Congenital Heart Disease
1/153
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
154 Terms
What is congenital heart disease (CHD)?
A structural anomaly of the heart or great vessels present at birth that is, or could be, of functional significance.
What is the most common birth defect in humans?
Congenital heart disease (CHD).
What are the common types of congenital heart defects?
Atrial septal defect (ASD), ventricular septal defect (VSD), patent foramen ovale (PFO), patent ductus arteriosus (PDA), coarctation of the aorta, Tetralogy of Fallot, transposition of the great vessels.

What embryological structure forms the heart by approximately 3.5 weeks of gestation?
Bilateral clusters of progenitor cells that form a cardiac crescent and midline linear heart tube.
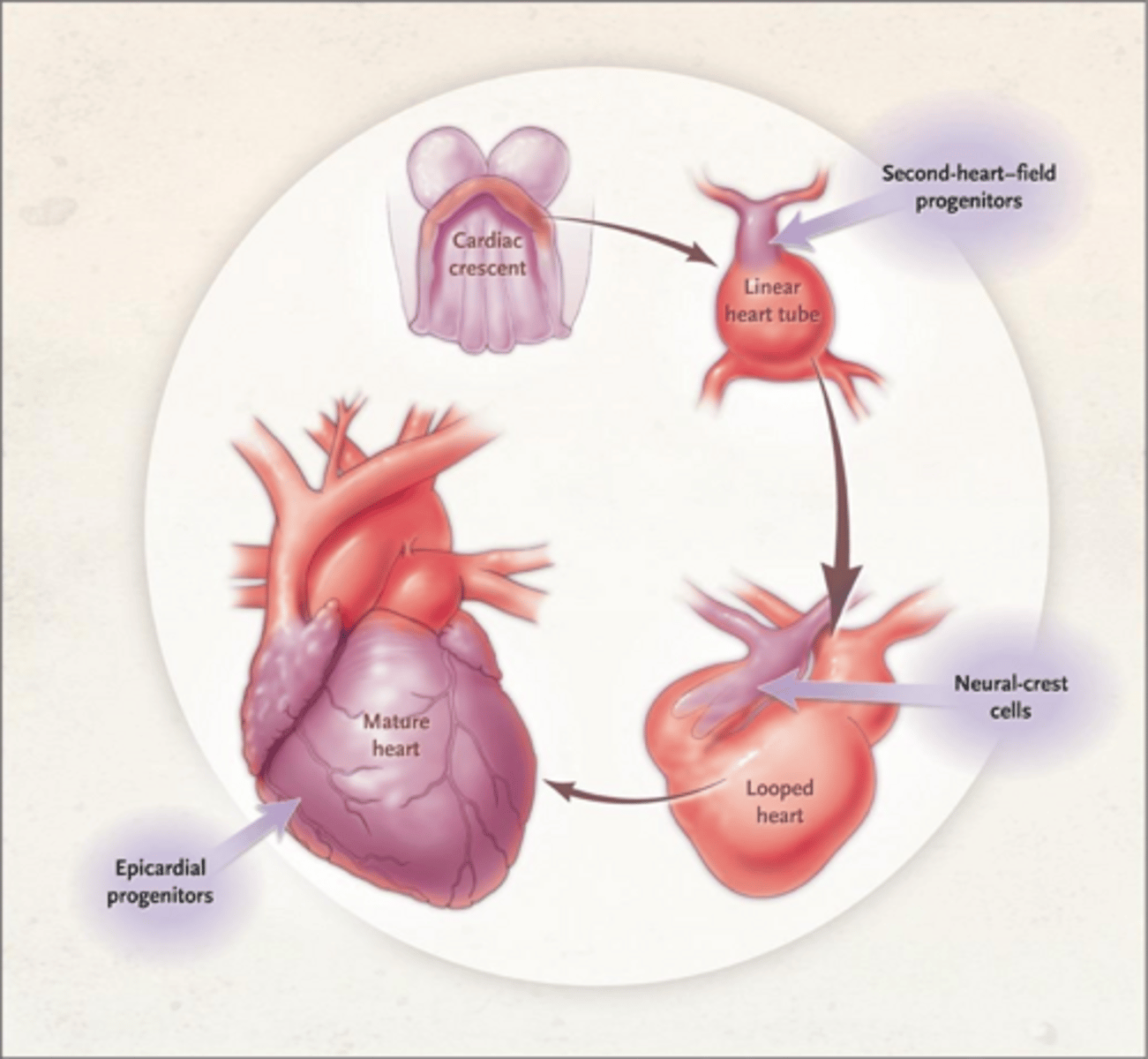
What development error leads to ASD/PFO?
