Patho2-Cardiac
1/66
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
67 Terms
Preload (load = work)
Volume of blood in ventricles at END of diastole/End diastolic ventricular pressure
Diastolic = RE=elaxation
Blood ENTERING heart BEFORE contraction
Venous Return/Blood entering the right atrium
Increased in
Hypervolemia
Regurgitation of cardiac valves
Heart failure
Afterload (load=work)
Resistance left ventricle must overcome to circulate blood
Force required to eject left ventricle volume
Increased in
Hypertension
Vasoconstriction
Inc afterload = inc cardiac workload
PVR= peripheral vascular resistance which affects afterload
Contractility + SV
Contractility = ability of myocardium to stretch and contract in response to filling of heart with blood////hearts ability to contract and pump blood effectively
SV = amount of blood ejected from ventricles with each contraction
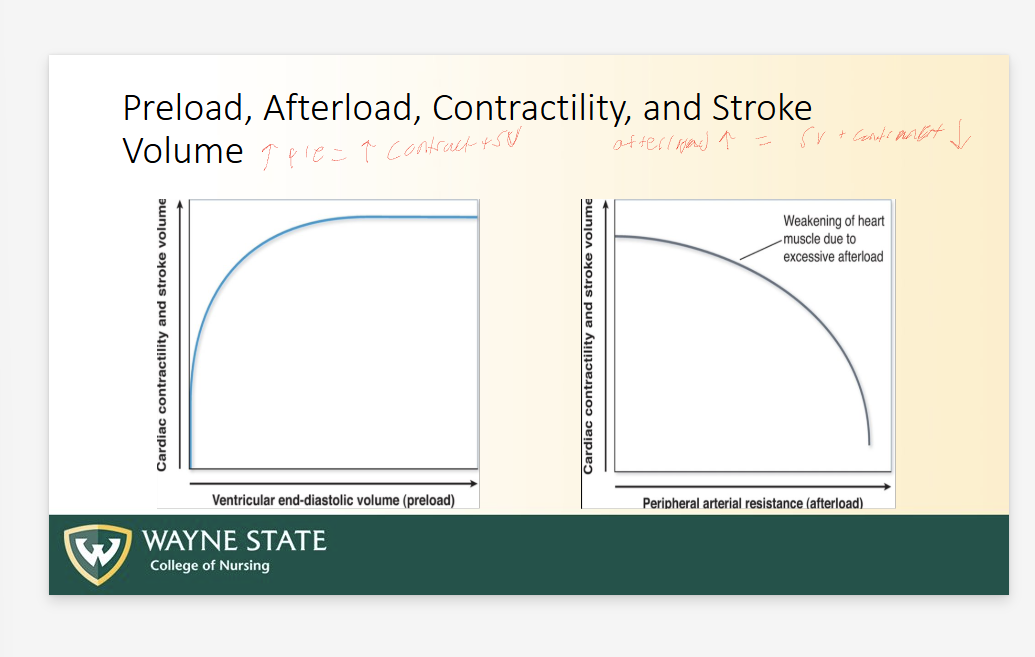
Preload, Afterload, Contractility, and SV
Increased pre = Increased contractility + SV
Increased afterload = DECREASED SV + contractility
Weaking of heart muscle due to EXCESSIVE afterload
Left ventricular ejection fraction (LEVF)
Percentage of blood leaving the LV each time it contracts
Healthy = 60-70
Lower than 40= heart failure
