Ex Phys Final
1/29
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
30 Terms
Cardiac Output
Q=HR*SV.
HR increases to peak VO2
Average person SV increases up to 40-60% VO2 max
endurance athletes can increase until VO2max
25 L/min at high intensity
Cardiovascular Drift
gradual increase in HR over time. With exercise SV decreases and is compensated for by HR.
Causes: increased skin BF, decreased BV, increased HR.
Heat and wind really matter.
What happens to HR and SV when going from supine to standing?
SV decrease, HR increase. Because of gravity, there is less venous return to less SV. HR increase to compensate and because you are moving.
HR
increases in proportion to VO2.
Max= 220-age
Limitations: medication (beta blockers blunt), fitness, age effect not linear, variability, 10-15 bpm error.
SA node= natural 80-100 bpm. Decreased PNS raises HR to 100-110 bpm, increased SNS raises HR from 100-110 to max.
HRV
heart rate variability. Used as a measure of ANS activity. Higher HRV is good because you are highly adaptable to change.
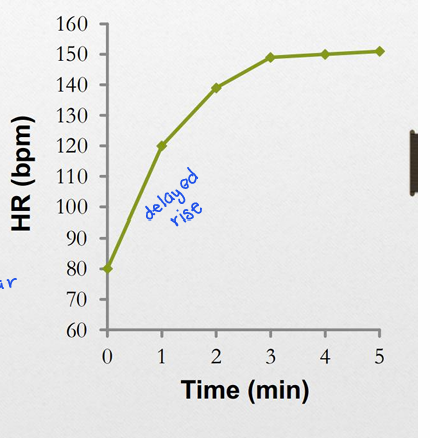
HR response to submax exercise
Delayed rise (like O2 deficit), steady state reached in 1-4 min.
SV will immediately rise (increased venous return, muscle and respiratory pumps)
How can athletes significantly increase their SV above sedentary individuals?
Larger muscles in the heart (left ventricle 5x bigger than right), increased contractility, decreased filling time as HR increases.
Frank-Starling Mechanism
Increased venous return=increased stretch=optimizes cross bridging=greater contraction.
increase in stroke volume during exercise (increased preload is good!)
How is SV regulated? what influences
filling (venous return)
ejection
contractility (SNS stimulates)
decreased afterload (decreased resistance)
Oxygen concentrations in blood during exercise
arterial is constant, venous varies by tissue.
a-vO2 difference: at rest 5 ml/100 ml, at max exercise 15-17 ml/100 ml
What does the CV system do during exercise (summary)
Increase CO (increase HR and SV)
Increase a-vO2 difference
Blood flow diverted from gut (vasoconstriction) to exercising muscle (vasodilation)
this is from intrinsic control (endothelial, myogenic, metabolic mechanisms)
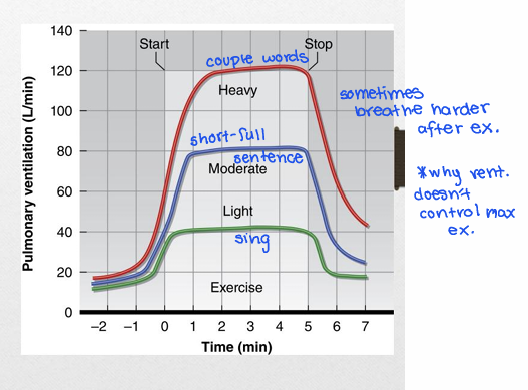
Ventilation during exercise
proportional to exercise intensity (delayed rise and recovery).
anticipatory response- heavier breathing before and at beginning of ex.
Light and moderate- increase tidal volume to 600-700 ml
Moderate and high- increase breathing frequency
ventilation doesn’t determine max exercise
Breathing Problems
Dyspnea- shortness of breath
Hyperventilation- excessive Ve
Valsalva maneuver- breathing against a closed glottis
increase intra abdominal pressure and intra thoracic pressure. Restricts venous return, decreasing CO (why you should breathe through lifts or hard activities)
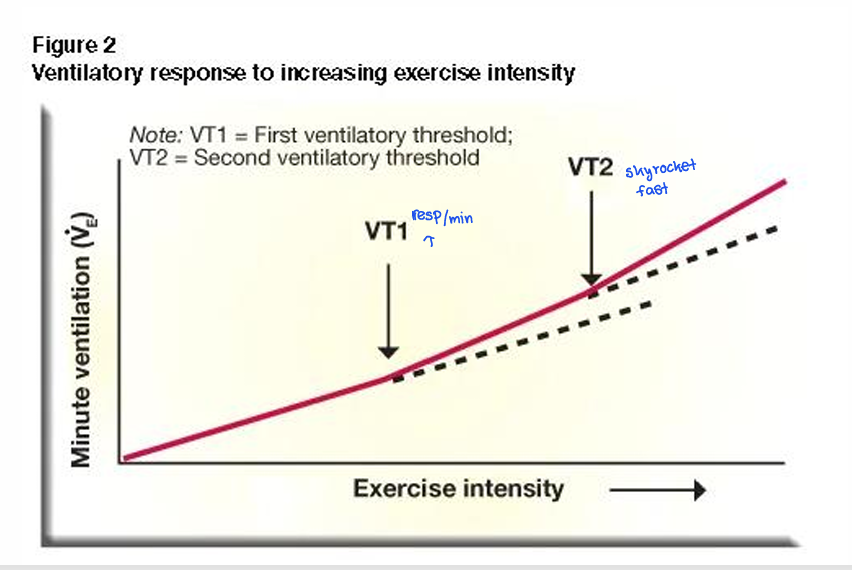
Ventilatory threshold
also known as anaerobic threshold. With increased intensity, Ve begins to increase greater than VO2. Occurs at about 55-75% of VO2 max.
