Lecture 8: OMT for Cardiovascular Disease/Problems
1/41
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
42 Terms
1. Biomechanical model
2. Respiratory-Circulatory model
3. Neurologic model
4. Metabolic-Energy model
5. Behavioral model
what are the 5 physiologic models?
Biomechanical Model
• The structural model and the structural exam is the basic approach we have been teaching you
• This approach may change depending on many patient variables
• Posture and balance
• Motion
• Functional anatomy
• Tensegrity
Respiratory-Circulatory Model
• This is the model we consider when we feel that increasing movement of fluids would be helpful
• Sprained ankle, respiratory illness, pedal edema in CHF, etc
• Getting nutrients to and removing waste products from organs
• Respiratory mechanics
• Junctional areas are key sites
Respiratory-Circulatory Model
Goal of this model is to facilitate venous and lymphatic drainage and help the body mobilize and ultimately remove excess fluids
Cervicothoracic (diaphragm) Fascia
the fascia that covers the thoracic inlet
Sibson's Fascia
-thickened endothoracic fascia above the 1st rib to C7 transverse process (covers the apex of lung, which is prone to injuries)
-final area for obstruction of 2 great lymphatic ducts
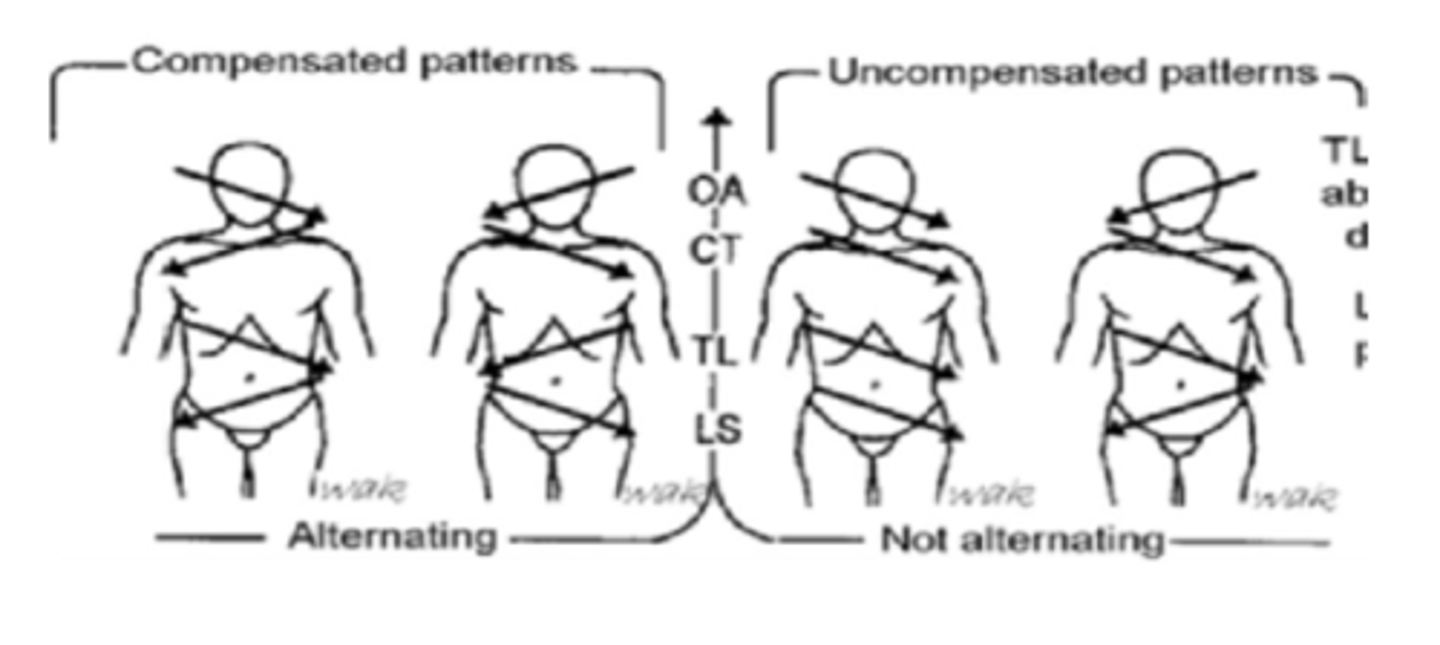
Zink's Common Compensatory Patterns (CCP)
Neurologic Model
goal of this model is to de-facilitate viscerosomatic reflexes to help restore parasympathetic dominance to the autonomic nervous system
Parasympathetic
The preferred homeostatic state of the cardiovascular system is under _____________________ dominance.
