Final Exam Study Guide (Adult II) Part 2
1/302
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
303 Terms
What is overflow incontinence and what might cause it?
Overflow leads to dribbling urine; incomplete emptying of bladder leads to distention and urine leakage
Causes:
Urethra prolapse
BPH
Weak bladder muscles (like w/ diabetic neuropathy and spinal cord injury)
For a male reporting urinary incontinence, what should the nurse ensure has been performed?
Ensure prostate exam performed
The leakage of urine occurs in small amounts and is more frequent when the patient coughs.
Which information does the nurse provide to the patient about the disorder?
“This is called stress incontinence”
• “This is caused by weakness of muscles around the urethra”
• “This occurs when intraabdominal pressure exceeds urethral resistance”
Elderly female patient experiencing urinary incontinence. Which physiological change does the nurse expect to see in this patient?
Decreased muscle tone
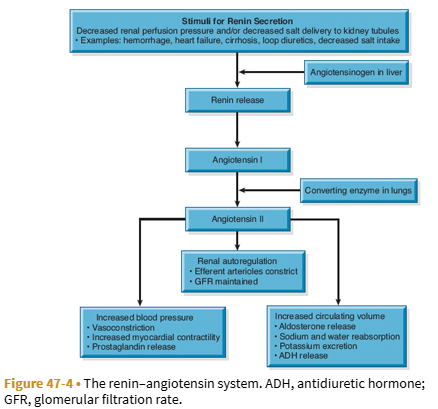
Explain the renin-angiotensin-aldosterone system
What is chronic kidney disease?
A progressive, irreversible disorder, and kidney function does not recover
—>In CKD, there is kidney damage or a decrease in glomerular filtration rate that lasts for 3 or more months
What does untreated chronic kidney disease lead to?
Untreated chronic kidney disease leads to end-stage renal disease (ESRD/ESKD), the retention of uremic waste products, and the need for renal replacement therapy or kidney transplantation
What are the 5 stages of chronic kidney disease based on?
Estimated glomerular filtration rate (GFR: the amount of plasma filtered through the glomeruli per unit of time.
List risk factors for chronic kidney disease
CV disease
Diabetes
HTN
Obesity
Glomerulonephritis
Pyelonephritis
Renal cancer
List s/s of chronic kidney disease
Lethargy
Seizures
Coma
HTN
Edema
Anemia
Muscle weakness
Muscle cramping
Metallic taste in mouth
Anorexia
N/V
Frost on skin (uremic frost)
Itching (pruritus)
Hiccups
What diagnostic labs/tests are used to evaluate a patient for chronic kidney disease?
Urine and serum lab tests
Kidney US or CT
List interventions for the management of chronic kidney disease.
Chronic kidney disease has a slow progression, so interventions include:
Control CV risk factors
Tx hyperglycemia
Manage anemia
Encourage smoking cessation
Weight loss (if obese)
Exercise
Reduce salt/alcohol intake
Education on minimizing nephrotoxins
Manage BP: Keep BP below 130/80
Early referral for initiation of renal replacement therapies
List pharmacologic interventions for the management of chronic kidney disease.
Calcium and phosphorus binders (OsCal, PhosLo, Renegel): To tx the calcium and phosphorous imbalance
Antihypertensive and CV Agents (Digoxin, Dobutamine, Diuretics): To tx HTN, HF, and pulmonary edema
Anticonvulsants: To tx neurologic abnormalities (Valium, Phytoin)
Erythropoietin (Epoetin Alfa): To tx anemia (we want hct of 33-38% and hgb of 12 g/dL); administered IV or subQ ; patients on erythropoietin will c/o of decreased levels of fatigue
Iron supplementation
What is acute nephritic syndrome?
A type of glomerulonephritis that causes inflammation of the glomerular capillaries
List risk factors for acute nephritic syndrome.
Recent infection, such as:
Acute viral infections (URIs, mumps, varicella, Epstein-Barr virus, Hep B, HIV)
Skin infection
Strep infection (of the throat)
Certain medications
List s/s of acute nephritic syndrome. Also list s/s of its more severe form, and s/s that could happen in older adults.