Vol blood ejected/ Vol blood in LV
Inotropic + Chronotropic function
Ino: Force of contraction of cardiac muscle
Chrono = Heart rate
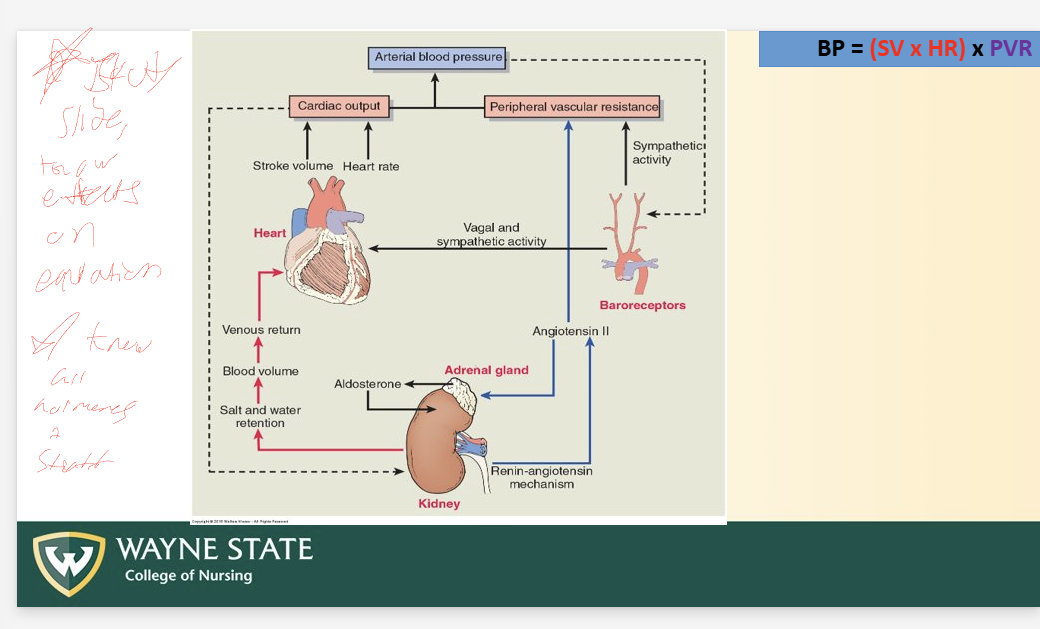
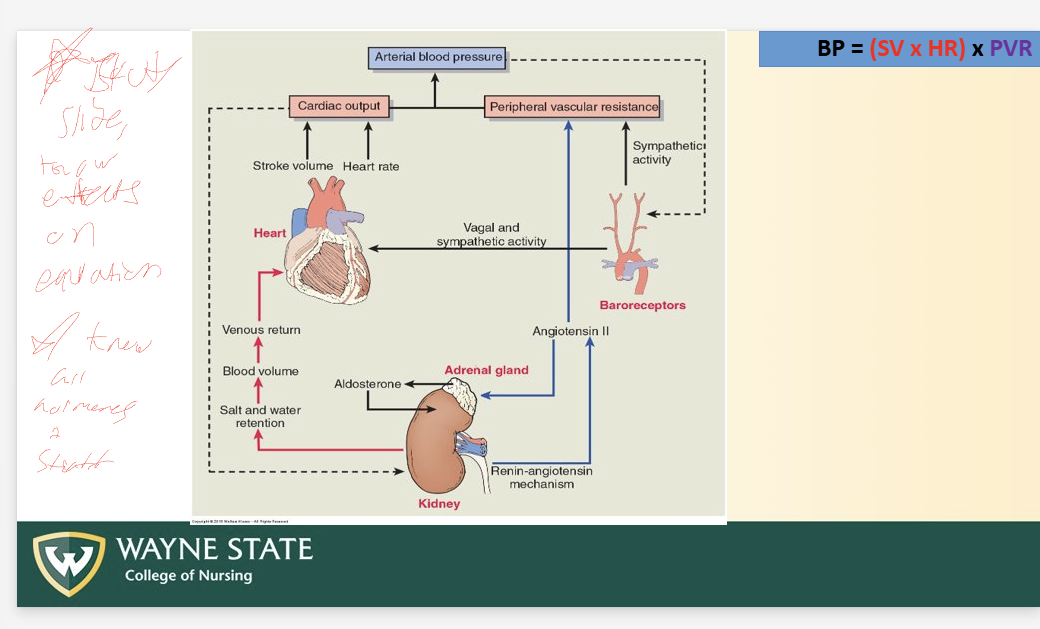
Blood Pressure
BP = CO x PVR
Refers to PRESSURE IN PERIPHERAL ART SYSTEM
CO = volume of blood pumped/min (ml/min)
PVR = systemic vascular resistance
Vasoconstrict = inc pvr
Vasodilate = decreased pvr
Cardiac Outfput
Volume of blood pumped/min (ml/min)
CO = SV x HR
Avg SV = 70ml
Avg = 70 ish
Avg CO = 5ml/min
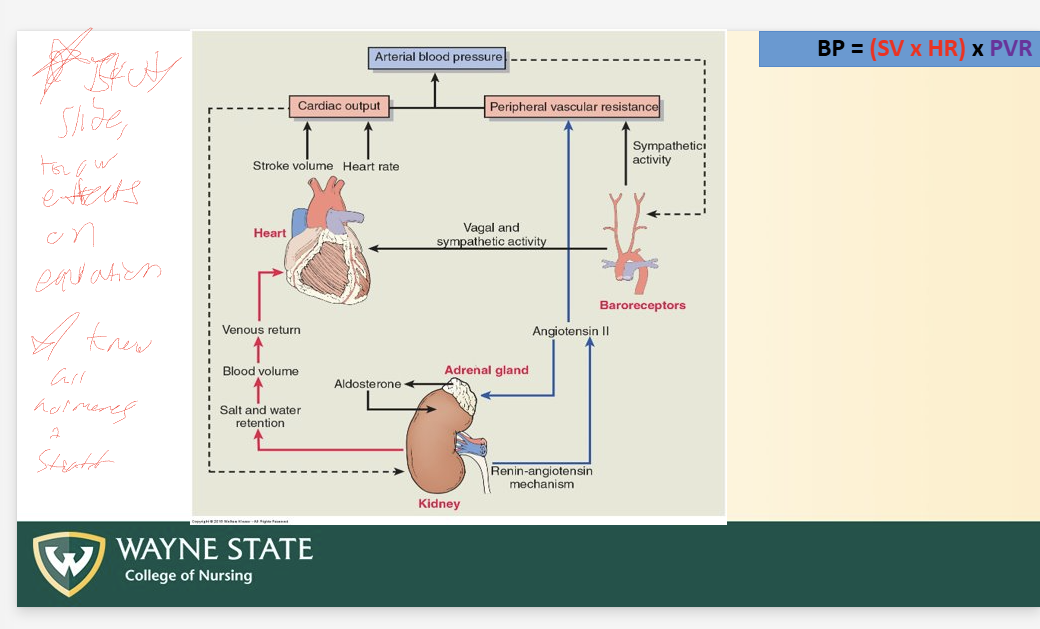
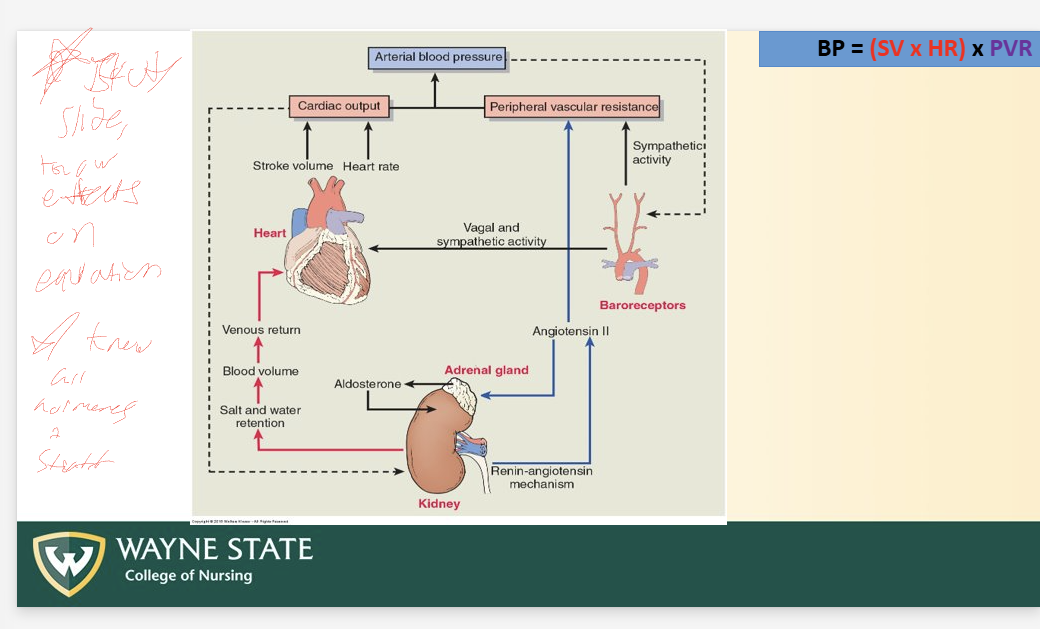
Total BP Equation
BP = (SV x HR) x PVR
CO = SV x HR
BP regulation (3)
Sympathetic nervous system
Antidiuretic hormone (ADH)
Renin-angiotensin-aldosterone system (RAAS)
PLEASE KNOW EFFECTS ON EQUATION
Sympathetic Nervous System (BP Regulation)
Steps
Decrease BP
Baroreceptor activation + signal send
Activates SNS
B1 activation
=HR
=CO
A1 activation
Vasocontriction
=PVR
AHD (BP Regulation)
Steps
Low BP
ADH secretion by pituitary gland
Reabsorption of water at kidney
Increase extracellular water volume
Increase Blood volume
Increases venous return
Increases SV = increase CO
RAAS (BP Regulation)
Steps
Decrease BP or Decrease extracellar fluid (due to decreased Na)