Failed atrial separation
What development error leads to TOF and D-TGA?
Neural crest/conotruncal defect.
What are the types of atrial septal defects?
Ostium secundum, ostium primum, sinus venosus, and coronary sinus defect.
What is the significance of a left-to-right shunt in atrial septal defect (ASD)?
It leads to RV volume overload, pulmonary overcirculation, and potential atrial enlargement.
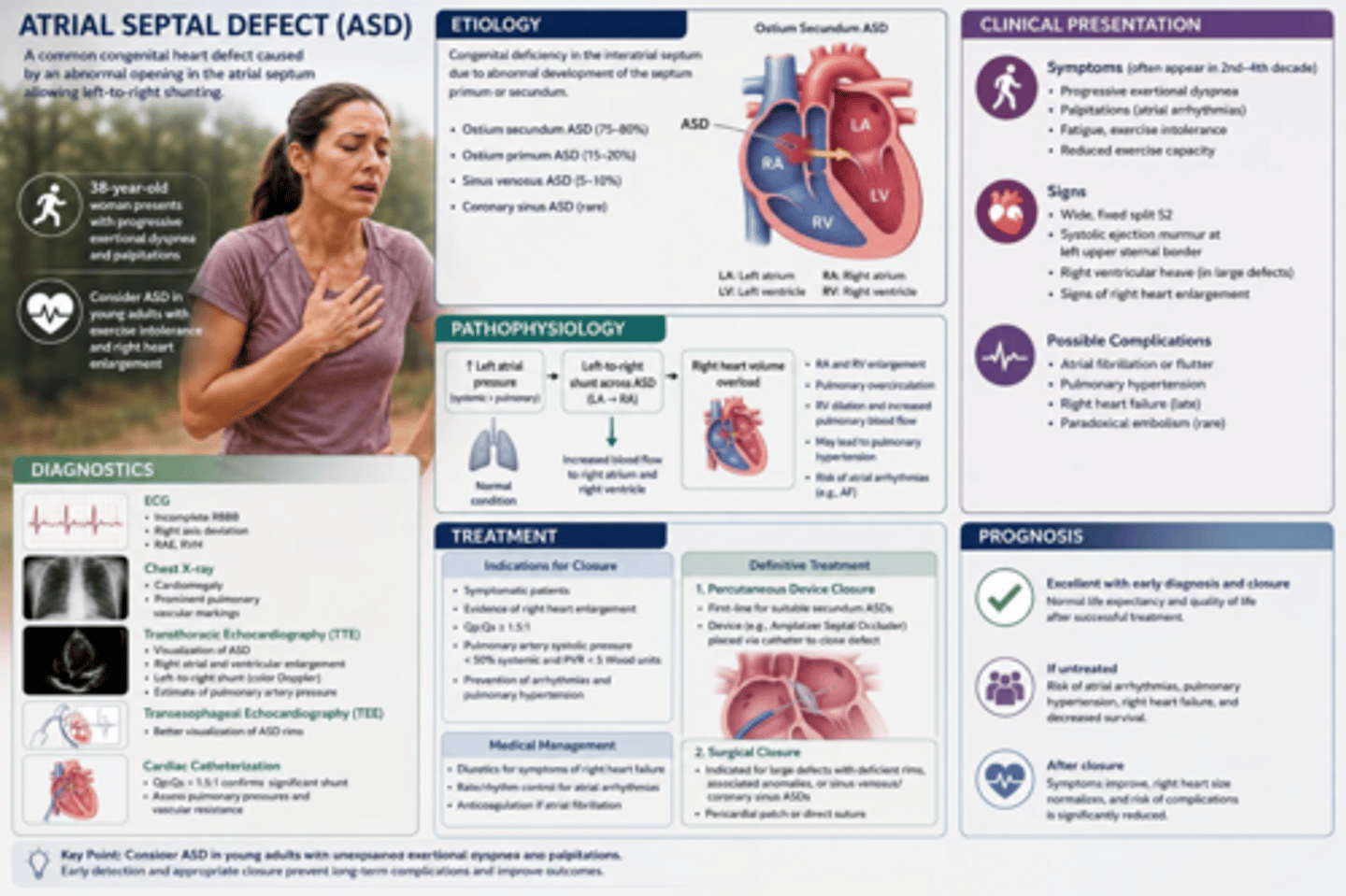
What are the consequences of an atrial septal defect?
