radiographic interpretation of dental caries
1/40
Earn XP
Description and Tags
lecture given 4/6/2026
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
41 Terms
if a new adult patient comes into your office and has no visible pathology and closed contacts, what radiographs should you take, if any?
pano and bitewings
what kind of electron interaction do we want to get radiographs?
photoelectric aka characteristic radiation
electrons interact with inner shell electrons
t/f demineralization of tooth structure is a dynamic process by an infectious disease
true
what factors contribute to caries?
bacteria- plaque or biofilm, strep mutans
diet- fermentable carbohydrates
what factors prevent caries?
hygiene- remove or interrupt bacterial plaque
fluoride- remineralizes outer surface of tooth and makes it more resistant to demineralization
what are the steps of caries detection?
patient history
clinical exam- visual, tactile, caries detection dye, transillumination, electronic caries monitor
radiographic assessment *done last!
what is the ranking of caries diagnostic value of radiographs, from most to least?
bitewing, periapical, pano, CBCT
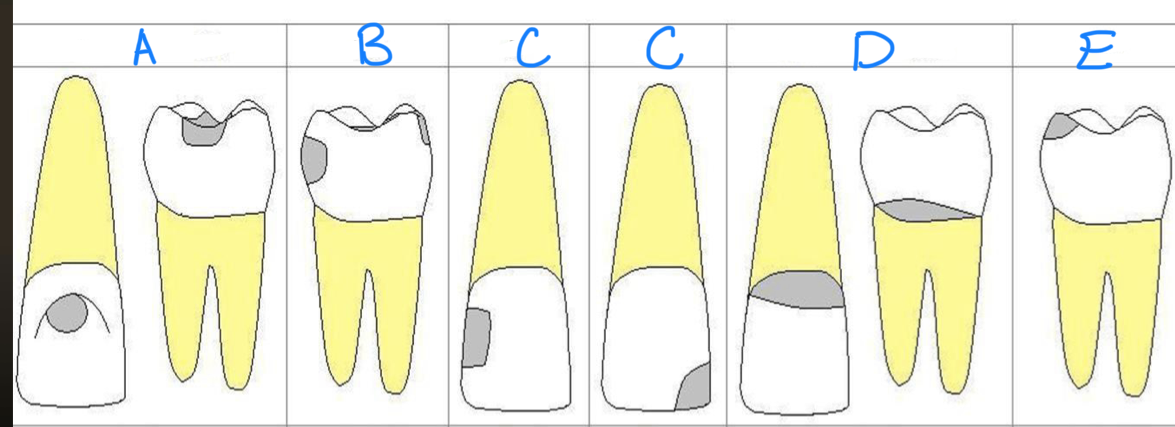
a?
class I, occlusal surfaces
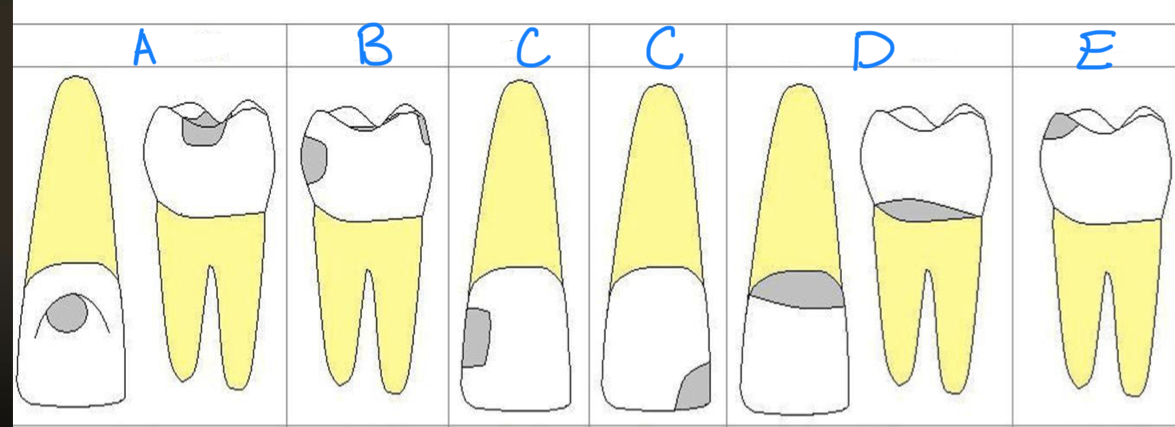
b?
