L17- Application of molecular pathology in cancer detection and treatment
1/51
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
52 Terms
whats the process of tumor spread
• Early dissemination from primary tumour
• Late dissemination from primary tumour
• Genetic divergence of primary and metastatic tumours has implications for treatment

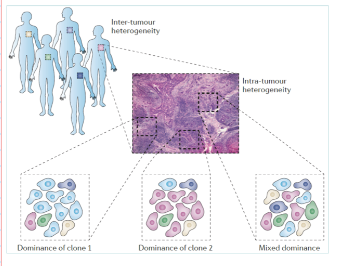
what is intra-tumor heterogeneity
• Common and unique mutations
• Varying aggressiveness
• Distinct clinical and biological features
• Different metastatic capabilities
what genomic alterations can occur in cancer
Point mutations
Translocations
Gene amplification
Epigenetic modifications
Deletions
Aberrant RNA splicing
Altered gene expression
what ways can cancer cell survival be promoted die to genomic pertubations
Cell cycle control
DNA repair
Differentiation
Apoptosis
Tumour vascularisation
Metabolism
How is breast cancer classified pathologically?
Cancer is a complex disease
Two main categories:
Carcinoma (epithelial origin):
Ductal carcinoma in situ (DCIS)
Lobular carcinoma in situ (LCIS)
Invasive ductal carcinoma
Rare subtypes: medullary, mucinous (colloid), tubular, papillary
Invasive lobular carcinoma
Sarcoma (stromal/connective tissue):
Phyllodes tumour
Angiosarcoma
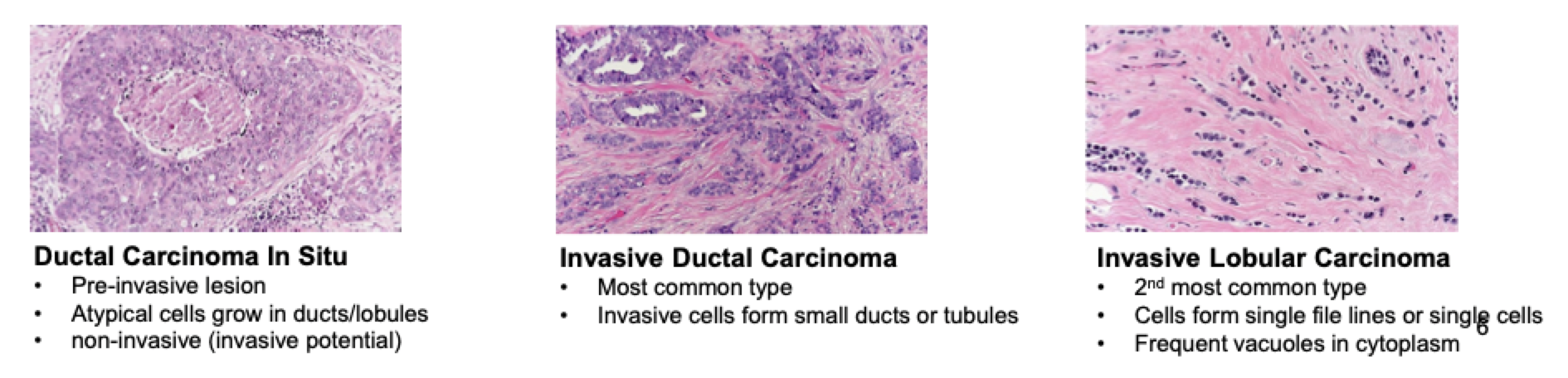
What are the key features of major breast cancer subtypes?
Ductal carcinoma in situ (DCIS):
Pre-invasive lesion
Atypical cells in ducts/lobules
Non-invasive but has invasive potential
Invasive ductal carcinoma:
Most common type
Cells form small ducts or tubules
Invasive lobular carcinoma:
2nd most common type
Cells form single-file lines or single cells
Frequent cytoplasmic vacuoles
what was the main treatment option for breast cancer
Breast is oestrogen dependent organ, remove oestrogen and tumour shrinks
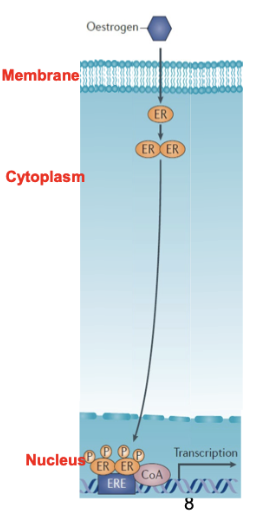
Why is breast cancer often hormone-dependent and how is this exploited therapeutically?
Breast is an oestrogen-dependent organ
Removing oestrogen (e.g. oophorectomy) can cause tumour shrinkage
ER-positive cancers (~70%) depend on oestrogen signalling
Treated with tamoxifen (anti-oestrogen) → blocks oestrogen receptor activity
Prevents oestrogen-driven tumour growth
What are the main breast cancer subgroups based on receptor expression and their treatments?
ER-positive (~70%)
ER⁺ / PR⁺, luminal markers
Subtypes: Luminal A, Luminal B
Treatment: Tamoxifen
HER2 (ERBB2) positive (~10%)
Overexpression of ERBB2 receptor
Treatment: Trastuzumab (targets extracellular domain of ERBB2)
Triple negative (~15%)
Lack ER, PR, HER2
Aggressive, heterogeneous
No clear target → chemotherapy
What characterises HER2-positive and triple-negative breast cancers?
HER2-positive:
Driven by ERBB2 receptor overexpression
Targeted with trastuzumab
Triple-negative:
Do not express ER, PR, or HER2
Aggressive and difficult to treat
No obvious receptor target → rely on chemotherapy
Normal-like (~5%)
Poorly understood subgroup
Underlying defects not well defined
Why is targeting the estrogen receptor (ER) important in breast cancer?
>70% of breast cancers are ER⁺ (ESR gene)
Estrogen drives tumour growth and breast development
Estrogen withdrawal ↓ proliferation (>90%)
ER⁺ tumours are treated with endocrine therapy (mainstay)
Tamoxifen → ER antagonist
Aromatase inhibitors → ↓ estrogen production
Fulvestrant → destabilises and antagonises ER
Prevents estrogen signalling (blocks nuclear activity/dimerisation)
What are the clinical outcomes and limitations of endocrine therapy in ER⁺ breast cancer?
Typically given for ~5 years post-surgery
Reduces recurrence and mortality
However, resistance develops over time
Many patients eventually relapse with metastatic disease
Require alternative endocrine therapies after resistance develops
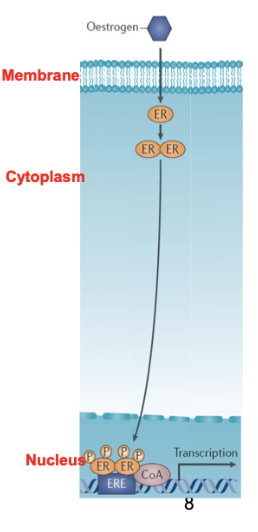
how does fulvestrant work
Fulvestrant-Prevent oestrogen from entering nucleus and cause oestrogen dimerising
How is genomic information used to identify cancer patient subgroups?
Genomics helps stratify patients into subgroups with shared genetic alterations
Discovery phase:
Identify biomarkers and therapeutic targets
Understand oncogenic mechanisms
Uses whole genome analysis, including:
Copy number & LOH (loss of heterozygosity)
Gene expression & alternative splicing
Methylation
Transcription factor binding
Linkage/association studies
Mutation analysis
How are genomic findings validated and applied clinically?