RV volume overload leading to RV enlargement, pulmonary overcirculation, atrial enlargement leading to afib or flutter, PAH develops in 6-19% of people.
What is the typical clinical presentation of an adult with an atrial septal defect?
Dyspnea, fatigue, exercise intolerance, palpitations, and a fixed, widely split S2 (systolic flow murmur at upper left sternal border).
What diagnostic tool is primarily used for assessing atrial septal defects?
Transthoracic echocardiography (TTE). Helps detect location, size, shunt direction and RV dilation.
When do you use a TEE with ASD?
Superior for device closure planning.
What is seen on CXR with ASD?
Cardiomegaly, prominent pulmonary vascularity.
When would you use cardiac catheterization in ASD?
Reserved for PVR assessment when PAH suspected
What is the treatment for hemodynamically significant atrial septal defects?
Closure indicated for defects with Qp:Qs ≥1.5 and RV enlargement, using percutaneous device closure (for secundum ASDs with suitable anatomy) or surgical closure (for primum, sinus venosus and coronary sinus defect)
When is closure contraindicated in ASD?
PA systolic pressure >2/3 systemic or net R-> L shunt (Eisenmenger)
What is the natural history of untreated large atrial septal defects?
~25% die before age 27; 90% by age 60.
What are the consequences of a significant left-to-right shunt in VSD?
Pulmonary overcirculation, RV volume overload, and potential heart failure.
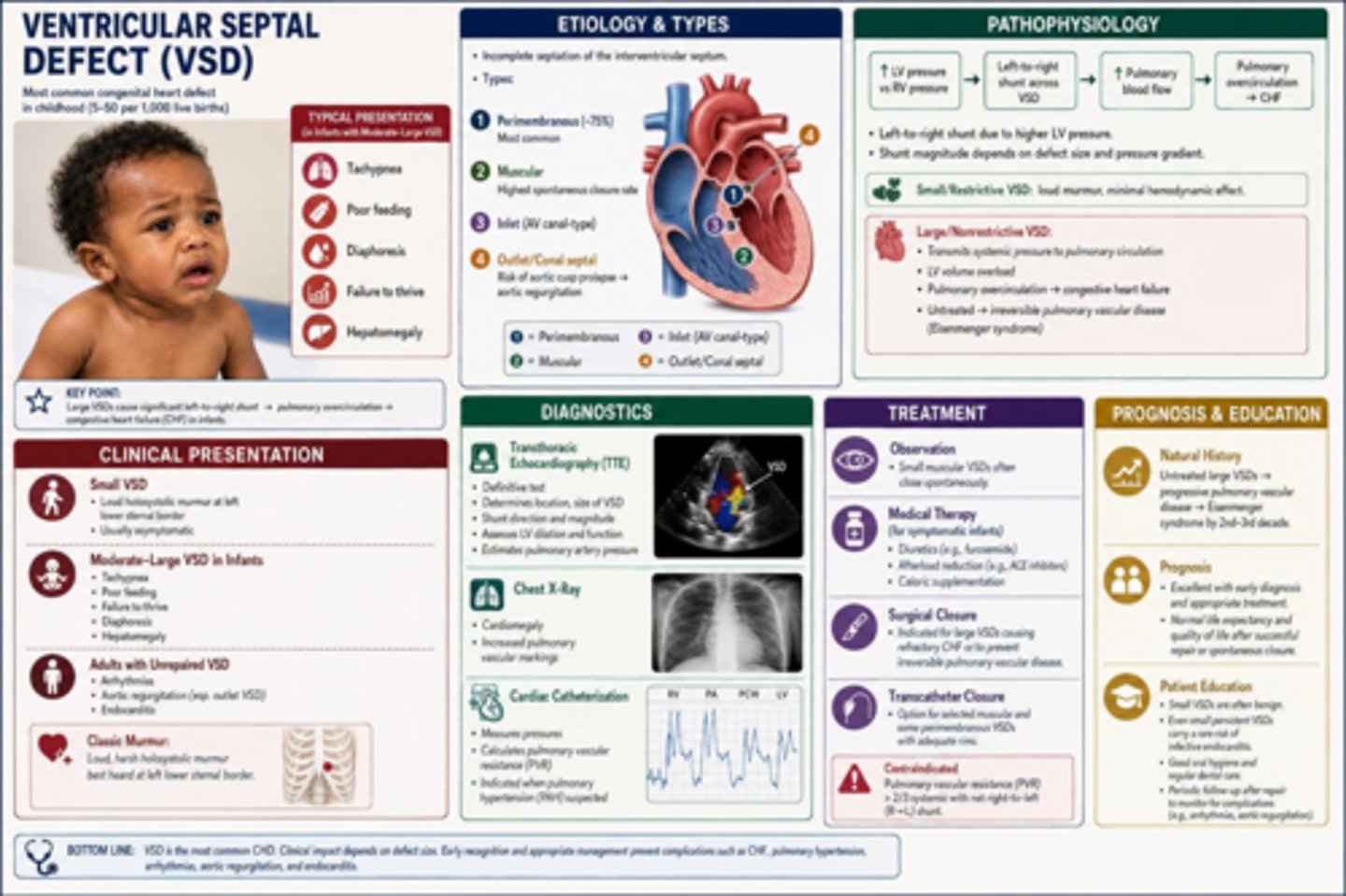
What is the most common congenital heart defect (CHD) in childhood?
Ventricular Septal Defect (VSD); usually very young like several weeks old.
What causes VSD?
Incomplete septation of the interventricular septum
What type of VSD is the most common?
Perimembranous VSD (~75%)
Which type of VSD has the highest spontaneous closure rate?
Muscular VSD
What is a potential risk associated with outlet/conal septal VSD?