class II, proximal surfaces
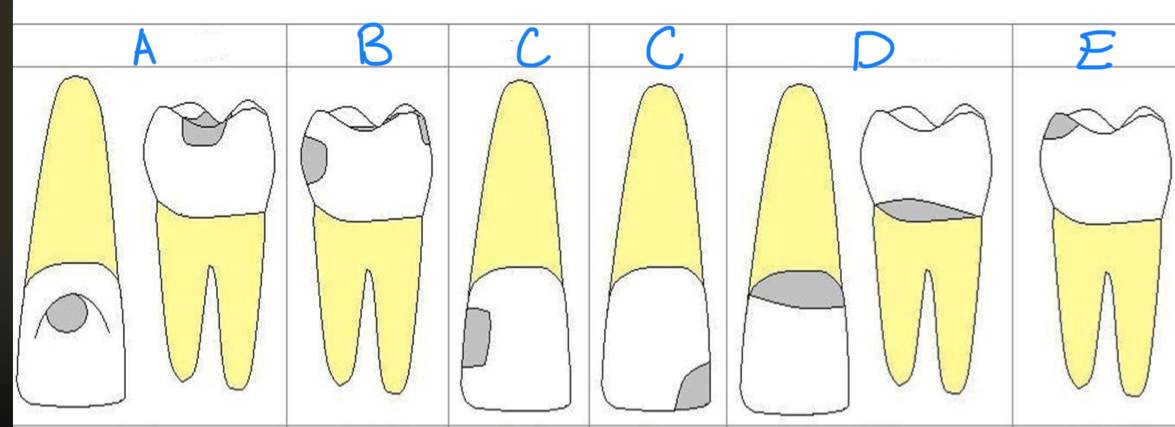
c? left lol sorry
class III
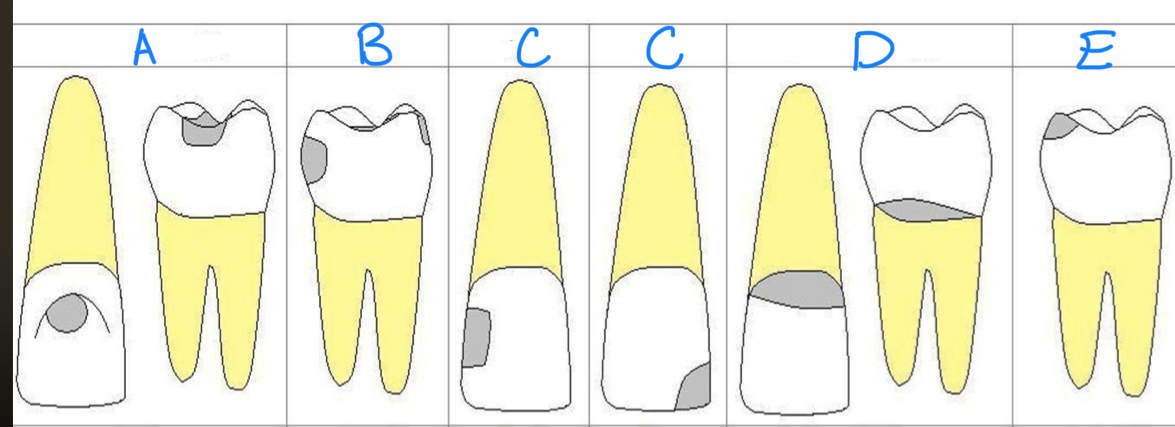
c? right
class IV
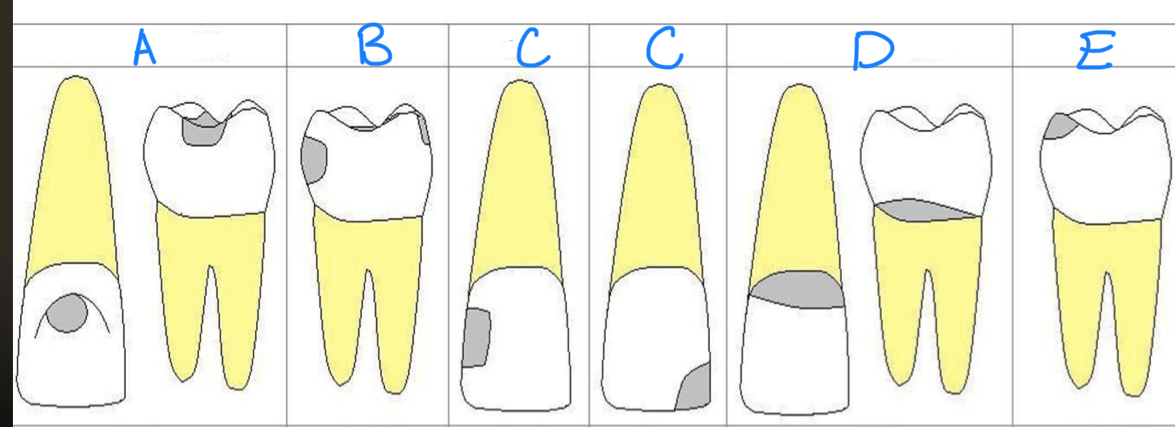
d?
class V, buccal and lingual surfaces or root surfaces
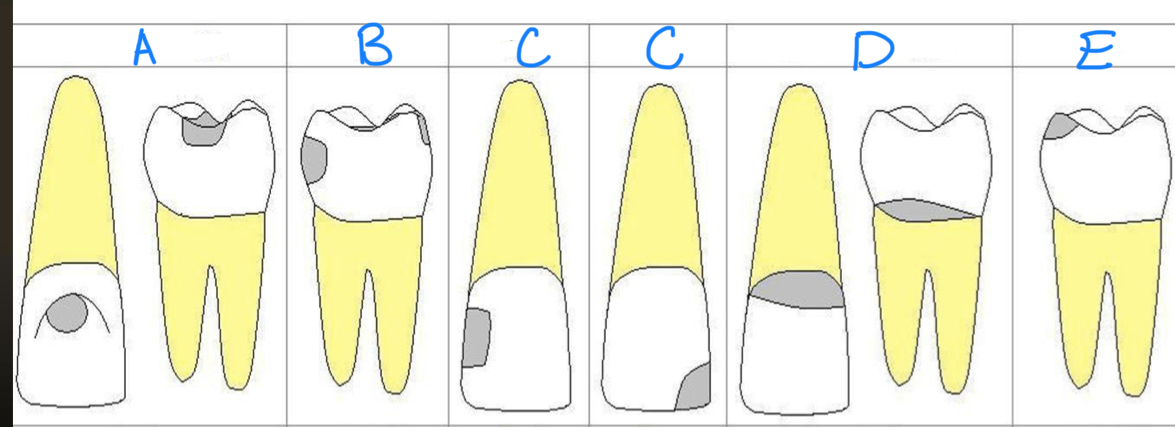
e?