Validation phase:
Study larger patient cohorts
Statistically validate targets and biomarker signatures
Focus on fewer, relevant genes
Methods: copy number signatures, targeted genotyping
Clinical utility:
Classify patients by prognosis
Stratify based on treatment response
Each patient screened for gene alterations/signatures
Used in diagnostic assays and clinical decision-making
What is the overall workflow and key principle of using genomics to stratify cancer patients?
Patients are grouped based on common genetic alterations
Follows a pipeline:
Discovery → Validation → Clinical application
Trend across stages:
Start broad (whole genome, many genes)
Move to fewer, highly relevant genes
Study larger patient cohorts for validation
Final step:
Develop validated diagnostic assays
Apply in routine clinical practice for patient stratification
what does it mean that tumours are heterogenous- what is the clinical importance?
Interactions with different types of stroma and connective tissue etc
Need to be able to pick out tumour cells from other types of cells, so we only analyse their cells/DNA
if contain diff populations of clones with mutations in them, also mixes up DNA when analysing samples
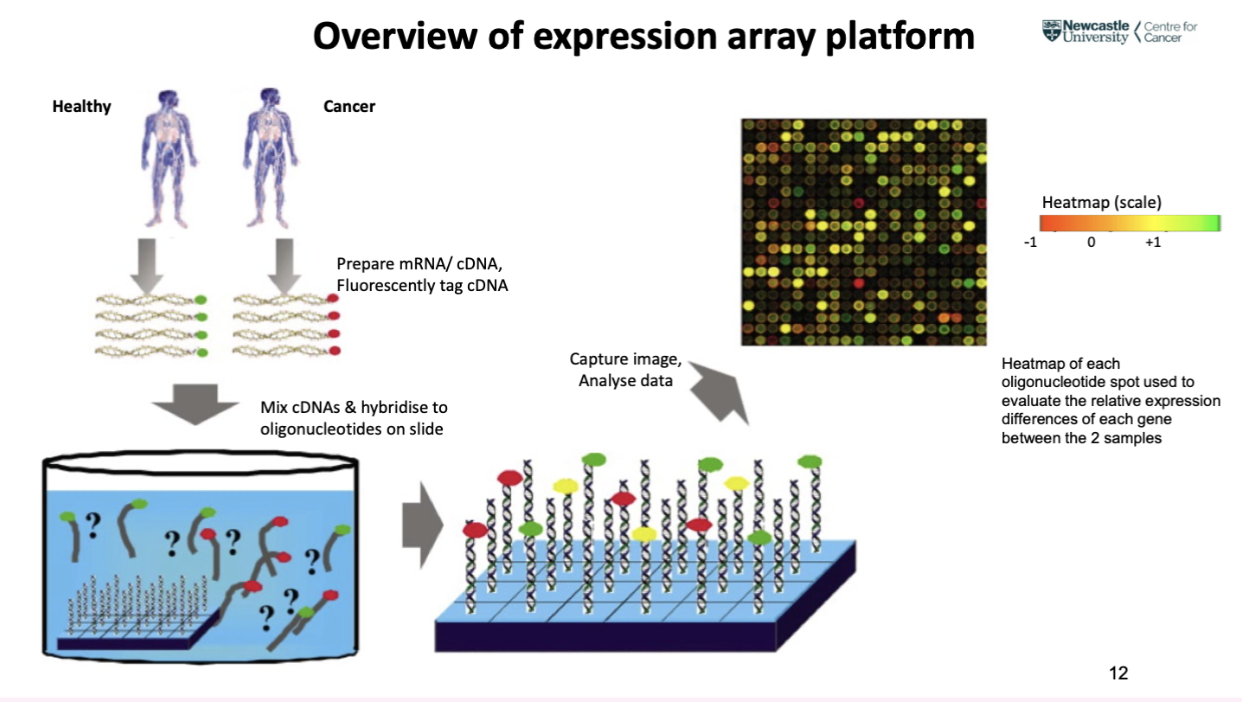
what are genetic array platforms
Tens-hundreds of thousands of oligonucleotide probes spotted onto glass slides
Probes-Against targets in the genome
Sample hybridised to slide, see what binds to specific probes
what are the types of genomic array platforms and what do they detect (4)
Expression array – mRNA, microRNA
Exon array – alternative splicing of mRNA
SNP array – somatic and germline mutation, gene amplification/deletion of DNA
DNA methylation array – CpG methylation sites associated with gene activity
what is the method for using expression array platforms
Take sample from cancer patient/tumour and a control sample- equal amounts
Isolate mRNA
Convert tp cDNA
Tagged with fluorescent probe (healthy green, cancer red)
mRNAs bind to probe
Detect level of fluorescent
Can look at the different of expression of healthy and cancer cells (as equal sample amounts were used)
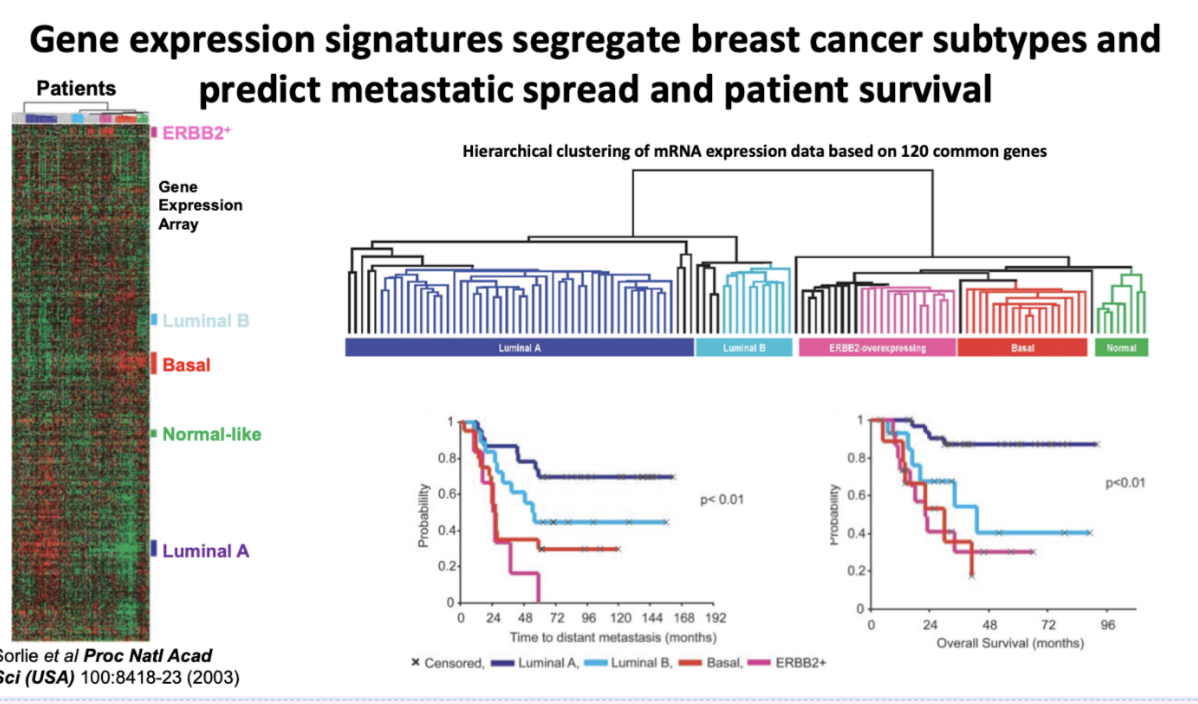
how is data from gene expression arrays used
Gene expression signatures segregate breast cancer subtypes and predict metastatic spread and patient survival
Use info to predict how patient will react to therapy and survival time
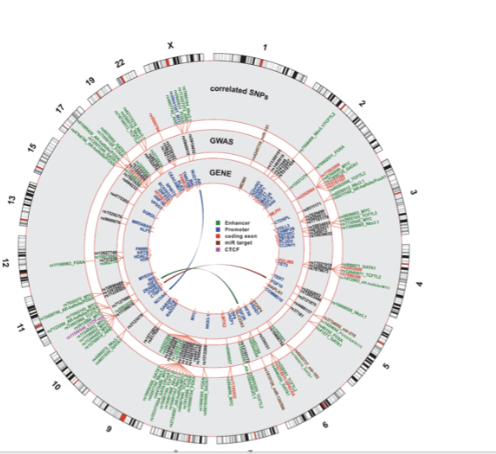
What are SNPs and why are they important?