Hematuria
Edema
Proteinuria
Cola-colored urine
HTN
Anemia
Elevated BUN and creatinine (aka Azotemia—>high amount of nitrogen containing compounds in the blood like urea and creatinine)
More severe form:
HAs
Malaise
Flank pain
In Older Adults:
Dyspnea
Engorged neck veins
Cardiomegaly
Pulmonary edema
List diagnostic labs/testing to diagnose acute nephritic syndrome.
Serum lab tests—>elevated serum IgA level
Electron microscopy and immunofluorescent analysis to help identify the lesion
Kidney bx is needed for a definitive diagnosis
List interventions for the management of acute nephritic syndrome.
Management: Tx sx, preserve kidney function, and tx complications quickly (hypertensive encephalopathy, rapidly progressive glomerulonephritis, ESKD)
Corticosteroids (to control inflammation)
Antihypertensives (to control BP)
Antibiotic if the cause is strep A (penicillin)
Dietary restrictions (protein/sodium restriction)
What is nephrotic syndrome?
A disorder that occurs when renal and systemic diseases cause glomerular damage, which results in increased glomerular permeability to plasma proteins.
List causes of nephrotic syndrome
Massive proteinuria
Many kidney or systemic diseases that causes glomerular damage (i.e., diabetic neuropathy, lubpus, bacterial endocardidits)
List s/s of nephrotic syndrome.
Edema (usually pitting and/or periorbital, can also be sacral, abdominal, or in the legs/feet)
Irritability
HAs
Fatigue/Malaise
Proteinuria
Hypoalbuminemia
Hyperlipidemia
List diagnostic labs/tests to evaluate a patient for nephrotic syndrome.
Urine tests—>Proteinuria (especially high levels of albumin; levels >3.5 g/day)
Serum tests—>hypoalbuminemia (low blood albumin levels), hyperlipidemia (LDLs)
Kidney Bx necessary to confirm diagnosis
List interventions for the management of nephrotic syndrome.
Management is focused on addressing the underlying illness, slowing the progression of CKD, and relieving sx
Diuretics (to minimize edema)
ACE inhibitors (to reduce proteinuria)
Lipid-lowering agents (to tx hyperlipidemia—>statin meds)
Dietary sodium restrictions
What is acute kidney injury?
A rapid reduction in kidney function resulting in failure to maintain fluid-electrolyte and acid-base balances.
—>Can occur over a few hours or a few days
—>severity of AKI is based on increases in serum creatinine and decreased urine output
—>Severity of AKI is based on the RIFLE and KDIGO classification systems
List potential causes of acute kidney injury.
Prerenal Failure—>Caused by reduced kidney perfusion (hypoperfusion of the kidney)—>most common cause of AKI
Volume depletion resulting from: GI losses (emesis/diarrhea, NG suction), hemorrhage, renal losses (diuretic agents, osmotic diuresis)
Impaired cardiac efficiency resulting from: Arrhythmias, cardiogenic shock, HF, MI
Vasodilation resulting from: Anaphylaxis, antihypertensive meds/other meds that cause vasodilation, sepsis
Intrarenal Failure—>damage to kidney tissue/reflects injury to glomeruli, nephrons, and tubules
Prolonged renal ischemia resulting from: Hemoglobinuria (transfusion reaction, hemolytic anemia), pigment nephropathy (associated w/ breakdown of blood cells containing pigments that in turn occlude kidney structures), rhabdomyolysis/myoglobinuria (trauma, crush injuries, burns)
Nephrotoxic agents such as: Aminoglycoside antibiotics (gentamicin, tobramycin), ACE inhibitors, heavy metals (lead, mercury), NSAIDs, radiopaque contrast agents, solvents/chemicals (ethylene glycol, carbon tetrachloride, arsenic)
Infectious processes such as: Acute glomerulonephritis, acute pyelonephritis
Postrenal Failure—>caused by obstruction to urine flow
Urinary tract obstruction, including:
BPH
Blood clots
Calculi (stones)
Strictures
Tumors
List prerenal failure causes of AKI.