Onset of involuntary hyper-ventilation (excessive production of CO2 due to HCO3 buffering of H+ from lactic acid)
Causes of VT
Temperature: increase in temp may stimulate respiratory control center (increase)
Hormonal: epi and NE may increase the sensitivity of arterial chemoreceptors to changes in PO2, PCO2, and pH
Mechanical: force and frequency of muscle contraction will be detected by sensory neurons (lower force, slower to VT)
Potassium: increases progressively with intensity, may stimulate arterial chemoreceptors (waste buildup-VT2 to clear)
Respiratory Muscles demands during ex
11% of CO during max or near max exercise (a lot of blood). Primarily type 1 fibers (oxidative, good endurance) 9-12% of VO2 post exercise (can increase breathing)
Lactate and muscle pH during high intensity
Lactate in muscle- clears in 30m, creating lactate in type II muscle faster than can get into blood stream (will be higher in muscle)
Blood- lactate levels lag behind, but will be higher for longer (delayed clearing)
Active recovery
effective- maintains blood flow to tissue, enhances removal of lactate, H+ and other metabolites from muscle
What variables/threshold need to be hit to truly determine if someone has reached their VO2 max
Max HR (w/in 10 beats)
RER 1-1.1
RPE >17
lactate levels (8mmol in blood)
above VT2→ plateau in O2 with increasing workload
Want to hit 3-hopefully 4
Isometric vs Isotonic vs Isokinetic
Isometric- ability to hold position or joint angle w/o movement under resistance. No lengthening or shortening.
Isotonic- muscle strengthening/lengthening at variable speed and joint angle. External resistance dictating muscle tension (same weight)
Isokinetic- same speed. Measuring how much torque at each speed.
Muscular strength vs endurance vs power
Strength- maximal force a muscle can generate. Ability to resist external forces.
Endurance- ability to exert force repeatedly against resistance, lower loads, more reps, longer durations. Increase resistance to fatigue
Power- rate at which work is performed (w/t, f*v). Explosive strength
Limits of aerobic and anaerobic power
Aerobic- rate of energy release by aerobic processes (krebs cycle, ETC) Capacity= VO2max. Limitation= cardiovascular system
Anaerobic- rate of energy release anaerobic process (PCr, glycolysis) Anerobic capacity=Wingate. Limitation= oxygen deficit (O2 consumed>demand, can’t clear substrate)
Epigenetics
how behaviors and environment can affect the way genes work and are expressed. Exercise, nutrition, sleep, where you live… possibly even disease prevention (ex decreases cancer risk). SAID principle for genes
Allostatic load
Allostatic=maintaining stability through change.
Allostatic load=cumulative physiologic effects of chronic stress
Periodization
a method of organizing your training that involves emphasizing different aspects of your fitness at different times.
Systematically changes one or more variables to keep training challenging. increase vol, decrease intensity
Periodization principles
progressive overload through periods (intensity increase or volume increase)
training goes from less specificity to more specificity in goal (build general fitness to more goal specific tasks)
planned recovery (good sleep, hydration→ planned periods of decreased volume or intensity)
Phases of periodization
Macrocycles: long term planning before a competition, usually a “where I want to be” spanning long time period (the goal)
Mesocycles: usually 1-2 month cycles involving higher volume training to push capacity with spurts of lower volume to avoid burnout (skill/performance development)
Microcycles: weekly training regimens- vol and intensity can change between mode or type of exercise based on focus (conditioning)
Fatigue
Exercise or non-exercise induced loss in total performance due to physiological factors.
coming off an injury and violating the Rule of Too. Tend to overestimate how important a single session is to training.
Need to account to accumulated fatigue
Peripheral Fatigue
impairments in muscle function distal to NMJ.
lactate, H+, metabolic waste build up, ATP depletion, glycogen depletion. Cross bridge inefficiency.
Chemical, ion, waste, bioenergetics. Mechanical
Central fatigue
Reduction in CNS ability to voluntarily control muscle contractions, reduced cortical motor output.
NT changes: serotonin accumulates, decreased CNS excitability. Fluctuation in motivation (excitability), increase in inhibitory NTs (GABA). Don’t know if RMP or activation threshold is changing.
ANS dysregulate- HRV changes
Reduced neural drive evident at max and sub max efforts
Potential, NTs