Week 7 Content.
1/59
Earn XP
Description and Tags
Respiratory Investigations and Intro to Chest X-Rays
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
60 Terms
Respiratory Assessment- ABG Analysis
Arterial Blood Gas (first-line test): Evaluates gas exchange, lung +kidney function, acid-base status
Respiratory Assessment- Chest X-Ray
Diagnose lung/cardiac pathology, monitor progression
Tidal Volume (TV)
Volume of air in one breath (~500mL)
Minute Ventilation (MV)
MV = Respiratory Rate × TV (~6L/min)
Alveolar Ventilation (AV)
Air reaching alveoli (~4.2L/min)
Dead Space
inhaled air that does not participate in gas exchange -30% of air remains in conducting airways
Inspiratory Reserve Volume (IVR)
Volume of air able to inhaled over and above TV
Expiratory Reserve Volume (ERV)
Volume of air able to be forcefully exhaled after completion of respiratory cycle
Residual Volume (RV)
Volume of air remaining in lungs after maximum exhalation
Minimal Volume (MV)
Amount of air that would remain in your lungs if they were allowed to collapse
Inspiratory Capacity (IC)
Amount of air capable of being inhaled into lungs after completed respiratory cycle (TV+IRV)
Vital Capacity (VC)
Maximum amount of air that you can move into or out of your lungs in a single respiratory cycle (ERV+TV+IRV)
Functional Residual Capacity (FRC)
Amount of air remaining in your lungs after completing a respiratory cycle (ERV+RV)
Total Lung Capacity (TLC)
Total volume of your lungs (VC+RV)
Steps in Respiration (Gas Exchange)
Pulmonary Ventilation
External (Pulmonary) Respiration
Internal (Tissue) Respiration
Pulmonary Respiration
Consists of inhalation/exhalation
External Respiration
Gas exchange between alveoli and blood
Internal Respiration
Gas exchange between blood and tissue
Factors affecting Ventilation
Surface tension (Causes alveolar recoil, surfactant reduces surface tension= Respiratory Distress Syndrome)
Lung Compliance (High compliance = easy expansion, Low compliance = stiff lungs)
Diseases reducing compliance (TB, Pulmonary Oedema, ↓ Surfactant, Intercostal paralysis, Emphysema)