Prerenal Failure—>Caused by reduced kidney perfusion (hypoperfusion of the kidney)—>most common cause of AKI (so shock can cause prerenal failure/AKI)—>anything that causes massive fluid loss can cause prerenal failure
Volume depletion resulting from: GI losses (emesis/diarrhea, NG suction), hemorrhage, renal losses (diuretic agents, osmotic diuresis), severe burns
Impaired cardiac efficiency resulting from: Arrhythmias, cardiogenic shock, HF, MI
Vasodilation resulting from: Anaphylaxis, antihypertensive meds/other meds that cause vasodilation, sepsis
List intrarenal failure causes of AKI
Intrarenal Failure—>damage to kidney tissue/reflects injury to glomeruli, nephrons, and tubules
Prolonged renal ischemia resulting from: Hemoglobinuria (transfusion reaction, hemolytic anemia), pigment nephropathy (associated w/ breakdown of blood cells containing pigments that in turn occlude kidney structures), rhabdomyolysis/myoglobinuria (trauma, crush injuries, burns)
Nephrotoxic agents such as: Aminoglycoside antibiotics (gentamicin, tobramycin), ACE inhibitors, heavy metals (lead, mercury), NSAIDs, radiopaque contrast agents, solvents/chemicals (ethylene glycol, carbon tetrachloride, arsenic)
Infectious processes such as: Acute glomerulonephritis, acute pyelonephritis
List postrenal failure causes of AKI
Postrenal Failure—>caused by obstruction to urine flow
Urinary tract obstruction, including:
BPH
Blood clots
Calculi (stones)
Strictures
Tumors
List s/s of acute kidney injury.
Drowsiness
HA
Muscle twitching
Seizures
Increased BUN and creatinine (aka azotemia)—> significant increase in creatinine (especially if over a few hours or a couple days)
Oliguria (low urinary output; for adults urine output <400–500 mL/day or <0.5 mL/kg/hr)
Fluid overload
Dyspnea
Increased K+
Increased phosphorus
Decreased H&H
Decreased calcium
Increased magnesium
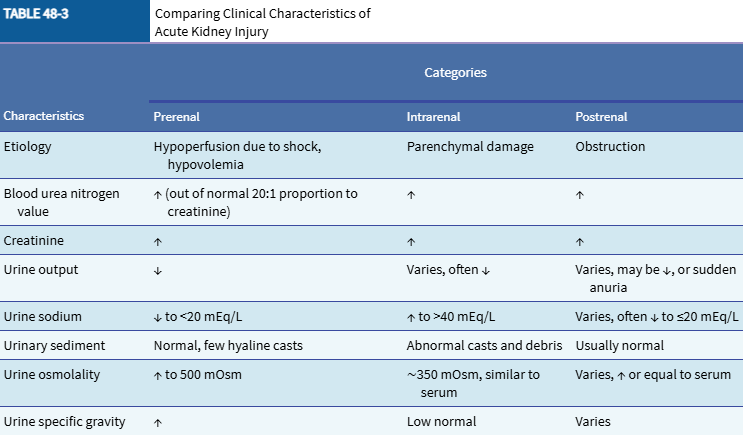
Differentiate prerenal failure, intrarenal failure, and post renal failure in the following characteristics:
Etiology
BUN value
Creatinine
Urine output
Urine sodium
Urinary sediment
Urine osmolality
Urine specific gravity
What pH crisis do patients with AKI experience?
Progressive metabolic acidosis
What is used in the diagnostic evaluation of acute kidney injury?
Serum blood tests
Urine tests
Imaging studies: U/S, CT, KUB x-rays, kidney biopsy
List interventions for acute kidney injury.
Eliminate the underlying cause (Prerenal, Intrarenal, Postrenal)
Maintain fluid balance
Avoid fluid excess
RRT if indicated
Nutritional therapy—>low in sodium, potsssium, and phosphorus, but higher in calories than standard feedings
Medications: Diuretics (used to increase urinary output), Calcium-channel blockers (used to tx AKI resulting from nephrotoxins)
What is hemodialysis/what is done during this? What is the purpose of hemodialysis? How common is it and how often is it performed?