class VI
where are interproximal caries likely to develop?
the most superior zone of contact to the papilla
interproximal caries- incipient
caries suseptible zone
do not extend into DEJ
triangle with broad base at outer surface
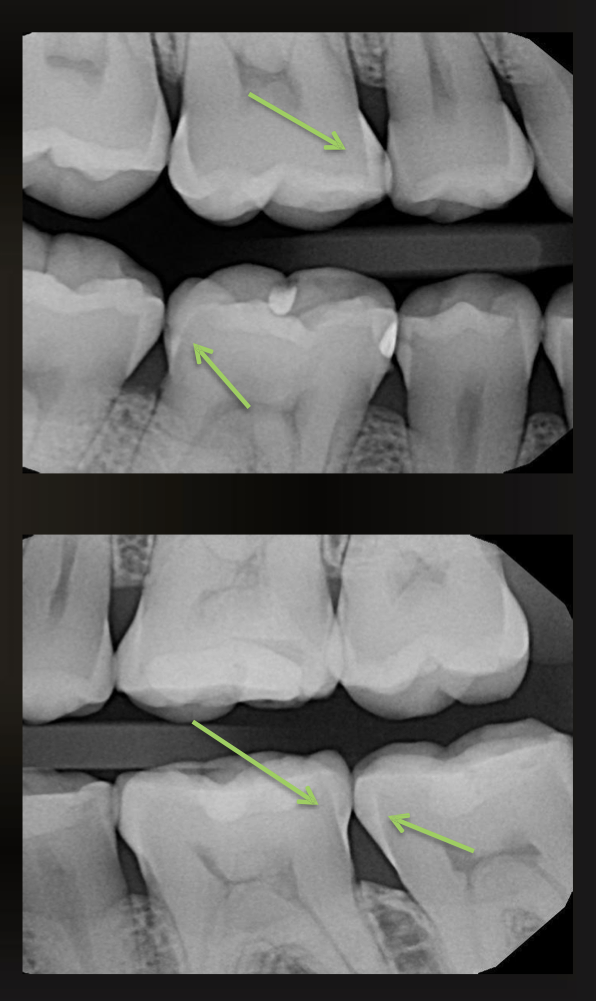
what are the arrows pointing to?
incipient interproximal caries
how do interproximal caries spread?
along the DEJ
into dentin- creates a second triangle at the base of the DEJ
in some cases, lesion may appear not to have penetrated enamel
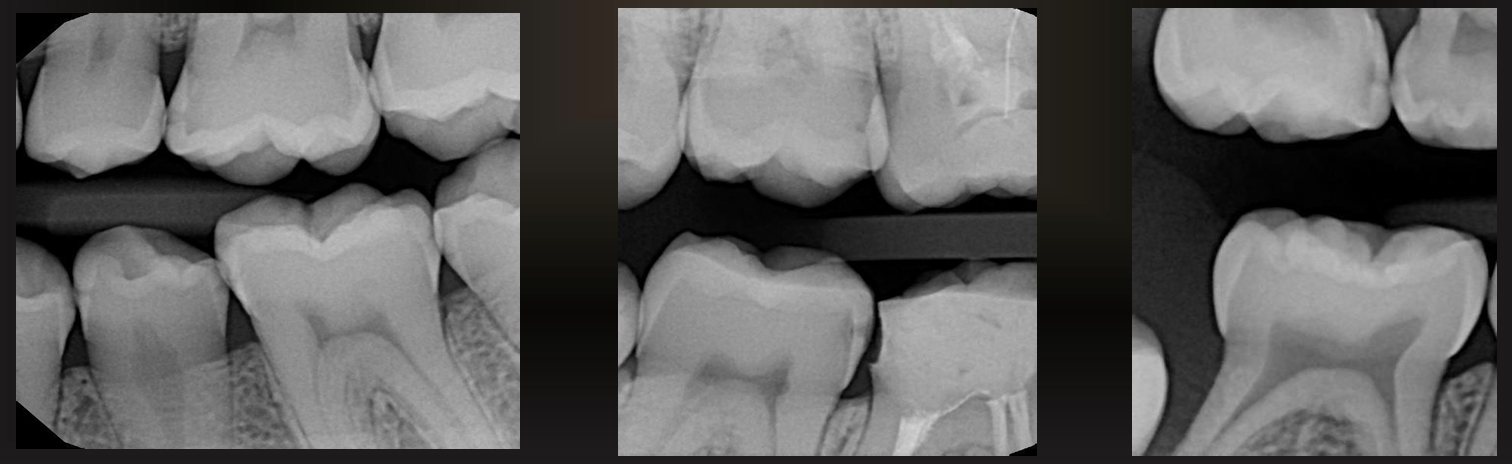
what do these images have?
interproximal caries (not incipient)
are these caries or restorations with radiolucent material?
caries
are these caries or restorations with radiolucent materials?
