Equine large intestine anatomy
1/52
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
53 Terms
Why do we see the GI issues we see with horses?
horses are trickle feeders and have evolved to continuously consume grass for most of the day
with modern domestic horses we’ve altered their natural behaviour, e.g. feeding twice a day, affecting their GIT
what are 2 challenged of a grazin diet?
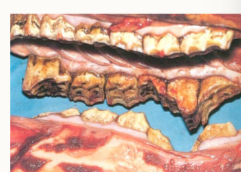
silicates in grass which are harder than enamel - wear down teeth
cellulose and hemicellulose require microbial fermentation
what 3 things will changing the diet affect?
number and type of bacteria
pH and conditions for VFA absorption
water balance
what do infrequent feeds cause (3)
decrease pH (due to sudden increased VFA production)
increase lactate
large influx of water
what can changes in bacterial flora cause (3)
enteritis
colitis
laminitis
what can breakdown of the mucosal barrier lead to?
septic peritonitis and death
what can changes in the water balance of the LI lead to?
impactions
what does the structure of the equine teeth enable?
grinding and rotational chewing movement - consider the drastic effect of there being a missing tooth
where does the first amount of liquid come from in the GIT?
the saliva
important for swallowing and lubricating food and buffering stomach acidity
why can’t horses vomit?
their muscular cardiac sphincter prevents reflux
what is an oesophageal obstruction known as?
choke
give 3 reasons for choke
dry food - sugar beet
inadequate chewing - dental disease
unsuitable food
what are the 2 regions of the equine stomach?
glandular epithelium
squamous epithelium
what separates the two regions in the equine stomach?
margo plicatus
function of the equine glandular epithelium?
secretes hydrochloric acid, pepsinogen and mucous
what are stomach ulcers?
areas where the acid from the glandular region has caused damage to the squamous epithelium
this occurs in particular with horses that are only fed at set times - the stomach produces acid continuously!
does the SI have a fixed position?
no, only attached by the long mesentery, no specific position/rotation
what carbohydrate can’t be digested in the small intestine?
fructans
cellulose
hemicellulose
common diseases of the equine SI? (5)
parasites
diarrhoea
impactions
twists/strangulations
infiltrative bowel disease
what does infiltrative bowel disease look like on an ultrasound, what can we describe it as
where there should be smooth mucosa, there’s bumps, due to infiltration of immune cells
it’s a malabsorptive disease
function of the caecum?
major for microbial digestion of cellulose
controls entry of ingesta into the large intestine
pacemaker for peristalsis and motility of the large intestine
describe the gross appearance of the caecum?
has sacculations and taenia
it’s a blind ending sac which is on the ventral abdomen of the horse - the first organ you’ll find during surgery
how much water is exchanged across the large intestine a day?
around 100 litres
with 100 litres being exchanged between the large intestine and blood stream daily, why is it not a good idea to feed a horse only a couple of times a day?
because this causes this huge volume of water to be exchanged in a very short period of time → problems
Describe the structure of the ventral colon
sacculations and taenial bands
why does the ventral colon have sacculations?
to increase surface area
why does the ventral colon have taenial bands?
important for mixing and moving the ingesta

Which parts of the colon can we visualise?
large part = dorsal, because this has no sacculations
smaller part/where you can visualise the sacculations - this is where the ventral colon is
function of small colon
storage of faeces and absorption of remaining water
concern/potential diagnostic issue with the small intestine?
narrow diameter → can get impactions
when palpating a horse what should we feel in terms of taenia/other structures
2 on the caecum
LDC and pelvic flexure is smooth
anti-mesenteric taenial band of small colon is palpable
what are the 2 kinds of colic
medical
critical - often needing surgery
what are the 3 steps to approaching a colic horse?
history
physical examination
diagnostic techniques
what 3 main diagnostic techniques will we choose for a colic horse?
rectal palpation
nasogastric intubation
abdominal paracentesis
what information do we want to gather for the colic horse in terms of history?
diet
anatomical predisposition
infection
parasites
ulceration
other organs/systems giving false signs of colic
what key physical examination aspects do we want to focus our physical examination on
overall impression of horse
demeanour
degree of pain
any self trauma
abdominal distension
posture
What aspects will we focus on in the clinical examination
TPR
pulse and mucous membranes - focusing on quality, mucous membranes, colour, refill time + digital pulse
GI sounds
abdominal distension
skin turgour
what additional diagnostic tests can we do, but that are not the key ones for colic?
ultrasonography
blood sample - hydration, infection, biochemistry, electrolytes
faecal examination
endoscopy
radiograph
what should we feel per rectum examination on the LHS
spleen
caudal pole of left kidney
pelvic flexure
small colon
what should each of these feel like on rectal palpation?
spleen
caudal pole of left kidney
pelvic flexure
small colon
smooth, sharp border, no palpable masses
smooth margins against spleen
variable diameter, no sacculations, no taenial bands palpable, indentable contents, move across to midline
small diameter, two taenial bands, faecal balls
what should we feel per rectal examination on the RHS
caecum
what should the caecum feel like on rectal palpation?
large diameter, gas, feed, fluid contents, saculations
caudal and medial taenial band dorsoventrally (often caudodorsal to cranioventral)
why is nasogastric tubing an option in horses?
if horses get an obstruction → gas/fluid build up iin stomach → expansion → rupture
horses can’t vomit
why may we use a nasogastric tube?
horse unable to vomit
removal of liquid reflux
detect gastric impaction
relieve choke
administer oral fluid/treatment
what is a peritoneal tap?
getting fluid from the space around the intestines
may be useful in chronic colic and critical cases to gauge how the intestines are functioning
what do we analyse with peritoneal tap?
colour
volume
turbidity
total protein
cell number and type
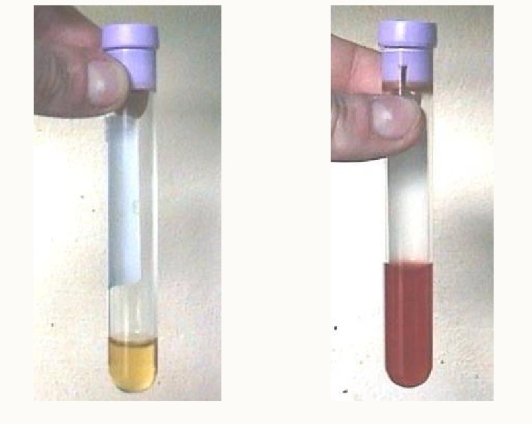
Which peritoneal tap sample is normal vs abnormal?
LHS = normal = yellow/clear, transparent
RHS = abnormal, red indicates potential necrosis/inflammation of small intestine
when may we use ultrasonography vs rectal examination?
small horses/ponies
foals
what information can we obtain from an ultrasound
provides extra information in adult animals
key diagnostic for colic - help identify enlargement of intestines
where do we listen to the gastrointestinal sounds in horses?
on the side of the animal
RHS - upper and lower parts of the caecum
LHS - upper and lower parts
why do we need to be careful with rectal examination?
can easily cause damage to the rectum
how do we check if there’s damage to the rectum post exam?
check on the back of our glove
especially the back of our hand - as dorsal damage to the rectum is the most common