Single-nucleotide polymorphisms (SNPs) = 1 base-pair DNA changes
Contribute to genetic variation between individuals (allele status)
Most SNPs have no effect, some cause subtle differences, others affect disease risk
~10⁷ SNPs in the human genome
~10⁶ SNPs are relevant to disease
Can influence risk of diseases (e.g. prostate cancer susceptibility)
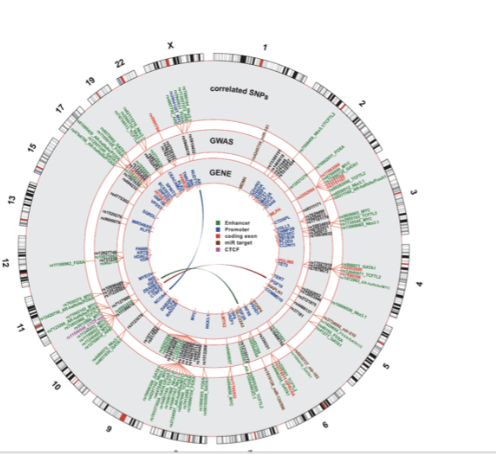
What are SNP arrays and how are they used in research?
Use DNA oligonucleotide probes to detect SNPs across the genome
Typically ~10⁶ SNPs analysed (~1 SNP per 3 kb)
Determine whether alleles are homozygous or heterozygous
Enable large-scale association studies (GWAS)
Example:
~43,000 prostate cancer cases vs ~43,700 controls
Identified 23 susceptibility loci
Used to link genetic variation to disease risk
What is meant by allele status in SNP analysis and why is it important?
Allele status = whether a SNP is homozygous or heterozygous
Determined using SNP arrays
Reflects individual genetic variation
Certain 1 bp changes (SNPs) can increase disease susceptibility
Key for linking genotype → disease risk in GWAS
what is the importance of the MDM2 SNP in cancer
Naturally occurring polymorphisms may influence individual’s susceptibility to cancer or response to treatment
SNP identified in a healthy population in MDM2 intronic promoter (SNP309, T to G change)
In binding site for TF- SP1
what does the MDM2 SNP cause
Transcription factor SP1 binds more strongly to promoter
Increased transcription from MDM2 promoter
elevated MDM2 mRNA (x8) and protein (x4)
MDM2 negative regulator of p53 and increased MDM2 protein expression attenuates p53 pathway promoting genetic instability
In patients - SNP309 genetic variants show susceptibility to tumour development and frequent metastases
what does next generation sequencing allow for
rapid sequencing of large genomes
1. Detailed sequence information for each individual provides a full genetic profile
predict development and progression of disease
First high quality ‘reference’ sequence of human genome completed in 2003
Sanger sequencing- used to cost millions
how can sanger sequencing be adapted
Adapted Sanger sequencing technology by miniaturisation
- fluorescent chain terminators and capillary electrophoresis
what do current sequencing strategies use
Current sequencing strategies use Nanopore sequencing
– bases identified as individual DNA strands are pulled through tiny holes in lipid bilayer (pore 2nm).
- one million nanopores running in parallel coan complete full genome sequencing in 1 hour
now costs less than 1000 pound
how is genome sequencing does using emulsion PCR
DNA taken from patient, made into SS and broken into fragments
Adaptor probes added to end of fragments
Fragments mixed with beads avg. one fragment to bead
Mix with lipid mix- 1 fragment on one bead enclosed in lipid droplet containing PCR mixture
PCR in situ in droplet
Millions of copies of one fragment in each droplet
Into nanopores for sequencing
Droplets burst and release beads
Sequencing done within each pore
Can sequence billions of fragments to be aligned by a computer
describe molecular profiling of primary breast cancer
correlations of mutations with genomic and clinical features (n=11,500)
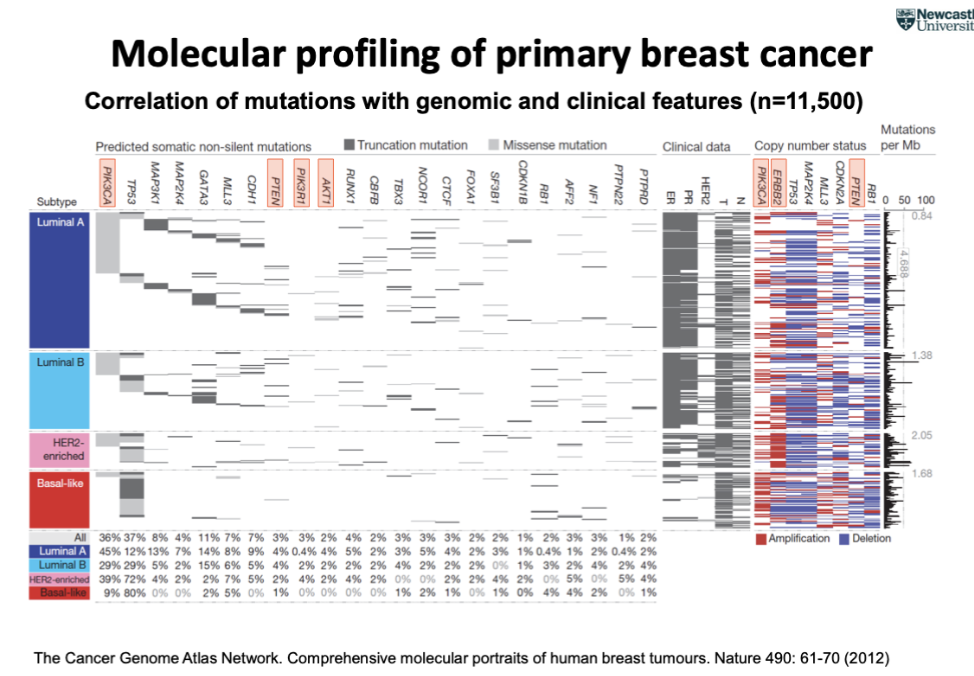
What does next-generation sequencing (NGS) reveal about breast cancer subgroups?