Aortic cusp prolapse leading to aortic regurgitation
What is the pathophysiology of VSD?
Left-to-right shunt due to higher left ventricular (LV) pressure
How does the size of a VSD affect its clinical presentation?
Small/restrictive VSDs have a loud murmur with minimal hemodynamic effect; large/nonrestrictive VSDs can lead to significant complications.
What are the consequences of untreated large VSDs?
Can lead to Eisenmenger syndrome and irreversible pulmonary vascular disease.
What are common clinical features of a small VSD?
Loud holosystolic murmur at the left lower sternal border, often asymptomatic.
What symptoms might moderate-large VSDs present in infants?
Tachypnea, poor feeding, failure to thrive, diaphoresis, hepatomegaly.
What are adults with unrepaired VSD at risk for?
Arrhythmias, aortic regurgitation, and endocarditis.
What diagnostic tool is definitive for assessing VSD?
Transthoracic echocardiogram (TTE). Used for definitive location, size, shunt direction, LV dilation and estimated PA pressure.
What does a chest X-ray (CXR) show in VSD cases?
Cardiomegaly and increased pulmonary vascular markings.
What is the treatment for small muscular VSDs?
Observation, as they often close spontaneously.
What medical therapies are used for symptomatic infants with VSD?
Diuretics, afterload reduction, caloric supplementation.
When is surgical closure indicated for VSD?
For large VSDs causing refractory congestive heart failure (CHF) or to prevent irreversible pulmonary vascular disease.
What is the natural history of untreated large VSDs?
Can lead to Eisenmenger syndrome by the 2nd to 3rd decade of life.
What is a Patent Foramen Ovale (PFO)?
A normal fetal communication that persists in ~25% of adults due to failure of septum primum to fuse with septum secundum. NOT a true ASD.
What is the clinical significance of PFO?