Sympathetic
Sympathetic or Parasympathetic:
• Decreased coronary blood flow
• Decreased time for diastole
• Cardiac remodeling
• Impaired lymph drainage
Sympathetic
Sympathetic or Parasympathetic:
• Increased catecholamines
• Increased inotropy
• Increased chronotropy
• Increased blood pressure
• Increased O2 demand
Parasympathetic
Sympathetic or Parasympathetic:
• Decreased inotropy
• Decreased chronotropy
• Decreased blood pressure
Parasympathetic
Sympathetic or Parasympathetic:
• Increased coronary blood
flow
• Improved lymph drainage
• Myocardial stabilizing
T1-4
sympathetic innervation to head and neck
T1-6
sympathetic innervation to heart and lungs
T2-8
sympathetic innervation to upper extremities
T5-9
sympathetic innervation to upper GI
T10-11
sympathetic innervation to lower GI
(small intestines, right colon), adrenals, kidneys (include T12), upper ureters, gonads
T11-L2
sympathetic innervation to lower extremities
T12-L2
sympathetic innervation to lowest GI
(left colon), GU (lower ureter, bladder, uterus/prostate, genitals)
Vagus Nerve
Parasympathetics for:
-Heart
-Bronchial Tree
-Esophagus (lower 2/3rds)
-Small Intestine
-Liver
-Gallbladder
-Pancreas
-Kidneys & upper ureter
-Ascending and transverse colon