restorations with radiolucent materials
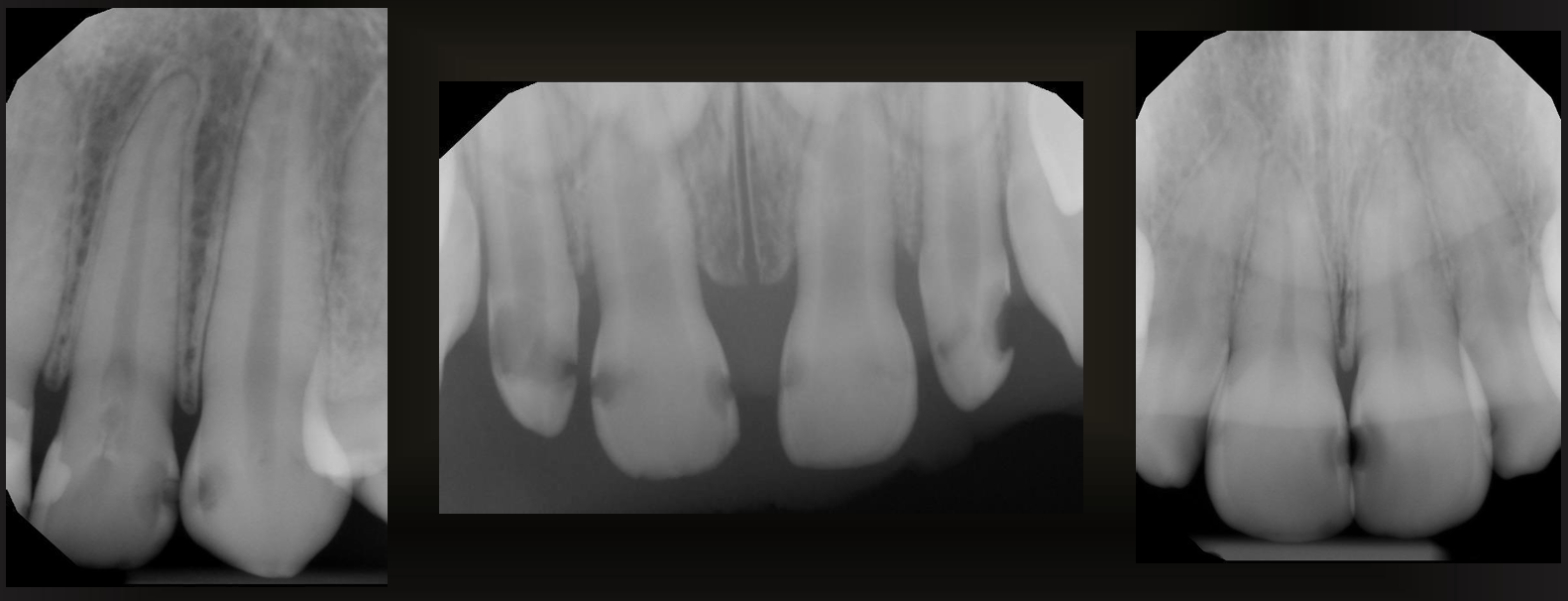
what is this arrow pointing at?
secondary caries
large occlusal caries
easily observed, appear as large/dark circles in the crown
pulp exposure cannot always be determined
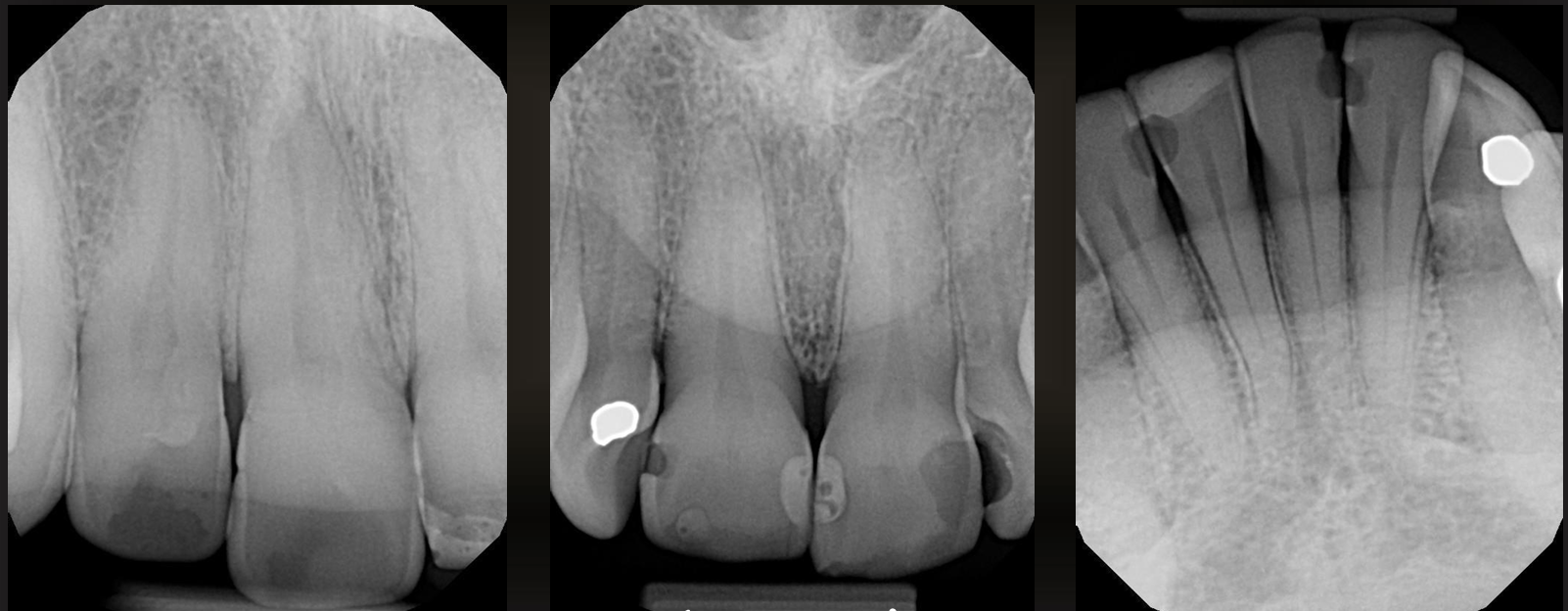
what are these?