Hemodialysis is a type of renal replacement therapy that removes medications or toxins from the blood, or for edema or hypertension that does not respond to other treatment
In hemodialysis, the blood is diverted from the client to a machine via the use of a blood pump to the dialyzer, where toxins are filtered from the blood, and the cleansed blood is returned to the client
Purpose of hemodialysis: Prevent death—>it does not compensate for the loss of metabolic kidney function
Intermittent hemodialysis (HD) is the most common renal replacement therapy (usually 3 times a week for 3-5 hours)
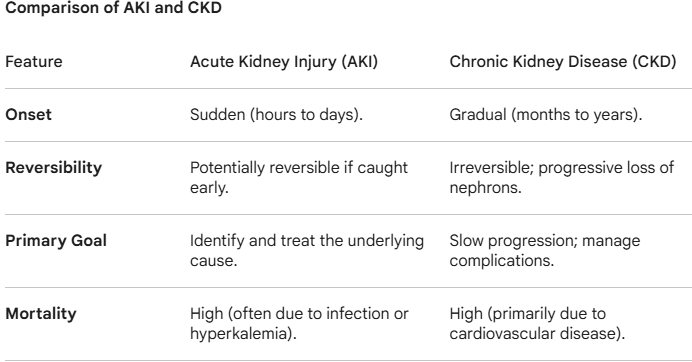
Compare AKI and CKD in the following areas:
Onset
Reversibility
Primary goal
Mortality
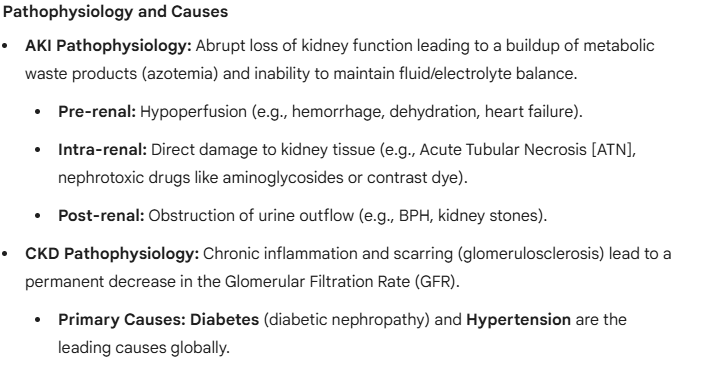
Differentiate the pathophysiology and causes of AKI and CKD
Differentiate the clinical manifestations of AKI and CKD
During hemodialysis, what is removed from the blood and how is it removed?
Toxins and wastes in the blood are removed by diffusion (large molecules blocked by semipermeable membrane—>i.e., RBCs, proteins)
Excess fluid is removed from the blood by osmosis
Ultrafiltration also helps to remove fluid and achieve fluid balance
What is required to perform hemodialysis?
Vascular access via:
Arteriovenous fistula: Joining an artery to a vein in the forearm; has the longest use capability and is the best option for vascular access
Arteriovenous graft: created b/t an artery and vein if the patient’s vessels are unsuitable for an AV fistula (connects using synthetic tubing
Central venous catheter
In what patients is hemodialysis immediately indicated?
Dialysis immediately for patients with
Fluid overload not responding to diuretics
Symptomatic hyperkalemia
Calciphylaxis (thrombosis and skin necrosis)
Symptomatic toxin ingestion (drug overdose or poisoning)
List nursing interventions for a patient undergoing hemodialysis.
Promote pharmacologic therapy—>heparin is usually admin to keep blood from clotting while in the dialysis circuit
Promote nutritional and fluid therapy
Meet psychosocial needs
Promote home, community-based, and transitional care
Protect vascular access
Detect cardiac and respiratory complications
Control electrolyte levels
Manage pain and discomfort
Prevent infection
Monitor for symptoms of uremia (Uremia is a dangerous, life-threatening condition defined as the buildup of urea and other nitrogenous waste products in the blood caused by severely damaged kidneys)
Sx of uremia include:
Extreme fatigue
Loss of appetite
N/V
Difficulty concentrating
HA
Weight loss
In advanced stages, confusion, coma, or seizures
What is uremia and list s/s.
Uremia is a dangerous, life-threatening condition defined as the buildup of urea and other nitrogenous waste products in the blood caused by severely damaged kidneys
Sx of uremia include:
Extreme fatigue
Loss of appetite
N/V
Difficulty concentrating
HA
Weight loss
In advanced stages, confusion, coma, or seizures
What is peritoneal dialysis (PD)? Where is the catheter placed? How is it different from HD?