Usually hemodynamically insignificant BUT can lead to paradoxical embolism and cryptogenic stroke.
What are the clinical features of PFO?
Usually asymptomatic, incidentally discovered. Significant in cryptogenic stroke, or associated with migraine with aura, platypnea-orthodeoxia, decompression illness.
What is the gold standard for diagnosing PFO?
Transesophageal echocardiogram (TEE) with agitated saline (bubble study).
What is the recommended treatment for PFO in patients with cryptogenic stroke?
Percutaneous PFO closure for secondary stroke prevention.
What is the first-line medical therapy for PFO?
Aspirin.
What is the risk of recurrent stroke with medical therapy for PFO?
Approximately 1.1% per year.
What is the ductus arteriosus?
Normal fetal connection between pulmonary artery and descending aorta.
What triggers the postnatal closure of the ductus arteriosus?
Rising oxygen tension and falling prostaglandin levels.
How long does functional closure of the ductus arteriosus take?
24-72 hours after birth.
When does anatomic closure of the ductus arteriosus occur?
2-3 weeks after birth.
What percentage of low-birth-weight preterm infants experience PDA?
Approximately 33%.
What is the pathophysiology of a hemodynamically significant PDA (hsPDA)?
It leads to a left-to-right shunt, pulmonary edema, and systemic hypoperfusion (renal, mesenteric and cerebral steal)
What are infants with PDA at risk for?
BPD, NEC, IVH.
What are common clinical features of PDA?
Continuous 'machinery' murmur, bounding pulses, widened pulse pressure, tachycardia, tachypnea, and feeding difficulties.
Which diagnostic tool confirms the presence of PDA?
Echocardiography.
What is the recommended treatment for persistent hsPDA beyond 2 weeks?
Ibuprofen or acetaminophen, transcatheter closure, or surgical ligation.
What is the recommended treatment for term infants/older patients?
Transcatheter closure, or surgical closure for hemodynamically significant PDAs.
What is the natural history of PDA?
Many preterm PDAs close spontaneously; untreated large PDAs can lead to CHF, PAH, and Eisenmenger syndrome.
What is Eisenmenger Syndrome?
A condition characterized by pulmonary hypertension at systemic levels due to chronic left-to-right shunting.
What causes the shunt reversal in Eisenmenger Syndrome?
Irreversible pulmonary vascular remodeling leading to increased pulmonary vascular resistance (PVR).
What is a post-tricuspid shunt in Eisenmenger Syndrome?
VSD, PDA, ASVD. High pressure, high flow -> PAH develops in the first years of life.
What is a pre-tricuspid shunt in Eisenmenger?
ASD; low pressure, volume only -> PAH develops much later (4th-5th decade) if at all.
What is the relationship between Down syndrome and pulmonary vascular disease?
Down syndrome is an independent risk factor for earlier and more severe pulmonary vascular disease.
What are the cardinal features of Eisenmenger Syndrome?
Central cyanosis, digital clubbing, and exertional dyspnea.
What happens to the original murmur in Eisenmenger Syndrome?
It disappears as pulmonary vascular resistance rises and the shunt equalizes.
What is the significance of a 'disappearing' murmur in a child with VSD?
It indicates potential development of Eisenmenger physiology and is a RED FLAG!!!!!
What is the window of opportunity for repairing post-tricuspid defects?
Repair should occur within the first 6-12 months of life to prevent irreversible changes.
What is the recommended timing for repairing pre-tricuspid defects?
Before the 4th decade of life, though earlier is better.
What is the consequence of defect closure once Eisenmenger physiology is established?
Closure is contraindicated as it can lead to acute right ventricular failure and death.
What are the long-term management recommendations for Eisenmenger Syndrome?
Avoid pregnancy, dehydration, routine phlebotomy, general anesthesia, and competitive sports.
What is the role of PAH-directed therapy in Eisenmenger Syndrome?
It improves symptoms and survival.
Is routine anticoagulation recommended in Eisenmenger?
NO, high bleeding risk.
What are the hemodynamic consequences of Eisenmenger Syndrome?
It leads to irreversible pulmonary vascular disease from chronic left-to-right shunt and subsequent shunt reversal.