large occlusal caries
small occlusal caries
radiographs are not very effective at detecting, may be seen as thin radiolucent line or cup shaped zone underlying occlusal enamel
minimum or no changes in enamel
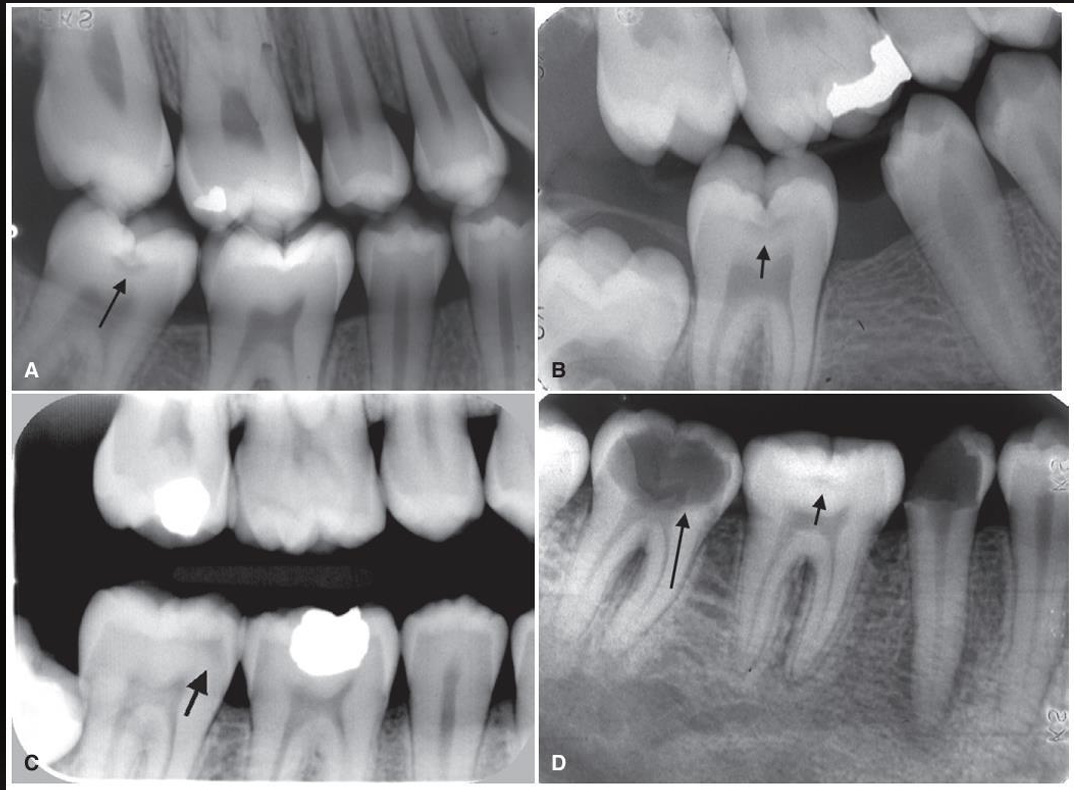
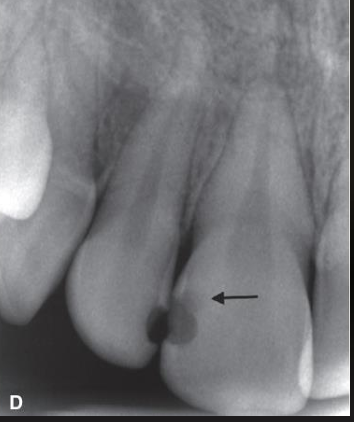
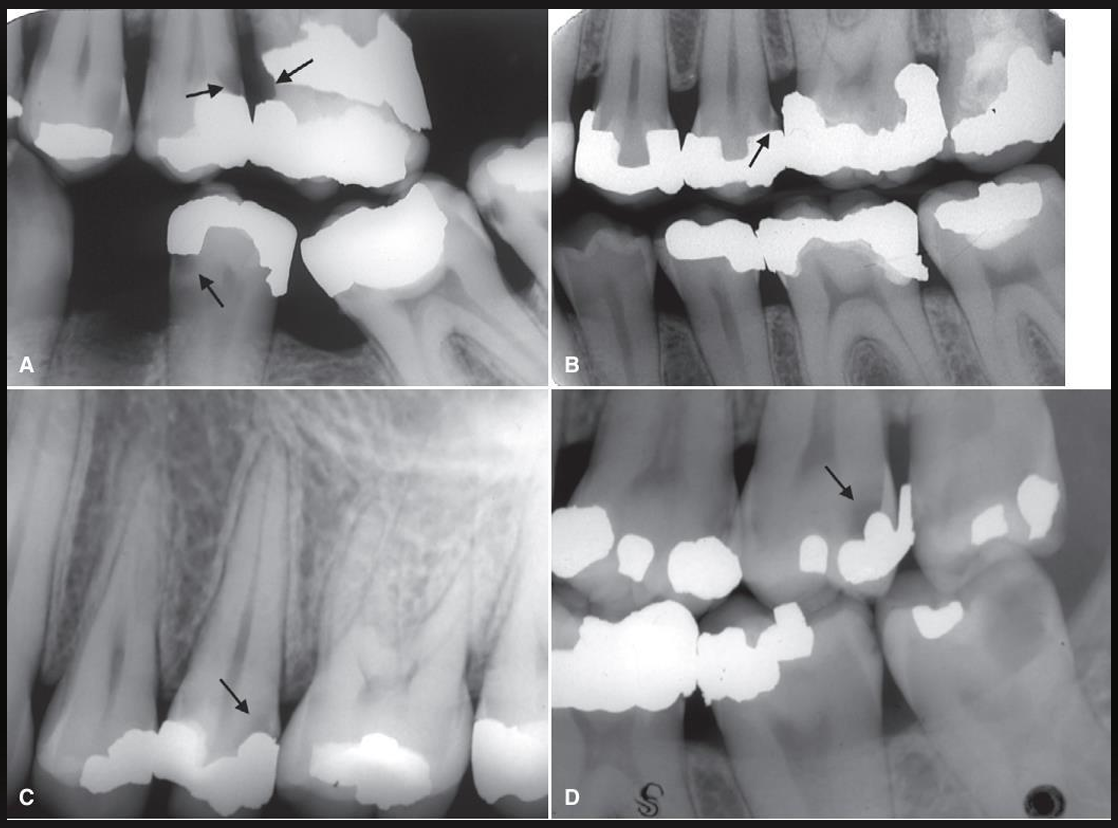
what are these arrows pointing at? (except for 2nd molar in image D)