Airway resistance (bronchoconstriction ↑ resistance, bronchodilation ↓ resistance, (Asthma, COPD, Emphysema, CB))
V/Q Ratio (normally 0.8)
ratio of the amount of air reaching the alveoli per minute (V) to the amount of blood reaching the alveoli per minute (Q)
assesses the efficiency and adequacy of ventilation and perfusion
(normally 0.8)
Higher V/Q at Apex of Lungs- due to position relative to heart
Lower V/Q at Base of Lungs- due to positon relative to heart
↑ V/Q Ratio
↑ ventilation or ↓ perfusion
↑ O₂
↓ CO₂
Common in Pulmonary embolism and Emphysema
↓ V/Q Ratio
↓ ventilation or ↑ perfusion
↓ O₂
↑ CO₂
Common in Asthma, Chronic bronchitis, Pulmonary oedema
Dalton’s Law
Total pressure= sum of partial pressures
Atmospheric Pressure (760mmHg) Equation
=PN2 + PO2 + PH2O + PCO2 + Pother gases
PN2 = 597.4 mmHg
PO2 = 158.8 mmHg
PH2O = 3.0 mmHg
PCO2 = 0.3 mmHg
Pother gases = 0.5 mmHg
Factors Affecting Diffusion
Partial pressure gradient
Surface Area
Solubility
Diffusion Distance
Henry’s Law
Quantity of a gas that will dissolve in a liquid is proportional to the partial pressures of the gas and its solubility
Higher PP+Solubility= more gas staying in solution
Relationship between movement of O2 and CO2
O₂ = Alveoli → blood → tissues
CO₂ = Tissues → blood → alveoli
DLCO (Diffusion Capacity of Carbon Monoxide)
Measures gas transfer efficiency using carbon monoxide (Normal ≥80%)
Estimates transfer of oxygen from alveoli in your lungs to bloodstream
Factors ↑ DLCO
Polycythaemia
Asthma
↑ pulmonary blood volume
Alveolar hemorrhage
Factors ↓ DLCO
Any conditon affecting effective alveolar surface area:
Decrease of total lung area, e.g. restrictive lung disease
-Chronic obstructive pulmonary disease (COPD) - except asthma
-Pulmonary embolism
-Cardiac insufficiency
-Pulmonary hypertension
-Chronic heart failure
Oxygen Transport
98.5% bound to haemoglobin
Forms oxyhaemoglobin
Hb saturation depends on PO₂
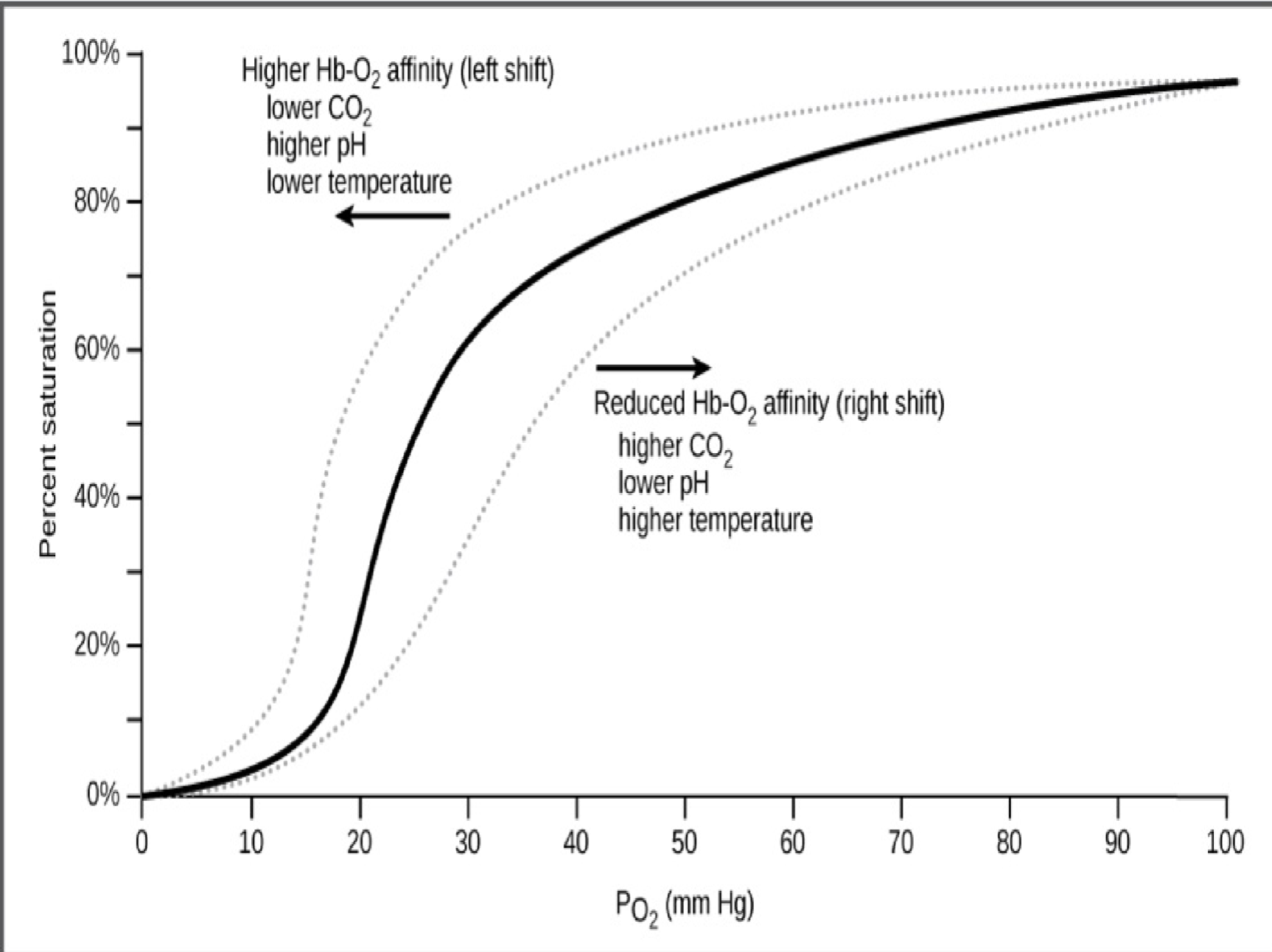
Oxyhaemoglobin Dissociation Curve
Demonstrates how easily Haemoglobin picks up and lets go of oxygen.