NGS allows stratification of patients into subgroups (broader classification than IHC)
Identifies >10 distinct breast cancer subgroups
These subgroups have different clinical outcomes (survival differences)
Survival curves show clear separation between groups (log-rank P ≈ 1.2 × 10⁻¹⁴)
Enables more precise prognostic classification beyond traditional subtypes
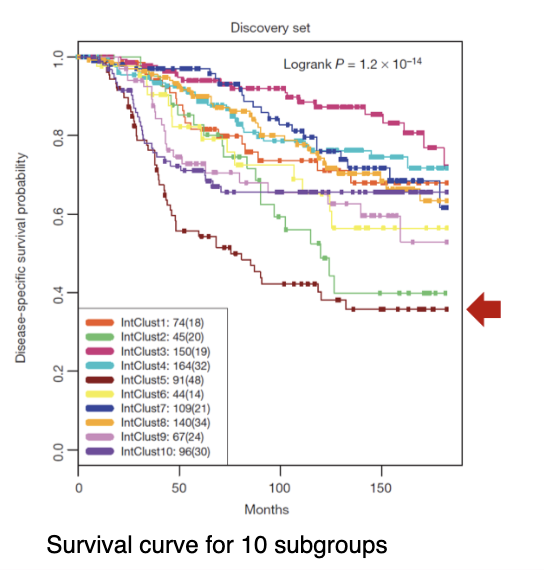
What characterises the high-risk breast cancer subgroup IntClust5?
High-risk group → poor prognosis, die quickly after diagnosis
Luminal tumours
ER-positive (ER⁺) but with additional tumour alterations
11q13/14 amplification (e.g. CCND1, EMSY)
Associated with steep mortality trajectory
Key idea:
Even ER⁺ cancers can be high risk if additional genomic alterations are present
Example: mutations/amplifications on chromosome 11q13 → worse prognosis
What is currently known about driver mutations in cancer from genome sequencing studies?
~140 genes (intragenic mutations) are known to drive tumorigenesis
Typical tumour has 2–8 driver gene mutations
Remaining mutations are passenger mutations
Driver genes are grouped into 12 signalling pathways
These regulate 3 core processes:
Cell fate
Cell survival
Genome maintenance
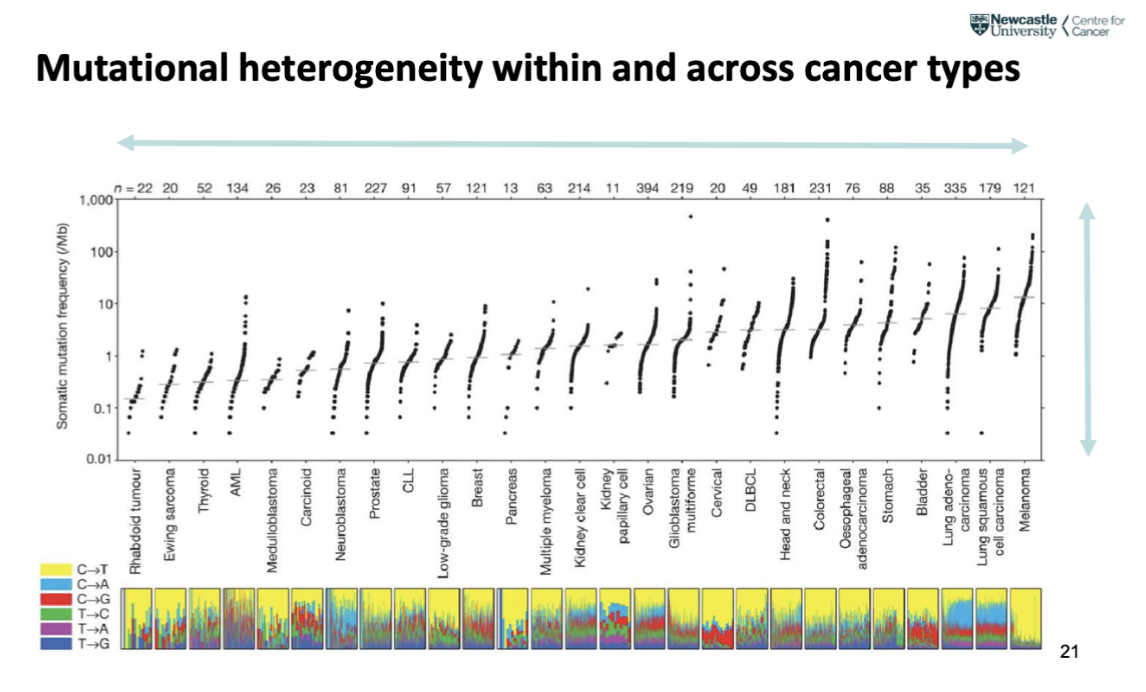
How do mutation burdens vary between different tumour types?
Tumours accumulate different numbers of mutations
Average ~90 mutant genes per tumour
Solid tumours: ~33–66 mutations
Examples: breast, prostate, pancreatic
Outliers: melanoma and lung cancers (~200 mutations)
Paediatric tumours & leukaemia: ~9–10 mutations
how can mutational heterogeneity within and across cancer types be presented
Each spot represents a patient where the average mutations read
Variation both across tumours and individuals- contribute to complexity and heterogeneity
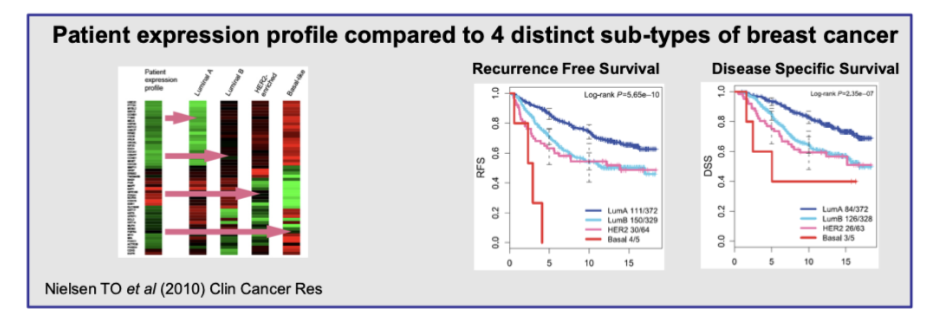
What molecular signature tests are used in breast cancer and how are they performed?
Breast cancer molecular tests:
RT-PCR (multiplex): PAM50, Oncotype DX, BCI
Microarray: MammaPrint, Curebest 95GC
PAM50:
50-gene signature for ER⁺ breast cancer
Used to predict response to tamoxifen therapy
Method:
RT-PCR on mRNA from FFPE (formalin-fixed paraffin-embedded) tissue samples
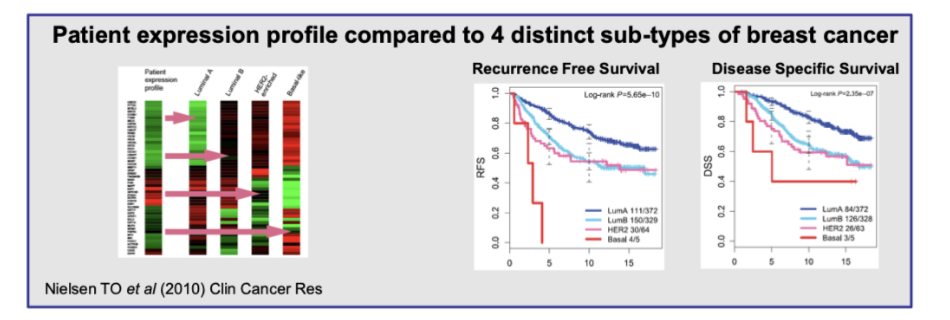
What is the clinical utility of PAM50 and molecular signatures in breast cancer?