small occlusal caries
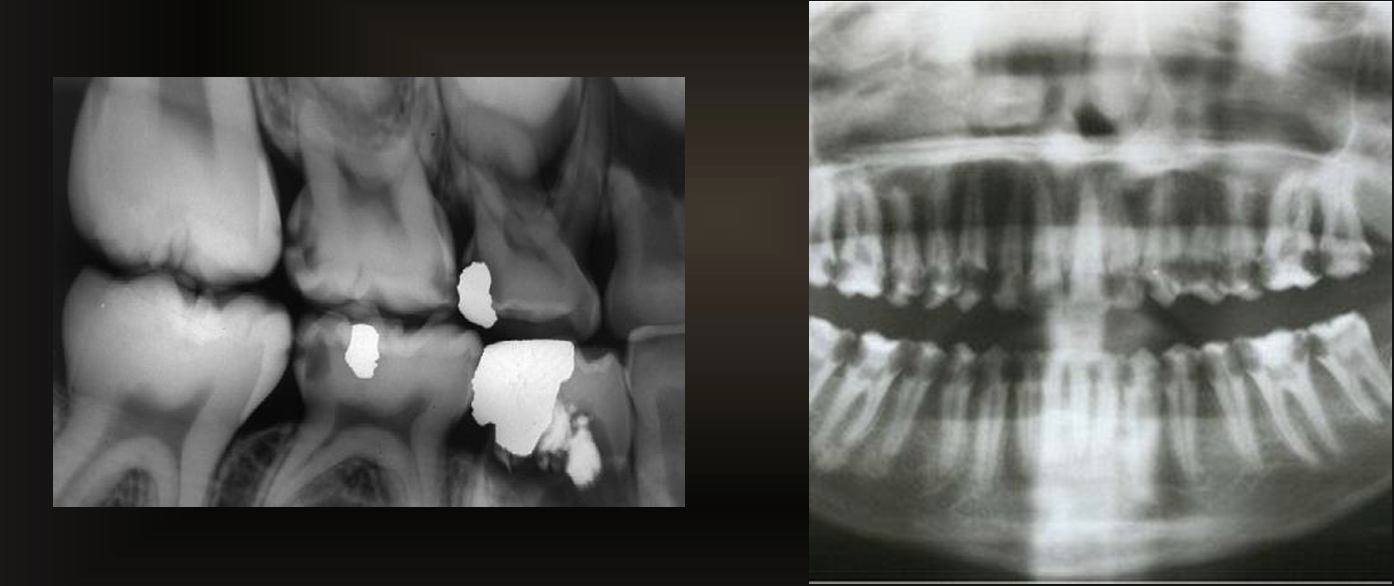
rampant caries
affects almost all teeth- usually caused by radiation
root surface caries
cratering on the roots of the teeth, involving cementum
buccal/lingual/proximal
saucer like radiolucency
may be confused with cervical burnout
can you have root surface caries without exposed roots?
no!