X-axis= PaO2- more oxygen avaliable as you move right
Y-axis= % saturation of haemoglobin (How “full” haemoglobin is with oxygen)
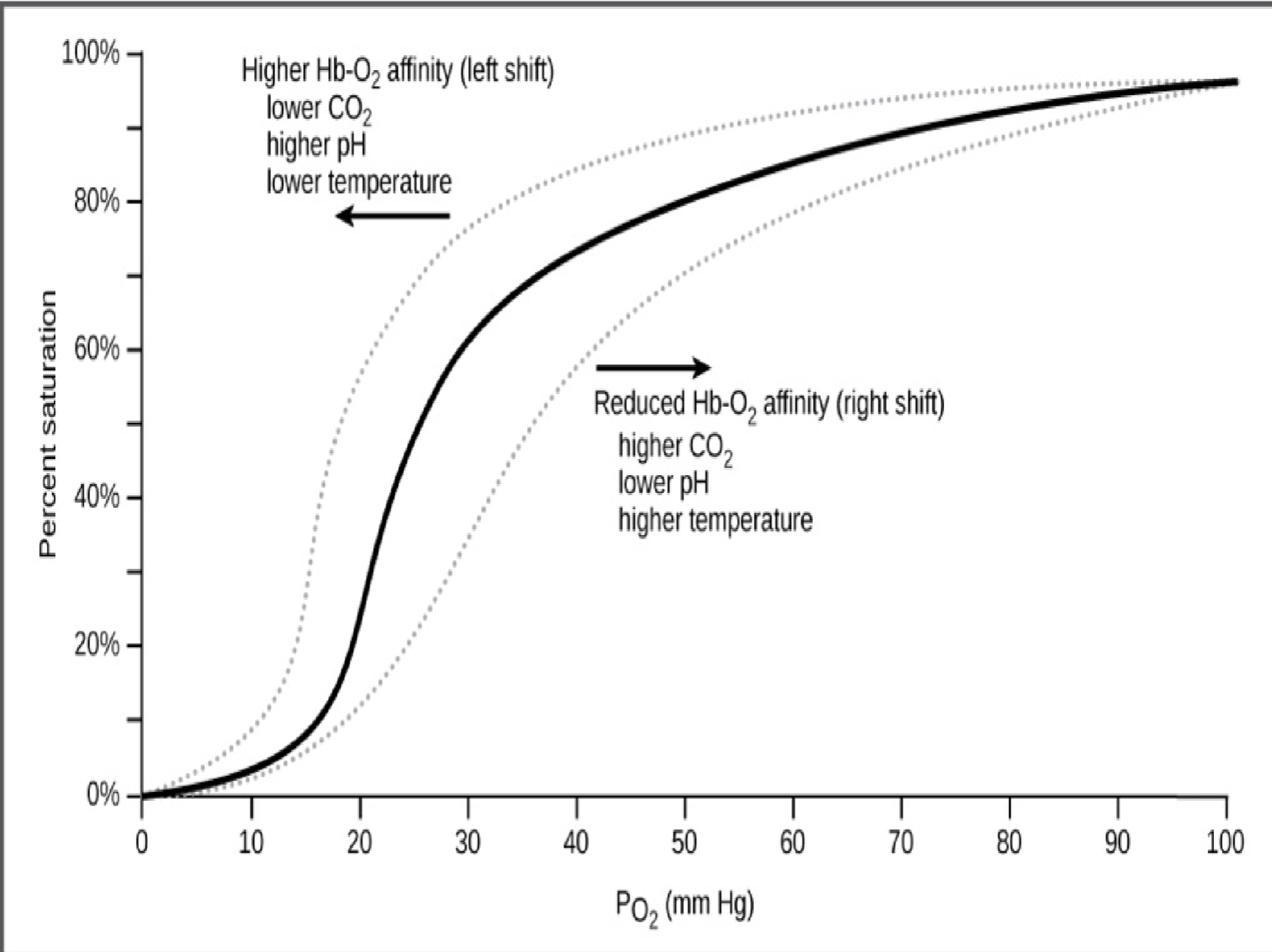
ODC- Left Shift
The curve moves LEFT when Hb has a higher affinity for oxygen (Hb grabs oxygen easily, does NOT want to let it go to tissues)
Caused by lower CO₂, Higher pH (less acidic), Lower temperature
Happens when body is more “resting” or calm
