogenous leukemia (CML) can transform into acute leukemia (blast crisis)
indolent course
Philadelphia chromosome, translocation chromosomes 9, 22, bcr-abl
Hematologic
Discuss how grading is used to predict the clinical behavior of a malignant tumor
Describes the appearance and behavior of the tumor cells to determine differentiation, nuclear chromatin quality, and proliferative rate.
Low-grade tumors resemble normal tissue and have a better prognosis, whereas high-grade tumors appear primitive, grow rapidly, and have higher metastatic potential.
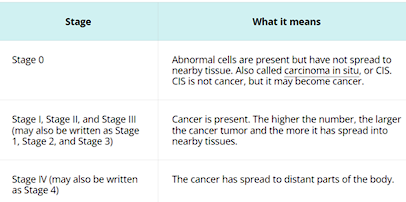
Discuss how staging is used to predict the clinical behavior of a malignant tumor and describe each one
Numerical staging system (I-IV)
Describes the anatomic extent and spread of the cancer at and beyond its site of origin
TNM staging system
Assesses Tumor size, Number of lymph nodes involved, and Metastasis stage (diff for each cell)
Clinical staging
Applied at time of presentation based on PE and radiographic findings
Pathological staging
Staging system applied after surgical resection of the primary tumor and sampling of the regional lymph nodes
List and describe the direct effects of malignancies
Bone marrow involvement causes pancytopenia, infection, or bleeding.
A brain mass causes neurological deficits like weakness, numbness, gait abnormality, visual changes, or headache.
Invasion of a nerve causes neurologic deficits like numbness, weakness, or pain.
Invasion of a blood vessel causes hemorrhage.
Impingement upon vasculature causes ischemia or infarction of tissue.
An obstructing mass causes bowel obstruction, constipation, pneumonia, or bile duct jaundice.
Bone destruction causes pain and pathologic fracture.
List and describe the indirect effects (Paraneoplastic syndromes) of malignancies
These are side effects affecting distant targets uninvolved by the tumor, generally through hormones or immune activation.
Cachexia: Loss of body fat and muscle, weakness, and anorexia associated with a neoplasm ("cancer wasting").
Hormone Production: Tumors can produce PTH (hypercalcemia), ACTH (Cushing syndrome), SIADH (hyponatremia), or Erythropoietin (polycythemia).
Nerve and muscle syndromes: Such as Lambert-Eaton syndrome, a myasthenia gravis-like syndrome caused by antibodies against presynaptic Ca channels
Describe the role of hormones, growth factors and other cellular genes in carcinogenesis
Hormones promote cancer by driving rapid cell division that increases the risk of DNA replication errors, while hijacked growth factors provide the tumor with continuous, self-sustaining growth and survival signals. Ultimately, this uncontrolled proliferation is driven by underlying mutations in cellular genes that permanently activate oncogenes (the "gas pedal") and disable crucial tumor suppressor and DNA repair genes (the "brakes").