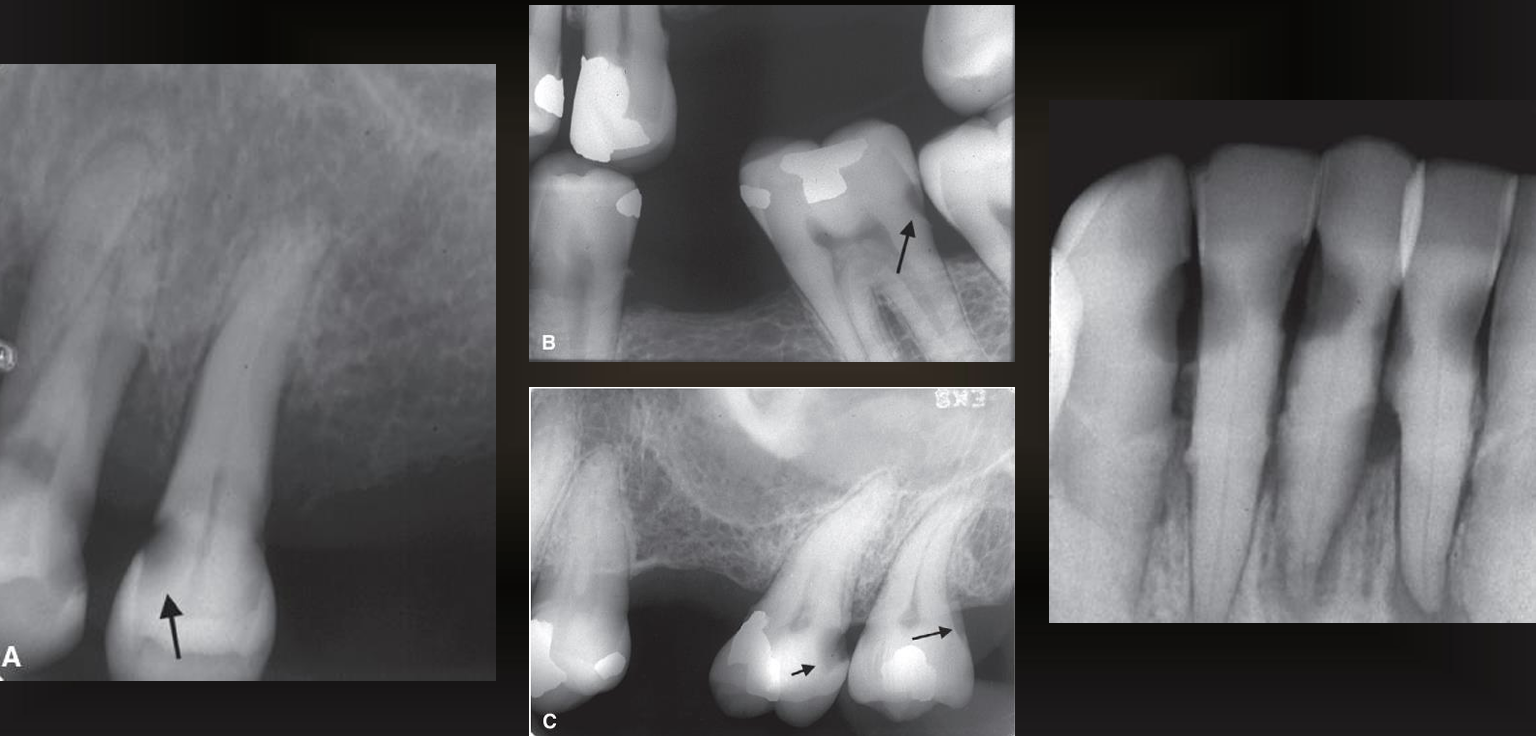
what are the arrows pointing to?
root surface caries
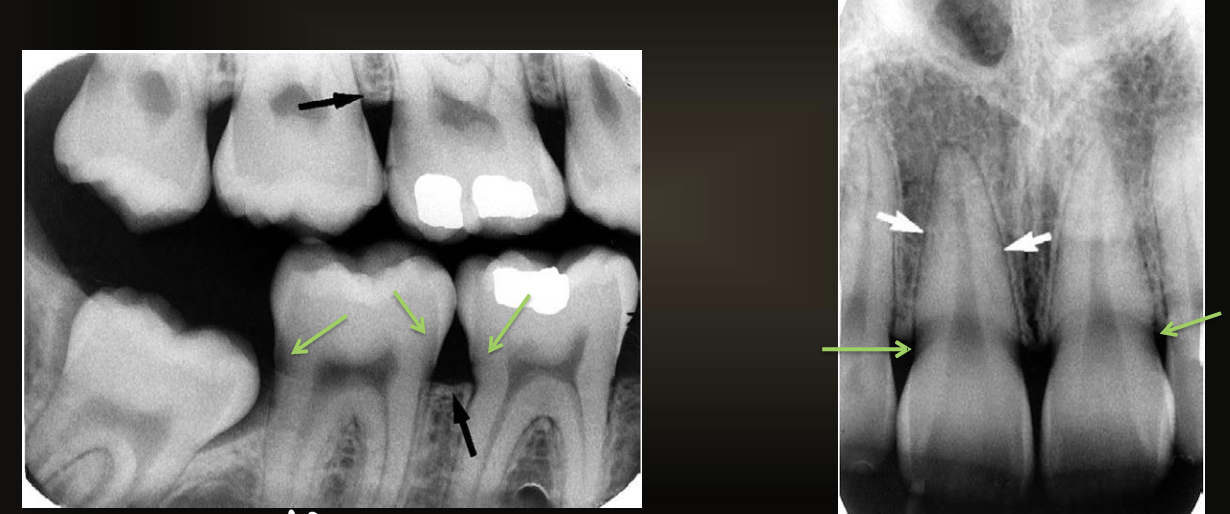
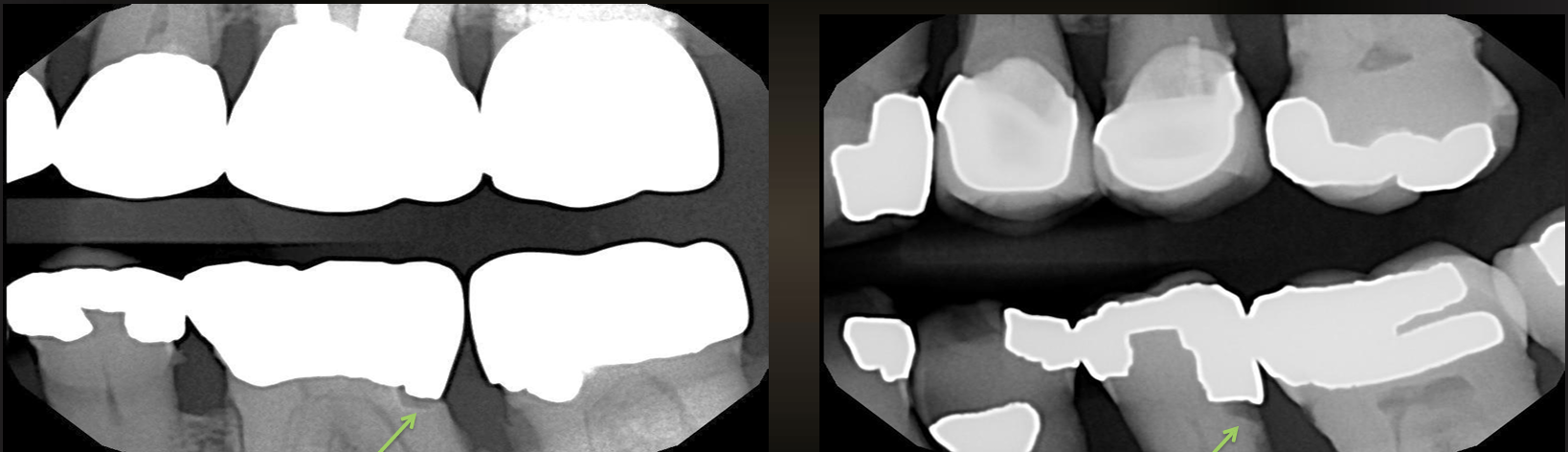
what are the green arrows pointing at?
cervical burnout
how can you tell if its cervical burnout or caries?
there is no bone loss, it affects multiple teeth, and if the angle of the radiograph changes the radiolucency is gone
recurrent caries
around the margin of existing restorations, spreads in a natural way
what do these images have?
recurrent caries
what are these arrows pointing at?
a restoration with a radiolucent liner- the box is too sharply defined to be a natural process (like secondary caries)
what are diagnostic confounders?
pits and fissures, cervical burnout, mach band effect, dental anomalies like hypoplastic pits and concavities produced by wear
mach band effect