Provides a prognostic score (0–100)
Predicts risk of recurrence (ROR) over 10 years
Compares patient gene expression to 4 breast cancer subtypes:
Luminal A
Luminal B
HER2-enriched
Basal-like
Correlates with outcomes:
Recurrence-free survival
Disease-specific survival
Enables individualised (personalised) treatment decisions
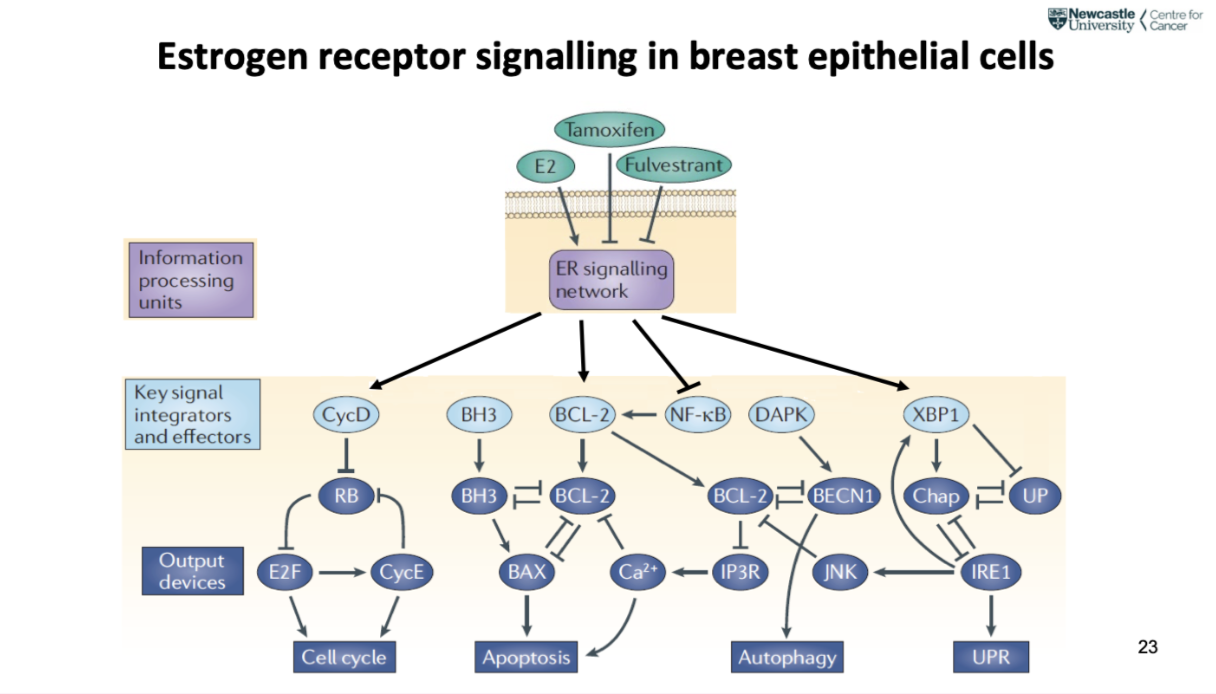
describe estrogen receptor signalling in breast epithelial cells
Estrogen (E2) activates ER → drives tumour growth (cell cycle progression)
Tamoxifen blocks ER, Fulvestrant degrades ER → inhibit signalling
ER signalling regulates:
Cell cycle (proliferation)
Apoptosis (BCL-2 vs BAX balance)
Autophagy & stress response (UPR)
Overall: ER network controls growth vs survival vs death of cancer cells
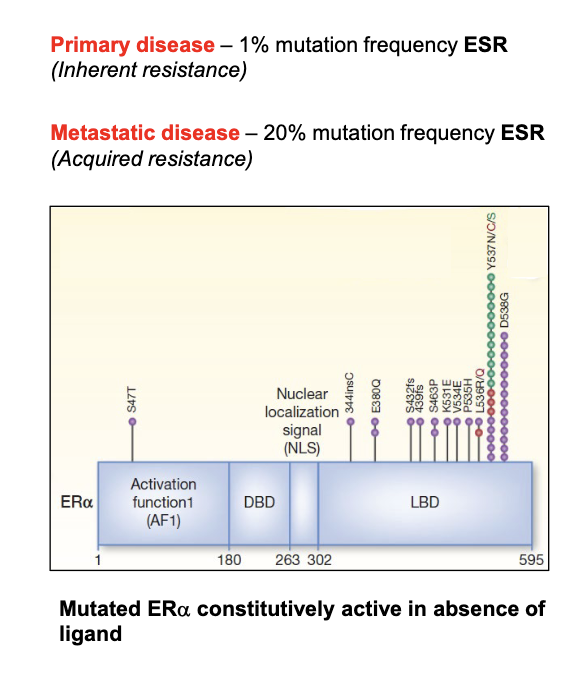
How do ER mutations cause resistance to endocrine therapy in breast cancer?
Mutations in ER (ESR gene) strongly drive signalling
Occur mainly in ligand-binding domain (e.g. Tyr537, Asp538)
Mutated ER is constitutively active without estrogen
Causes reduced sensitivity to anti-estrogens (tamoxifen, fulvestrant)
Higher drug doses needed for inhibition
Structural change → mimics active receptor conformation → drugs can’t properly block it
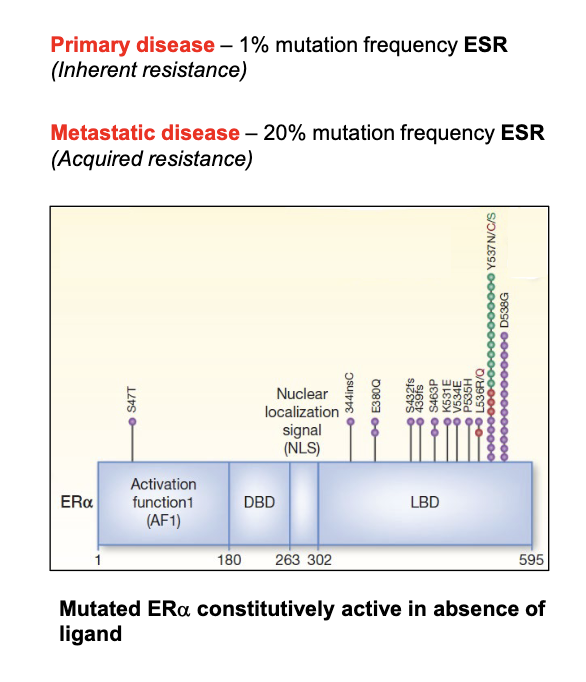
How do ER mutation frequencies differ between primary and metastatic breast cancer?