haemoglobin is MORE saturated → helps oxygen loading
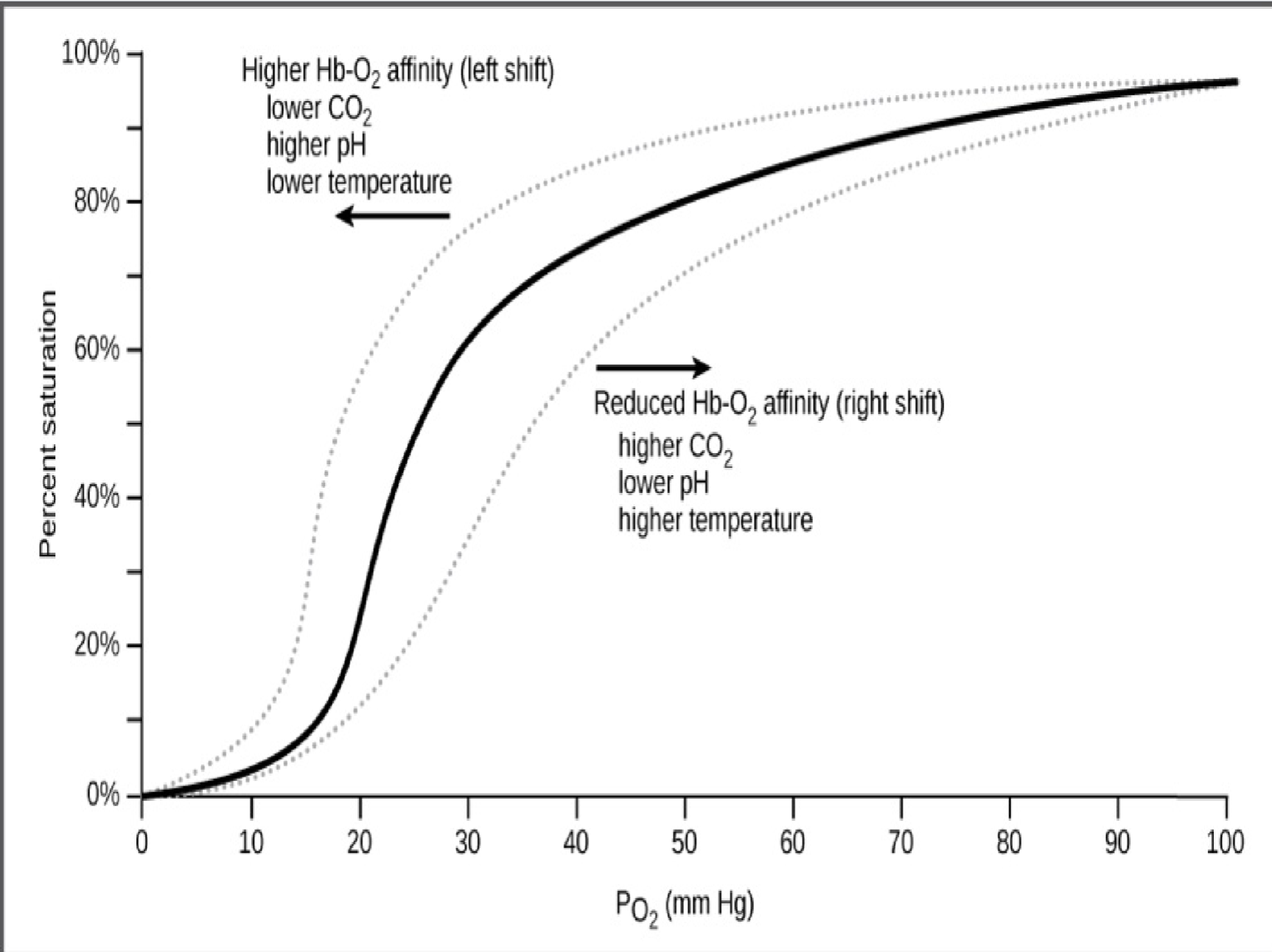
ODC- Right Shift
The curve moves RIGHT when Hb has a lower affinity for oxygen (Hb lets oxygen go more easily)
Caused by Higher CO₂, Lower pH (more acidic), Higher temperature
happens in active tissues like exercising muscle, fever, metabolically active tissue
These tissues need more oxygen → haemoglobin unloads oxygen there.