an optical illusion where the human eye perceives faint light and dark bands at the boundary of two shades of gray, even if the transition is gradual

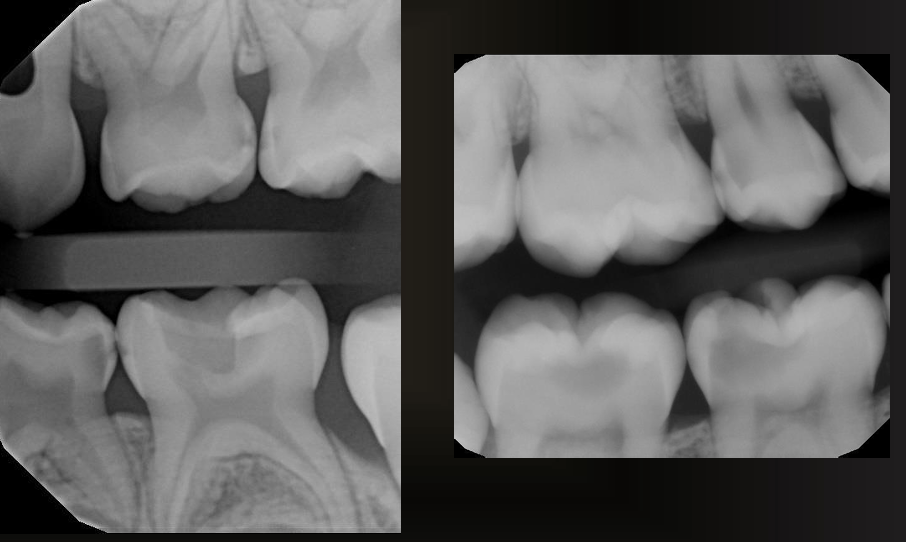
what is shown in the non-restored premolar?
mach band effect- the faint dark line under enamel is not caries, it is an ~optical illusion~
if you change angulation of radiograph or CBCT it would disappear
cervical burnout
apparent radiolucency below the CEJ due to anatomy or a gap between the enamel and bone covering the rooth
no root caries unless there is alveolar bone loss

what is the arrow pointing to?
hypoplastic pit
t/f the extent of caries you see on a radiograph is the same as what it will be when you drill
false- has to be significantly decalcified to be visible on x ray
t/f having overlap makes it easier to see interproximal caries
false- impossible