Primary disease: ~1% ESR mutation frequency (inherent resistance)
Metastatic disease: ~20% ESR mutation frequency (acquired resistance)
Indicates mutations are often selected during treatment
Explains why resistance develops over time
Key idea: mutated ER remains active even without ligand (estrogen) → therapy failure
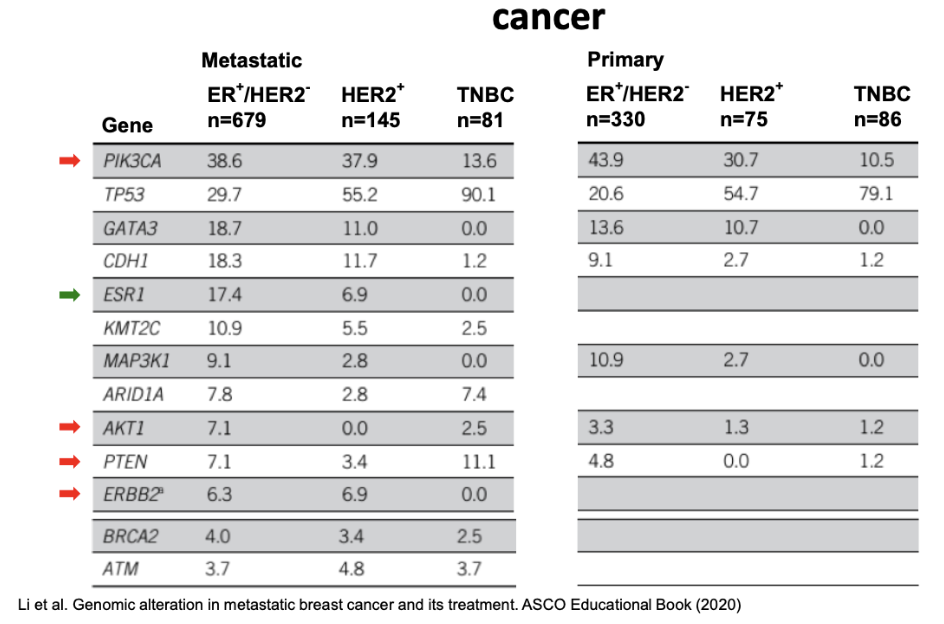
How does the genomic landscape differ between primary and metastatic breast cancer and why is this important?
Analysis of tumours can help when patient has become resistant, compare initial tumour vs altered tumour
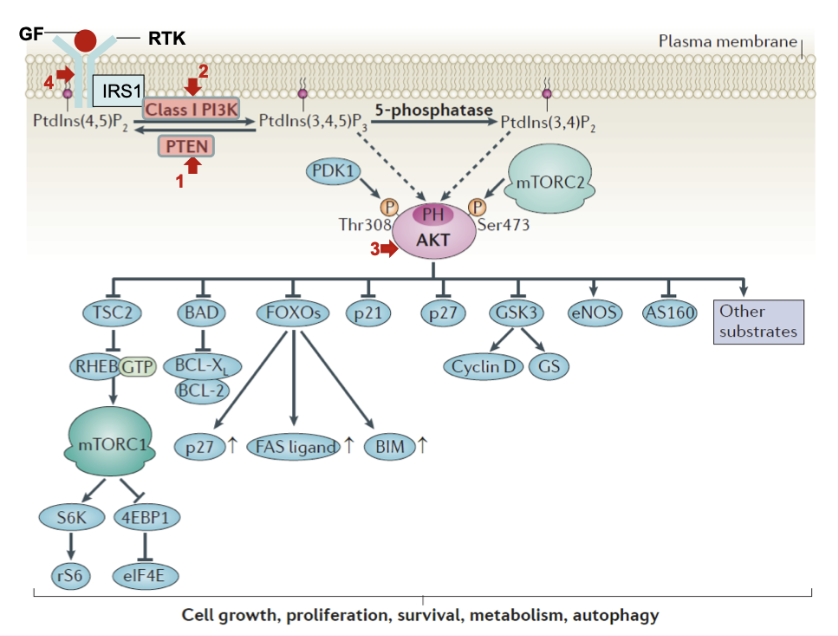
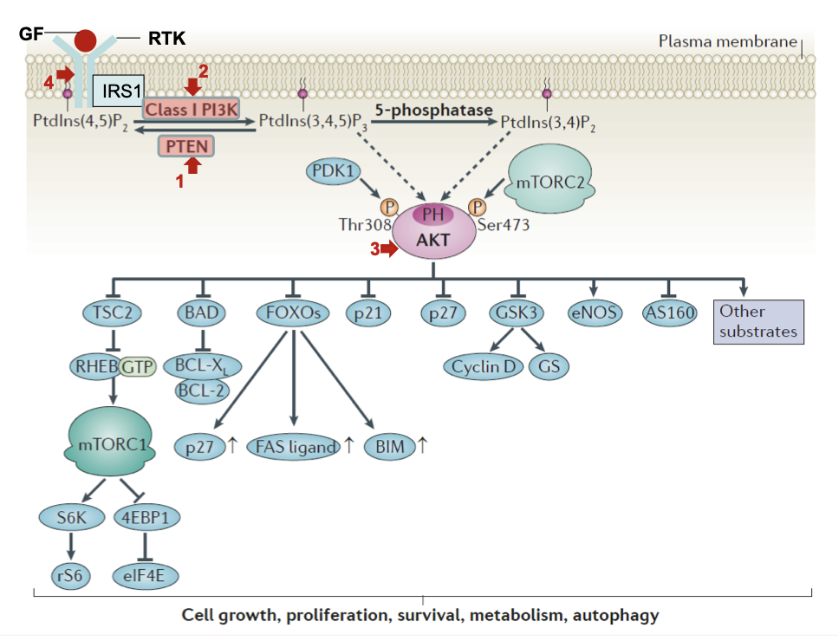
What are the key steps in the PI3K/AKT/mTOR signalling pathway?
Growth factor (GF) → RTK activation → IRS1 → PI3K activation
PI3K converts PIP2 → PIP3
PTEN opposes PI3K (converts PIP3 back to PIP2)
PIP3 recruits PDK1 and AKT
AKT activated by:
PDK1 (Thr308 phosphorylation)
mTORC2 (Ser473 phosphorylation)
Activated AKT acts as a central pro-survival and growth regulator
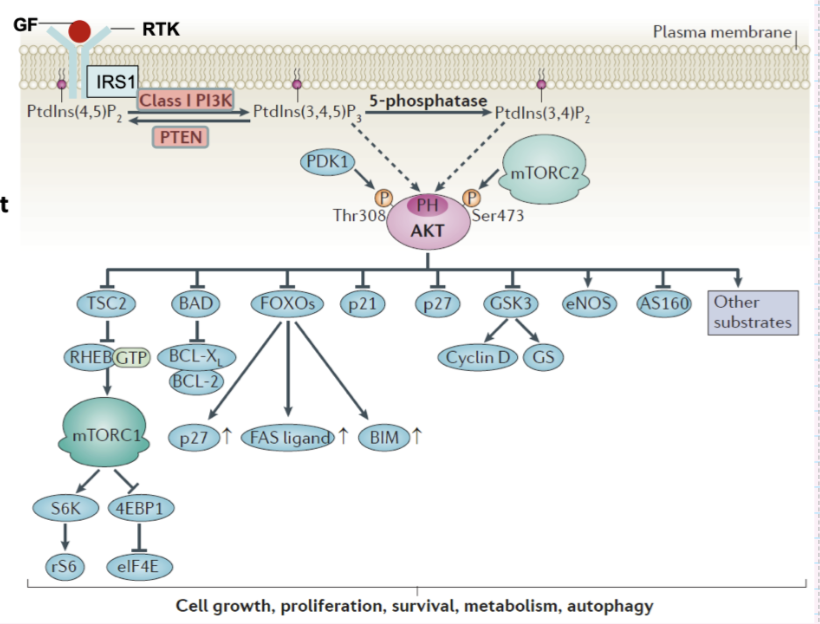
What are the downstream effects of AKT activation?