A type of renal replacement therapy
In peritoneal dialysis, the peritoneal membrane serves as the semipermeable membrane that uses diffusion and osmosis; ultrafiltration occurs w/ PD by the dialysate fluid having a higher glucose concentration than blood
Uses a peritoneal catheter placed in the OR
Slower than HD
List the disadvantages of peritoneal dialysis
Protein loss in outflow fluid
Risk for peritoneal injury
Potential discomfort from indwelling fluid
Peritonitis
Bowel perforation
List the advantages of peritoneal dialysis
Flexible schedules
Less dietary and fluid restrictions
Better option for patients with severe HTN, HG, pulmonary edema, of older age, who have cardiovascular disease, or diabetes
Better for patients who cannot tolerate anticoagulation or who have poor vascular access
List possible complications of peritoneal dialysis
Peritonitis
Leakage at the catheter site
Bleeding
Abdominal hernias
Hemorrhoids
Low back pain
Anorexia
What is completed during peritoneal dialysis?
Toxins and wastes are removed from the blood by diffusion
Ultrafiltration occurs through an osmotic gradient created by using a dialysate fluid with a higher glucose concentration
What is the vascular access for peritoneal dialysis?
Peritoneal catheter
List interventions for the nursing management of a patient with peritoneal dialysis.
Meet psychosocial needs
Promote home, community-based, and transitional care
Protect vascular access
Monitor symptoms of uremia
Detect cardiac and respiratory complications
Control electrolyte levels
Manage pain and discomfort
Prevent infection
List/describe the types of lower UTIs.
Lower UTIs Include:
Bacterial cystitis (inflammation of the urinary bladder)
Bacterial prostatitis (inflammation of the prostate gland)
Bacterial urethritis (inflammation of the urethra)
About 50% of patients with indwelling catheters become infected within ____ of catheter insertion (cystitis)
1 week
List risk factors for the development of lower UTIs.
Female gender
DM
Pregnancy
Neurologic disorders
Gout
Immunosuppression
Instrumentation of urinary tract
Obstruction to urinary flow (i.e., kidney stones, ……)
Inability/failure to empty bladder completely
What is urethrovesical reflux, what is a complication of it, and what group is it more common in?
The backward flow (or reflux) of urine from the urethra into the bladder is known as urethrovesical reflux (an obstruction of free-flowing urine)
It brings bacteria into the bladder from the urethra
There is an increased incidence of urethrovesical reflux in postmenopausal women
What are the most common bacterial infection in women?
Community acquired UTIs
What are the most common organisms responsible for UTIs? What other organisms commonly cause lower UTIs (cystitis)
E-coli or other organisms found in the lower GI tract are the most common organisms responsible for UTIs
Other Common Organisms that Cause Lower UTIs:
Staphylococcus aureus
Kliebsiella pneumoniae
Proteus
Enterobacter
Fungal: candida
Trichomonas (rare)
Once an indwelling urinary catheter is placed, how long before bacterial colonization beings?
48 hours
What are the 3 ways that bacteria can enter the urinary tract? Which is the most common?
Transurethral route (ascending infection)—>most common route of infection, often from fecal contamination through the urethra or from sexual intercourse (forcing bacteria from the urethra into the bladder in women)
Through the bloodstream (hematogenous spread)
By an intestinal fistula (direct extension)
What is the most common factor that places clients at risk for UTIs in the hospital setting? Because of this, what is the goal to prevent these UTIs from happening?
Catheters
Remove the catheter w/in 48 hours after placement whenever clinically possible
List s/s of lower UTIs.
Burning on urination
Urinary frequency
Urinary urgency
Nocturia (waking up one or more times during the night to urinate, often resulting in disturbed sleep)
Incontinence
Suprapubic or pelvic pain
Hematuria
Back pain
What sx might a patient with a catheter associated UTI have?
Most catheter associated UTIs are asymptomatic
What labs/diagnostic tests are used to evaluate for lower UTIs?
Urine tests (i.e., UA, urine culture)
CT scan
US
Kidney scan
List interventions for the management of lower UTIs.
Antimicrobial agents
Urinary analgesic agents
Patient education (hygiene, increase fluid intake, voiding habits, wear cotton underwear)
How are UTIs diagnosed?
Urine cultures are frequently used to diagnose a UTI; can also identify the specific organism causing the infection = can choose effective antibiotic via C&S testing
On UA leukocytes, nitrites, bacteria, maybe hematuria
How common are upper UTIs compared to lower UTIs?