Pelvic Splanchnics
Parasympathetics for:
-Descending and sigmoid colon, rectum
-Bladder wall and sphincter
-Lower ureter
-Uterus & prostate
-Ovaries & testes
-Genitalia
directly posterior
(tips in the same plane as transverse processes)
location of spinous processes of T1, 2, 3, and 12
pointed slightly downward
(tips in plane that is halfway between own transverse process and the one below it)
location of spinous processes of T4, 5, 6, and 11
pointed downward
(tips are one transverse process level below)
location of spinous processes of T7, 8, 9, and 10
Spinal Facilitation
Self-sustaining loop including the sensory afferents in the periphery, spinal cord interneurons, and either the somatic ventral horn motor neurons or the autonomic lateral horn motor neurons via the sympathetic chain ganglia and white rami communicants
Spinal Facilitation
1. The maintenance of a pool of neurons in a state of partial or subthreshold excitation; in this state, less afferent stimulation is required to trigger the discharge of impulses
2. A theory regarding the neurophysiologic mechanisms underlying the neuronal activity associated with somatic dysfunction.
3. may be due to sustained increase in afferent input, aberrant patterns of afferent input, changes within the affected neurons themselves, or changes in their chemical environment
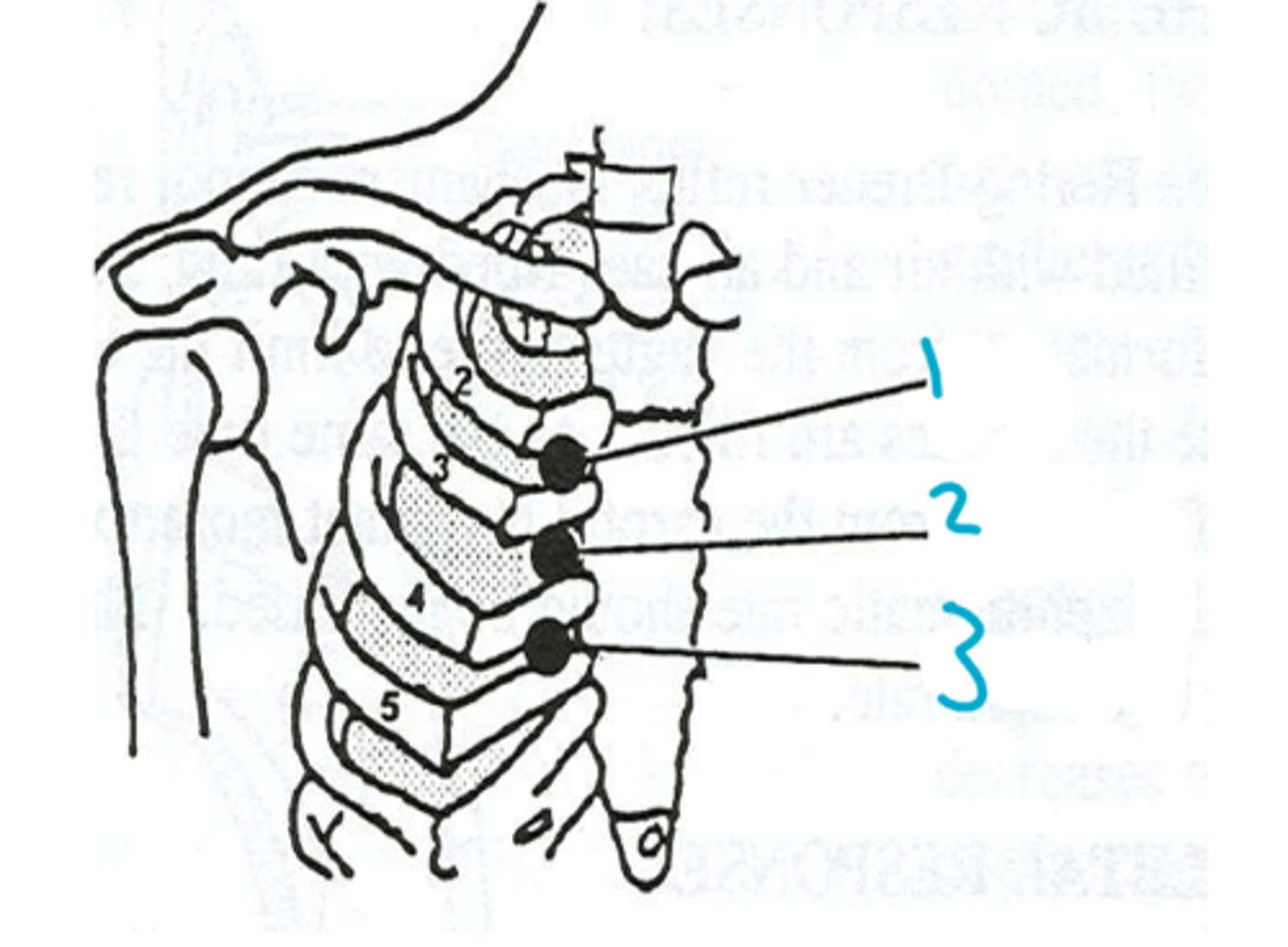
Chapman's Reflex Points
• A system of reflex points that present as predictable anterior and posterior fascial tissue texture abnormalities
Chapman's Reflex Points
• Reflective of VISCERAL disease or dysfunction via autonomic afferents
• Probable concurrent involvement of sympathetic efferents
Chapman's Reflex Points
• Located in deep fascia or periosteum
• Usually paired: anterior and posterior
• Relatively fixed in anatomic location (not mobile)
• May need to relax the overlying tissues first
• Usually found using a firm rotatory motion, either deep or superficial
• When compressed, response ranges from nonpainful to almost unbearable
Heart
1
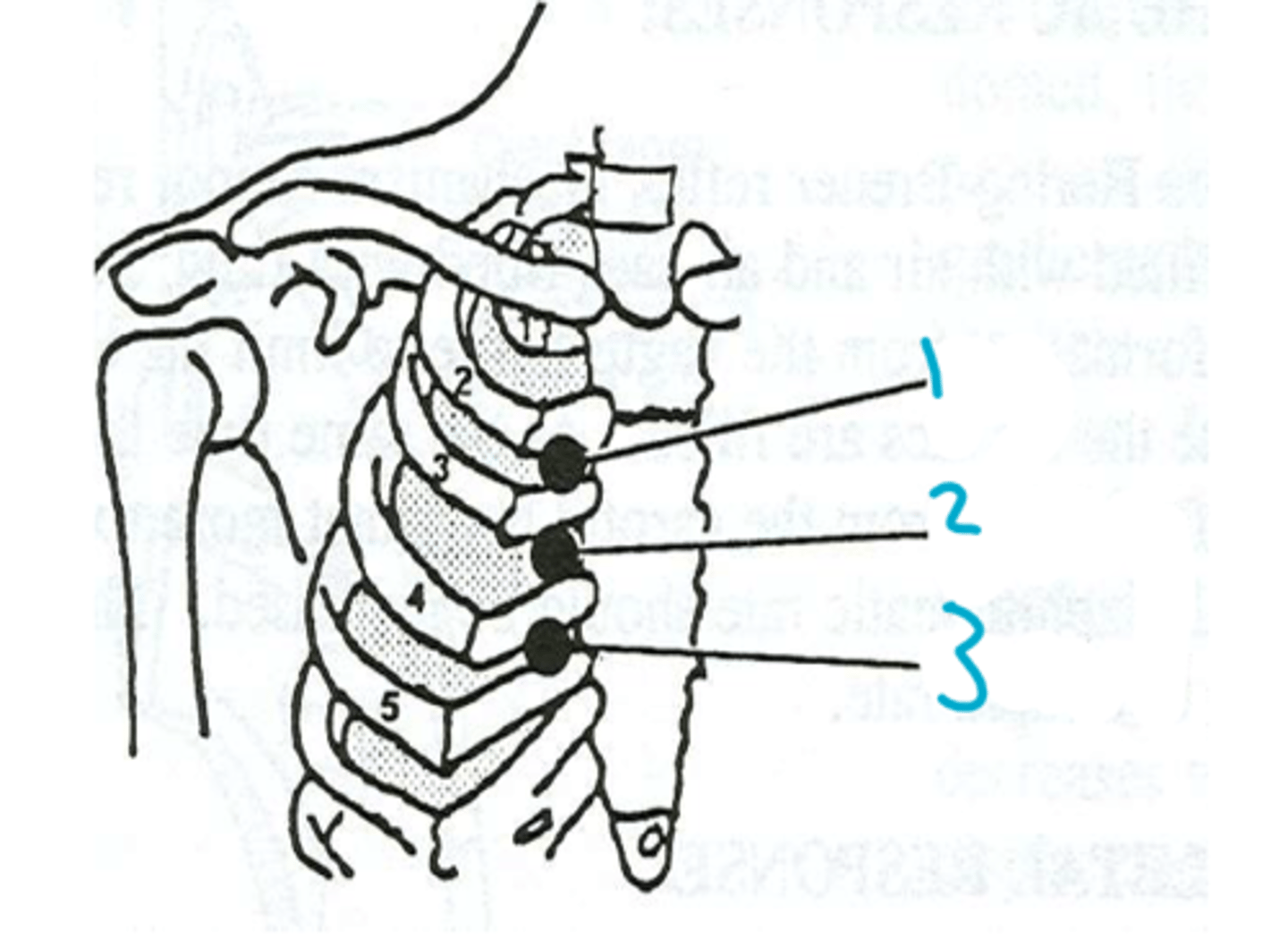
Upper Lung
2
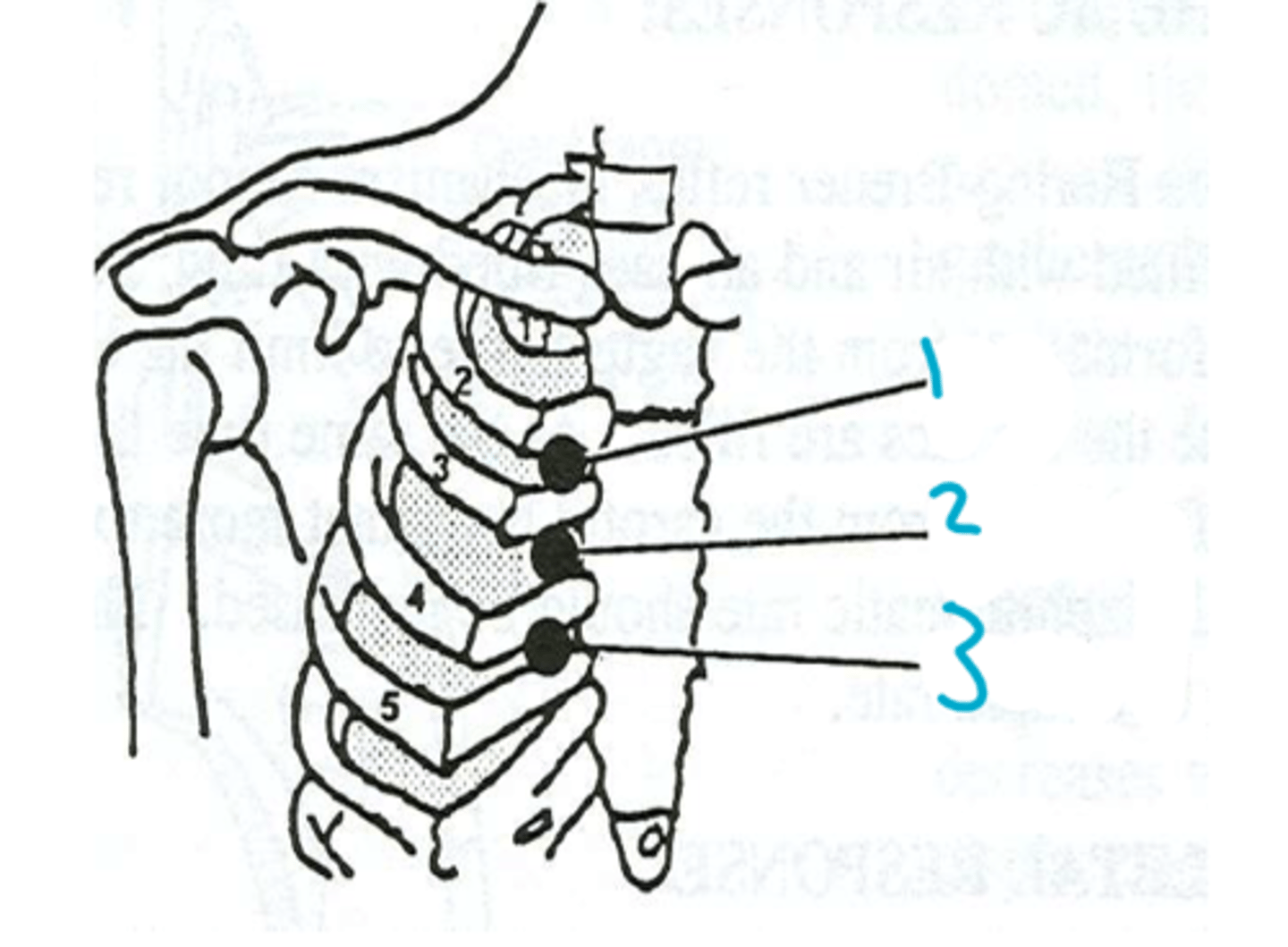
Lower Lung
3
Chapman's Reflex Points
• Palpation can aid in determination of presence or absence of visceral dysfunction
• Reduce adverse sympathetic influence on a particular organ or visceral system
• Improved function of the disturbed organ usually follows treatment of Chapman point
-Apply firm pressure
-Slowly move finger in circles
-Continue rotating pressure to 10-30 seconds
-End when mass disappears or is intolerable
How do you treat a Chapman's point?
Metabolic Energy Model
• Energy expenditure
• Energy conservation
• Changes in musculoskeletal system can effect body's energy requirements.
Behavioral Model
• Role of limbic system in perception of pain
• Depression and musculoskeletal pain
Metabolic Energy Model
goal of this model is to reduce energy requirements and to help maintain homeostasis by reduction of impediments to efficient energy use
Behavioral Model
goal of this model is to reduce or eliminate somatic dysfunction which may add to the overall allostatic load
• Inhibition and MFR to upper Thoracic T1-2 and then T3-5
• Then treat OA,AA,C3-5
Post MI OMT
-Improve thoracic compliance
-Enhance venous return to the heart
-Maximize efficacy of the diaphragm
-Normalize autonomic tone
-Treat secondary effects
goals of osteopathic management of CHF
1. Structural Screen
2. Open thoracic inlet
3. Doming abdominal diaphragm
4. Ischiorectal fossa release (Dome Pelvic Diaphragm)
5. Popliteal fossa release
6. Direct Pressure Techniques
7. Lymphatic Pump Techniques
Sequence of lymphatic treatment