Promotes cell survival:
Inhibits BAD, FOXO → ↓ apoptosis (↓ BIM, FAS ligand)
Increases BCL-2/BCL-XL activity
Promotes cell growth & proliferation:
Activates mTORC1 (via TSC2/RHEB) → protein synthesis (S6K, 4EBP1, eIF4E)
Increases Cyclin D (via GSK3 inhibition)
Regulates cell cycle:
Inhibits p21, p27
Affects metabolism & other pathways (eNOS, AS160, etc.)
Overall: drives cell growth, proliferation, survival, metabolism, and autophagy regulation
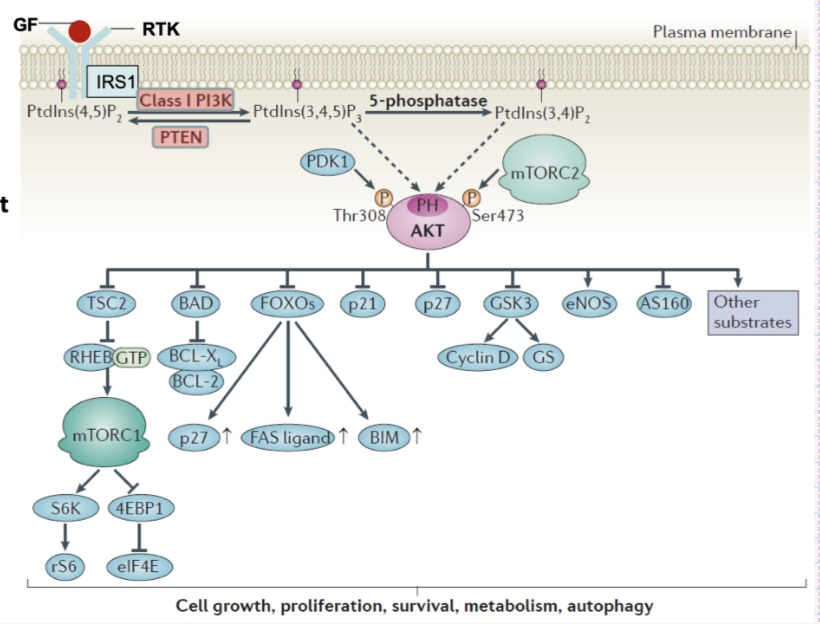
What additional regulatory steps and components fine-tune the PI3K/AKT/mTOR pathway?
Lipid conversions:
PtdIns(4,5)P2 → PtdIns(3,4,5)P3 (via PI3K)
PTEN reverses this
5-phosphatases convert PIP3 → PtdIns(3,4)P2
AKT recruited to membrane via PH domain binding to PIP3
TSC2 inhibits RHEB → regulates mTORC1 activity
Additional AKT targets:
eNOS, AS160, other substrates (metabolism, signalling)
Pathway tightly regulated at multiple levels (lipid, kinase, protein interactions)
What are the main driver mutations in PI3K signalling alterations in cancer?
PTEN deletion/mutations
PI3K activating mutations
AKT activating mutations
Upstream RTK activating mutations
What types of agents targeting PI3K signalling are in clinical trials?
Pan class I PI3K inhibitors
Isoform-selective PI3K inhibitors
Rapamycin analogues
Pan-PI3K–mTOR inhibitors
Active site mTOR inhibitors
AKT inhibitors
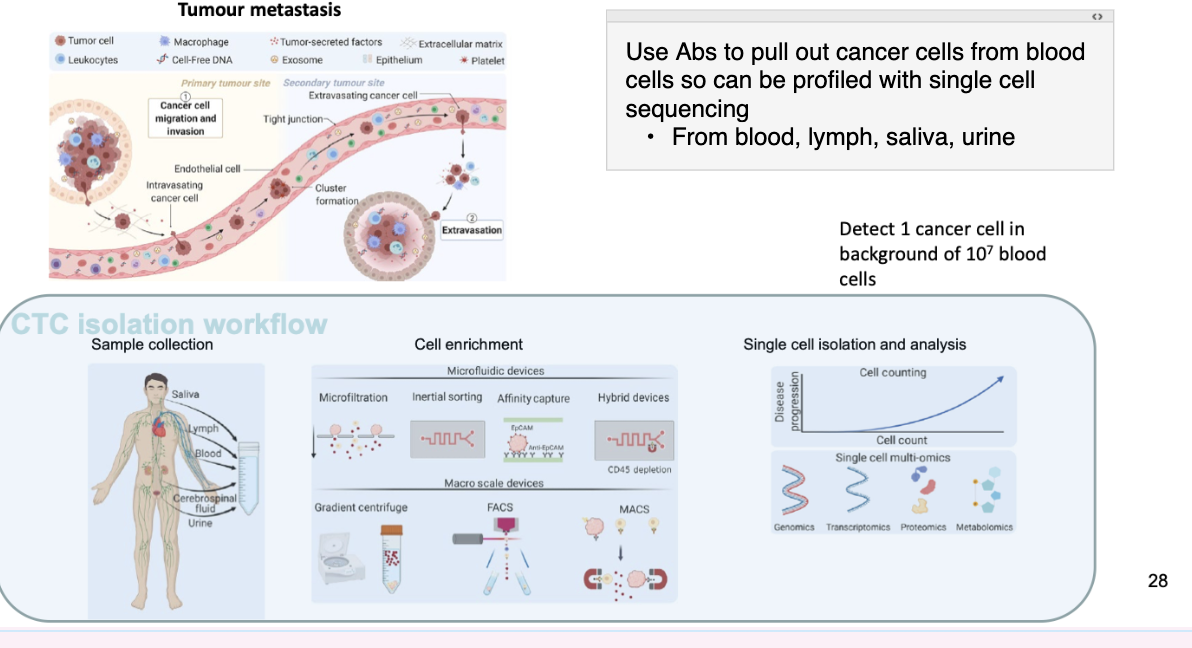
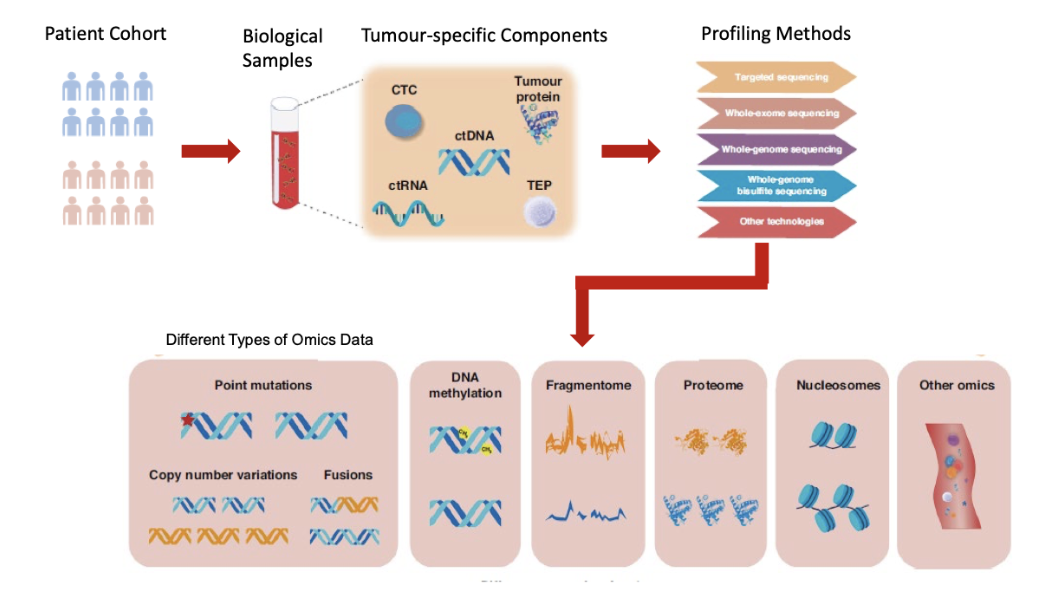
What are liquid biopsies and how do circulating tumour cells (CTCs) relate to metastasis?