CARBON DIOXIDE TRANSPORT
7% dissolved in plasma
23% bound to Hb
70% as bicarbonate (HCO₃⁻)
Normal Acid-Base Balance
Normal pH = 7.35-7.45
Acidosis (acidaemia if refering to blood)
pH <7.35 (too acidic). Caused by increased CO2 → increased hydrogen ion concentration→ lowers pH
Alkalosis (alkalaemia if refering to blood)
pH >7.45 (Not acidic enough). Caused by reducing CO2 → decreases level of carbonic acid→raises pH
Blood Buffer Systems
Prevent rapid changes in pH by rapidly binding H+ ions
Made of weak acid and weak base
2 important systems: protein and cardonic acid-bicarbonage buffer systems
Protein Buffer System
Intracellular fluid and blood plasma
Albumin in blood plasma→ Functional groups of amino acids: Amines (base) and Carboxyl group (acid)
Hb within RBCs→ Buffers H+→Deoxyhemoglobin collects H+ to reduce acidity of RBCs
Carbonic Acid-Bicarbonate Buffer System
Bicarbonate ion- weak base
Carbonic acid- weak acid
Does not function when there is a shortage of CO2

Respiratory Regulation
↑ CO₂ or H+ →stimulates respiratory→increased ventilation→ exhales CO2→elimates excess acid
Hyperventilation ↓ CO₂
Hypoventilation ↑ CO₂
Fast response
Renal Regulation
Abnormal pH→kidneys conserve/eliminate H+ and carbonic acid
If acidotic = eliminates H+ and retains carbonc acid
If alkalotic = elimiates carbonic acid
Slow response
Central Chemoreceptors
In ventral sruface of medulla
Detect CO₂ via changes in pH
Peripheral Chemoreceptors
in carotid and aortic bodies
respond to changes in O₂, and CO₂ and pH
Ventilation Response to Carbon dioxide
CO₂ = main breathing stimulus- increases TV and Respiratory rate
Dueing exercise, CO2 production is increased but little to no change in PaCO2
PaCO2 set point buffered during COPD
Ventilatory response to oxygen
• arterial blood oxygen tension (PaO 2) less tightly regulated
• respiratory stimulation dictated by PaCO 2 prevents critical
falls in oxygenation
• signalling from carotid bodies increases as PaO 2 falls
• firing rates increase within seconds in range of 60 – 80
mmHg
• inflexion point for hypoxic ventilatory responsiveness
• coincides with beginning of steep portion of oxyhaemaglobin
dissociation curve
Acid Base disorders- Respiratory Acidosis
↑ PaCO₂ from hypoventilation
Low pH
-lungs (primary mechanism by which [H+] is adjusted)
Acid Base disorders- Respiratory Alkalosis
↓ CO₂ from hyperventilation
High pH
-lungs (primary mechanism by which [H+] is adjusted)
Acid Base disorders- Metabolic Acidosis
↓ bicarbonate or ↑ acid
Acid Base disorders- Metabolic Alkalosis
↑ bicarbonate
Respiratory Acidosis- Pathophysiology
Inadequate alveolar ventilation (CNS depression (stroke), medication depression, neuromuscular disorders, lung/chest infections, airway obstruction)
Overproduction of CO2 (hypercatabolic states e.g. sepsis)
Increased intake (Rebreathing CO2 containing gases, Insufflation of CO2 into body)
Respiratory Alkalosis- Pathophysiology
increased expiration and pH increases as less carbonic acid created
Causes: Central (head injury), hyperventilation (pain, panic), medication, pulmonary due to hypoxaemia (PE, altitude)
Ventilatory response to hydrogen ions
Increased H⁺ stimulates carotid bodies→Ventilation increases to reduce PaCO₂
Lower PaCO₂ raises pH and decreases central chemoreceptor stimulation.
This partly offsets increased ventilation and helps compensate for metabolic acidosis.
pH regulation has priority over PaCO₂ homeostasis.
Metabolic acidosis- Pathophysiology
Increases concentration of [H+] and reduces bicarbonate concentration. Caused by:
• lactic acidosis, ketoacidosis
• diarrhoea
• reduced renal acid excretion
Metabolic alkalosis- Pathophysiology
Loss of hydrogen ions, produces elevation of bicarbonate and pH. Caused by:
• vomiting
• hypovolemia
• diuretic use
• administration bicarbonate
Compensation
METABOLIC problem= Carbonic acid abnormality→ LUNGS change PaCO2
RESPIRATORY problem= PaCO2 abnormality→ KIDNEYS cahnge carbonic acid
(more HCO3= more alkaline, more CO2= more acidic)
Hypoxaemia- Pathophysiology
Defiency of oxygen in arterial blood
PaO2 <60mmHg
SaO2 <90%
Hypoxia- Pathophysiology
Reduced oxygen to the body or at specific tissues
6 Steps in ABG analysis and Interpretation
the pH normal? (7.35-7.45)- Normal (compensated acidemia if below 7.35)
the PaCO2 normal? (35-45mmHg)
the HCO3 normal? (22-26 mEq/L)
Match the CO2 or the HCO3 with the pH
Does the CO2 or the HCO3 go the opposite direction of the pH?
Are the pO2 and the O2 saturation normal?