Less common than lower UTIs (has to travel further up the urinary tract)
List/describe the types of upper UTIs.
Pyelonephritis (inflammation of renal pelvis, tubules, and interstitial tissue)
Interstitial nephritis (inflammation of the kidney)
Kidney abscesses: A renal abscess is a localized collection of pus (infected fluid) within the kidney tissue (parenchyma) or in the surrounding space (perinephric space) = rare/severe complication of UTIs
What is the goal of tx of UTIs?
=Goal of treatment: an antibacterial medication that removes bacteria from the urinary tract without damaging the fecal and vaginal flora (minimizing vaginal yeast infections); meds that are affordable with few side effects
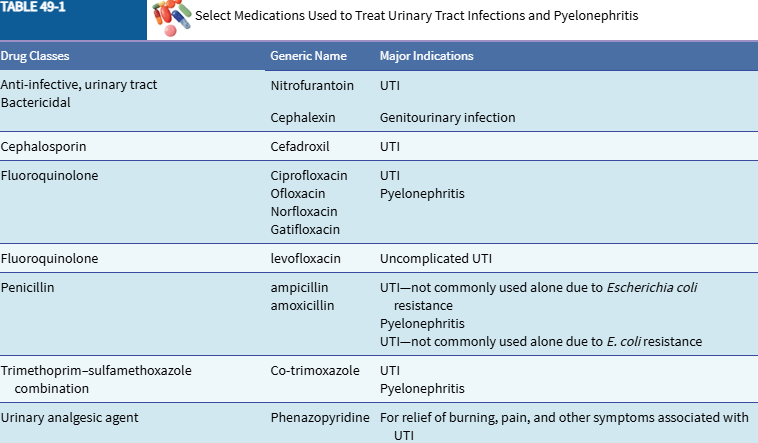
List drug classes with example meds used to tx UTIs and pyelonephritis
List patient education on preventing recurrent UTIs
Hygiene
Shower rather than bathe
Wipe from front to back after each BM
Fluid Intake
Hydrate well
Maybe 1 glass of cranberry juice daily
Avoid coffee, tea, colas, alcohol, and other fluids that are urinary tract irritants.
Voiding Habits
Void regularly (every 2-3 hours daily, fully emptying the bladder)
Women should void immediately after penile-vaginal intercourse
Interventions
Take medication exactly as prescribed
Keep in mind that if bacteria continue to appear in the urine, long-term antimicrobial therapy may be required to prevent colonization of the periurethral area and recurrence of infection
For recurrent infections, consider taking cranberry juice or capsules daily for longer than 8 weeks
If prescribed, test urine for the presence of bacteria following the manufacturer’s and health care provider’s instructions
Notify the primary provider if fever occurs or if signs and symptoms persist despite tx
Consult the primary provider regularly for follow-up
List age-related changes for men and women that increase risk of UTIs.
Both
Neurogenic (dysfunctional) bladder and indwelling catheters increases risk for UTIs
Women
Older women can have incomplete emptying of the bladder and/or urinary stasis
Postmenopausal women are more at risk of having bacteria in the vagina and urethra (can have recurrent cystitis from lack of estrogen; oral or topical estrogen can be used to restore the acidic pH of the vaginal area)
Men
Antibacterial activity of prostatic secretions that protect men from bacterial colonization of the urethra and bladder decreases with aging (catheterizations or cystoscopies that are used to diagnose urinary dysfunction, prostatic hyperplasia, or carcinoma increase the number of UTIs in men)
Most common cause of recurrent UTIs in older males is chronic bacterial prostatitis (resection of the prostate can help)
For UTIs, what sx are more common in older adults?
Incontinence
Delirium
Burning
Urgency
Fever
What is pyelonephritis?
A bacterial infection of the renal pelvis, tubules, and interstitial tissue of one or both kidneys
List causes of pyelonephritis.
The upward spread of bacteria from the bladder
Bacteria spread from systemic sources reaching the kidney via the bloodstream
An incompetent ureterovesical valve (= backflow of urine contaminated w/ bacteria)
Obstruction occurring in the urinary tract (bladder or prostate tumors, strictures, benign prostatic hyperplasia, and urinary stones)
Systemic infections (like tuberculosis)
How is pyelonephritis classified?
Pyelonephritis can be acute or chronic.