Liquid biopsies detect circulating tumour cells (CTCs) to evaluate metastasis
Metastasis process:
Tumour cells invade primary site
Enter bloodstream (intravasation)
Travel and form clusters
Exit vessels (extravasation) → secondary tumour
CTCs provide a non-invasive way to monitor cancer spread
Can detect ~1 cancer cell among 10⁷ blood cells
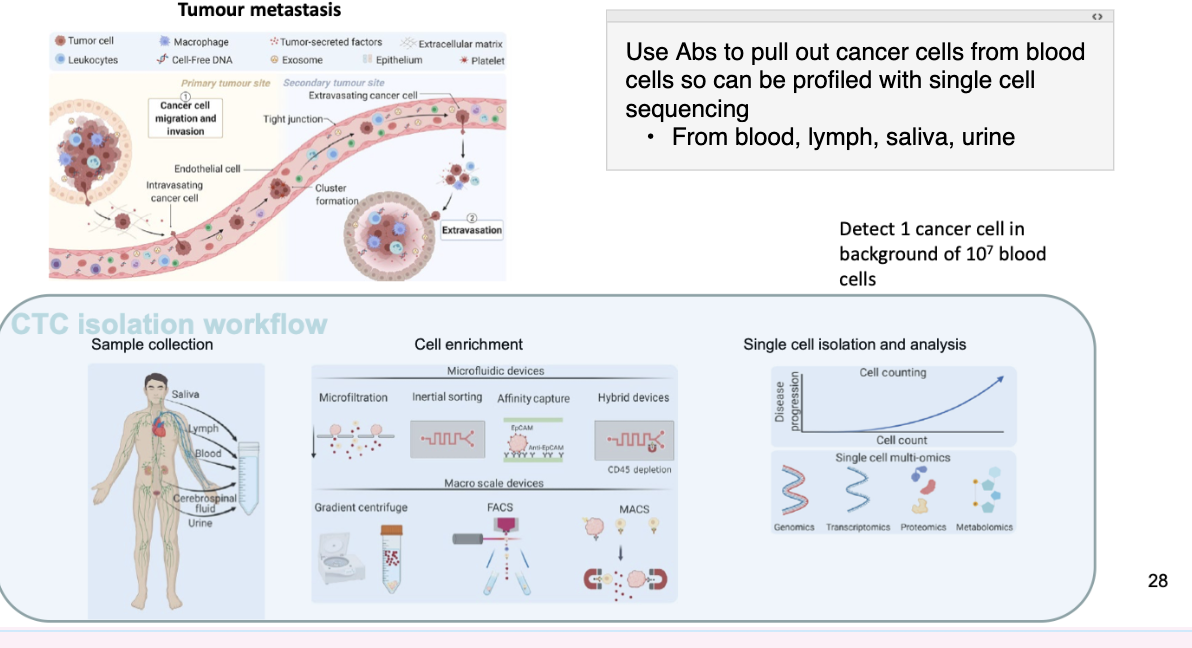
How are circulating tumour cells (CTCs) isolated and analysed in liquid biopsies?
Sample sources:
Blood, lymph, saliva, urine
Isolation method (your notes):
Use antibodies (Abs) to pull out cancer cells
CTC isolation workflow:
Sample collection (blood, lymph, cerebrospinal fluid, urine)
Cell enrichment:
Microfluidics (microfiltration, inertial sorting, affinity capture, hybrid devices)
Macro methods: gradient centrifugation, FACS, MACS
Single-cell isolation & analysis:
Cell counting (disease progression monitoring)
Multi-omics: genomics, transcriptomics, proteomics, metabolomics
Enables single-cell sequencing and profiling
why can cancer be studies from liquid biopsies
Can look at DNA from tumour cells in liquid
Cancer cells released into blood stream
When cancer cells they release DNA which enters the bloodstream (circulating tumour DNA)
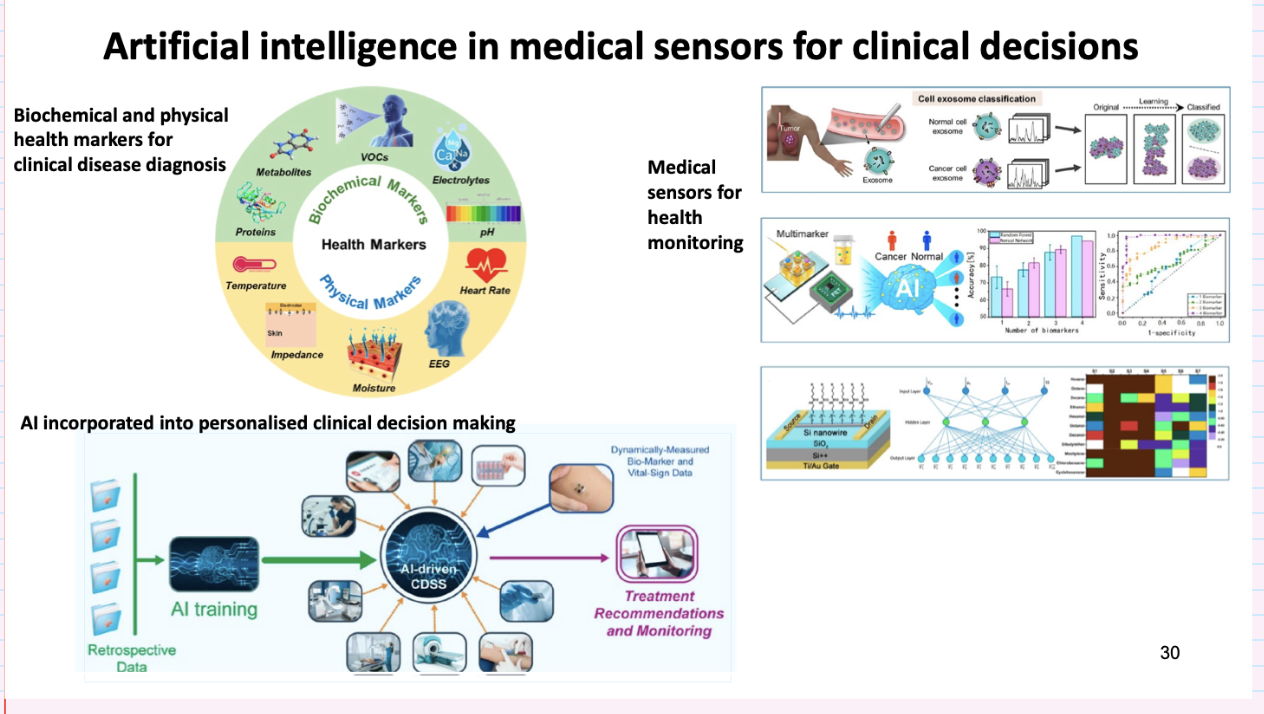
how can AI be used in medical sensors for clinical decisions
In pathology, with AI can look at 10s of thousands of samples in 24 hrs, overnight as well