What is coarctation of the aorta (CoA)?
Narrowing of the aorta just distal to the left subclavian artery at the level of the ductus arteriosus.
What exists in ≥50% of CoA?
Bicuspid aortic valve
What are common associated anomalies with coarctation of the aorta?
Ventricular septal defect (VSD), patent ductus arteriosus (PDA), and aortic arch hypoplasia.
What is the pathophysiology of coarctation of the aorta?
It causes a pressure gradient between the upper and lower body, leading to proximal hypertension and distal hypoperfusion.
What are the clinical features of coarctation of the aorta in neonates?
Ductal-dependent systemic circulation leading to shock, acidosis, and congestive heart failure upon ductal closure.
What are the clinical features of coarctation of the aorta in older children/adults?
Upper extremity hypertension, diminished/delayed femoral pulses, arm-leg BP gradient >20 mmHg.
What diagnostic tools are used for coarctation of the aorta?
Transthoracic echocardiography (TTE), MRI/CT angiography, chest X-ray (CXR), and catheterization.
What CXR finding is associated with CoA?
Rib notching, "figure 3" sign.
What is the treatment for coarctation of the aorta in neonates?
Prostaglandin E1 followed by surgical resection with extended end-to-end anastomosis.
What is the treatment for CoA in older children and adults?
Endovascular stenting preferred. Antihypertensive therapy for persistent HTN.
What is the prognosis for untreated coarctation of the aorta?
80% mortality, with causes including aortic dissection, congestive heart failure, and intracranial hemorrhage.
What is the most common cyanotic congenital heart defect?
Tetralogy of Fallot (TOF).
What are the four defects in Tetralogy of Fallot (TOF)?
Right ventricular outflow tract (RVOT) obstruction, large malalignment ventricular septal defect (VSD), overriding aorta, and right ventricular hypertrophy.
What genetic abnormalities are associated with ToF?
22q11.2 deletion (DiGeorge syndrome) and trisomy 12
What is the pathophysiology of non restrictive VSD in ToF?
Degree of R-> L shunt depends on severity of RVOS obstruction vs systemic vascular resistance. Severe obstruction is significant R->L shunt and leads to cyanosis. Mild obstruction is predominantly L->R shunt and leads to "pink tet"
What are hypercyanotic spells in Tetralogy of Fallot?
Acute worsening of RVOT obstruction leading to increased right-to-left shunting and profound cyanosis.
What happens to the murmur in Tet spells in TOF?
RVOT obstruction reduces flow across the obstruction, paradoxically softening the murmur.
What is the typical onset of cyanosis in Tetralogy of Fallot?
Weeks to months after birth, or during spells.
What is the characteristic murmur associated with Tetralogy of Fallot?
A harsh systolic ejection murmur at the left upper sternal border.
What clinical/physical feature is seen during Tet spells?
Squatting, which increases SVR, reduces R->L shunt.
What signs of chronic hypoxia are seen in TOF?
Nail clubbing and polycythemia.
What is the significance of a single S2 in Tetralogy of Fallot?
It indicates a single loud second heart sound due to the absence of a normal split.
What imaging findings are associated with Tetralogy of Fallot on chest X-ray?
A boot-shaped heart with decreased pulmonary vascular markings.
What is the acute management for ductal-dependent?
Prostaglandin E1.
What is the acute management for a Tet spell?
Knee-to-chest positioning, oxygen, morphine, phenylephrine, and IV fluids.
What is the definitive repair for Tetralogy of Fallot?
Complete surgical repair (VSD closure + RVOT relief) typically performed at 3-6 months of age.
What is the palliative repair for TOF?
Modified BT shunt or ductal stent in high-risk neonates.
What are late complications following repair of Tetralogy of Fallot?
Pulmonary regurgitation, right ventricular dilation, arrhythmias, and sudden cardiac death.
What is the prognosis for patients with repaired Tetralogy of Fallot?
30-year survival rate greater than 90% with modern surgical techniques.
What is the primary defect in D-TGA?
Ventriculoarterial discordance: Aorta arises from morphologic RV, and pulmonary artery arises from morphologic LV.
What are the consequences of D-TGA on circulation?
Creates two parallel circulations.