What is acute pyelonephritis?
An acute bacterial infection that leads to enlargement of the kidneys with interstitial infiltrations of inflammatory cells, tubular cell necrosis, and possible abscess formation (abscess = pocket of infection that can occur anywhere in the kidney)
Can also cause atrophy and destruction of tubules and glomeruli.
List s/s of acute pyelonephritis.
Chills
Fever
Leukocytosis
Bacteriuria
Pyuria
Low back pain
Flank pain
CVA tenderness
N/V
HAs
Malaise/fatigue
Painful urination
Tachycardia/tachypnea
Burning/urgency/frequency of urination
Nocturia
Recent cystitis or tx for UTI
What is used in the diagnostic evaluation of a patient for/with acute pyelonephritis?
Urine tests: Shows WBCs and bacteria; occasional RBCs & protein may be present; urine should b ecultured to determine causative organism
Serologic tests—>blood culture, c-reactive protein, erythrocyte sed rate to determine inflammation and/or cause of recurrent UTIs
US
CT scan
X-rays (KUB)
IV pyelogram
Radionuclide renal scan (identify active pyelonephritis or abscess in/around the kidney)
List interventions for the management acute pyelonephritis.
Antimicrobial agents (2-week course of antibiotics at least, may need for up to 6 wks for relapse)
Urinary analgesics
Hydration
Repeat urine culture 2 weeks after completion of antibiotic therapy
What is chronic pyelonephritis?
A condition caused from repeated episodes of acute pyelonephritis that result in scarred, contracted, and nonfunctioning kidneys
List s/s of chronic pyelonephritis.
Fatigue
HA
Poor appetite
Polyuria
Excessive thirst
Weight loss
HTN
Inability to conserve sodium = decreased urine concentrating ability (dilute + more urine) = nocturia
Tendency to develop hyperkalemia and acidosis
What is used in the diagnostic evaluation of a patient for/with chronic pyelonephritis?
Renal function tests—>BUN, creatinine clearance, creatinine levels
IV urogram
List complications of chronic pyelonephritis
ESKD
HTN
Kidney stones
List interventions for chronic pyelonephritis.
Antimicrobial agents (long-term prophylactic antimicrobial therapy to limit recurrence of infections)—>need to make sure meds are not nephrotoxic
Education focused on preventing acute infections
If hospitalized, careful monitoring of I&Os
3-4 L of fluids per day to dilute urine, decrease burning on urination, and prevent dehydration (unless contraindicated)
Assess vitals q4h; administer antipyretics and antibiotics as prescribed
Use NSAIDs appropriately; educate patient on reporting pain
Antibiotics to tx infection
Urinary antiseptic drugs (Macrodantin—>nitrofurantoin) to provide comfort
What is urinary incontinence?
Unplanned, involuntary, or uncontrolled loss of urine from the bladder
What raises the risk of urinary incontinence in women?
Age, gender, and number of vaginal deliveries are established risk factors for urinary incontinence in women
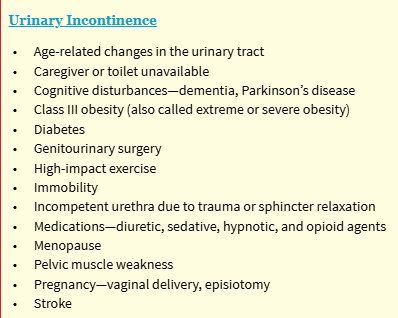
List risk factors for urinary incontinence
List the types of urinary incontinence.
Stress incontinence
Urge incontinence
Functional incontinence
Iatrogenic incontinence
Mixed incontinence
Overflow incontinence
Describe the pathology of stress incontinence, and explain what group is most often affected by this.
Most common type of incontinence
Loss of small amount of urine during coughing, sneezing, jogging, changing positions, jumping, or lifting
Cannot tighten the urethra enough to overcome the increased bladder pressure caused by contraction of the detrusor muscle
It predominantly affects women who have had vaginal deliveries. Thought to be the result of decreasing ligament and pelvic floor support or decreased/absent estrogen levels. In men, this can occur after a radical prostatectomy for prostate cancer.
List interventions for stress incontinence
Journaling, behavioral interventions, diet modification, pelvic floor (Kegel) exercises
Diet therapy
Drug therapy: Estrogen
Surgery
Vaginal cone therapy
What is urge incontinence? What is it also known as? What might cause urge incontinence?
The urge cannot be suppressed. The patient feels the urge but cannot hold it. (having bladder contractions regardless of the urine volume in the bladder)
Also known as overactive bladder
May have no known cause or may be the result of abnormal detrusor muscle contractions r/t other problems (from stroke, neurological problems, other urinary tract problems, irritation from concentrated urine-artificial sweetners-caffeine-alcohol-citric intake)
Drugs (diuretics) and nicotine can also irritate the bladder
List interventions for urge incontinence
Drugs: Anticholinergics, antihistamines, others
Diet therapy: Avoid caffeine and alcohol
Behavioral interventions: Exercises, bladder training, habit training, electrical stimulation
What is functional incontinence? What factors contribute?
• Occurs as a result of factors other than abnormal function of the bladder and urethra
• The lower urinary tract function is intact but other factors, such as cognitive impairment are not (Alzheimers)
List interventions for functional incontinence
Treatment of reversible causes
Urinary habit training (if incontinence not reversible)
Final strategy: Containment of urine, protection of patient’s skin
Applied devices
Urinary catheterization
What is iatrogenic incontinence? What resolves this type of incontinence?
• Involuntary loss of urine due to extrinsic medical factors, usually medications (alpha-adrenergic agents to decrease blood pressure like Doxazosin (Cardura), Prazosin (Minipress), and Terazosin (Hytrin))
• In people with an intact urinary system, these agents adversely affect the alpha receptors responsible for bladder neck closing pressure
• Has same characteristics as stress incontinence
• If medication discontinued, the incontinence resolves
List interventions for iatrogenic incontinence
Discontinue the medications that caused it
Treat the illness causing the need for medications
Kegel exercises
What is mixed incontinence? What group is this more common in?
The presence of more than one type of incontinence
Related to both stress and urge incontinence
Common in older women
What are common causes of the onset of urinary incontinence?
Acute UTI
Infection elsewhere in the body
Constipation
Decreased fluid intake
A change in a chronic disease pattern
Decreased estrogen levels
List causes of transient incontinence
Atrophic vaginitis, urethritis, prostatitis
•Delirium or confusion
•Excessive urine production (increased intake, diabetes, diabetic ketoacidosis)
•Limited or restricted activity
•Pharmacologic agents (anticholinergic agents, sedatives, alcohol, analgesic agents, diuretics, muscle relaxants, adrenergic agents)
•Psychological factors (depression, regression)
•Stool impaction or constipation
•Urinary tract infections (UTI)
What is used to diagnostically evaluate a patient with urinary incontinence?
Urine tests
Urodynamic tests
List nonsurgical/nonpharmacologic interventions for urinary incontinence.
Behavioral therapy is the 1st choice for tx urinary incontinence including:
Pelvic floor muscle exercises (Kegel exercises 4 times daily)
Voiding diary
Biofeedback
Prompted voiding (timed voiding that is carried out by staff or family members when the patient has cognitive difficulties that make it difficult to remember to void at set intervals)
Timed voiding (est set voiding frequency such as q2h if incontinent episodes tend to occur 2 or more hours after voiding = “void by the clock” at a given interval = void regularly every 2 hours)
PT
Avoid caffeine, alcohol, smoking
Bladder retraining (increasing voiding intervals as bladder strengthens)
Vaginal cone retention exercises (uses vaginal cones of varying weights)
Transvaginal/Transrectal Electrical Stimulation (using electrical stimulation to contract the pelvic floor muscles)
Neuromodulation (uses nerve stimulation to inhibit detrusor overactivity and hypersensory bladder signals, also strengthens weak sphincter muscles)
List pharmacologic therapies for urinary incontinence.
Anticholinergic agents = 1st-line meds for urinary incontinence (Levsin, Bentyl, HyoMax, Oxybutynin)
Alpha adrenergic agents
Tricyclic antidepressants can decrease bladder contractions + increase bladder neck resistance (amitriptyline, imipramine)
Pseudoephedrine sulfate acts on on alpha-adrenergic receptors, causing urinary retention, can be used to treat stress incontinence; this med needs to be used with caution in men with prostatic hyperplasia and patients with hypertension