Kidney
release Renin
Liver
Renin causes liver to change angiotensinogen to angiotensin I
Lung
ACE enzyme converts Angio 1 to Angio 2
2 responses (to angio2 in body)
1
Adrenal cortex release aldosterone
Causes sodium reabsorption at kidney + water reabsorption = SV increase
Increase volume + arterial blood pressure
2
Causes direct vasoconstriction of system arterioles = PVR increase
Increases arterial blood pressure
Endothelial damage
Caused by:
Hypertension
Hypercholesterolemia (high blood cholesterol)- LDL
Smoking
Uncontrolled diabetes mellitus
Uncontrolled endothelial injury leads to ATHEROSCLEROSIS (plaque buildup)
Atherosclerosis Steps (3 main)
Inflammation occurring in blood vessels due to endothelial cell damage
WBC arrive + Platelets
WBC margination
Endothelial layer becomes permeable + Leucocytes/WBC adhere + roll
WBCs transmigrate into tunica intima
WBC become “FOAM CELL” (wbc filled with LDL)
Macrophage engulf LDL at inflammation cite
Bad
Adherence + entry of leukocytes
Adherence + aggregation of platelets
Foam cell formation continue (Inside tunica intima
Smooth muscle migration occurs
Release of toxic oxygen species
Fibrous cap formation + Necrotic core
Macrophage + foam cel + lymphocyte + collagen accumulate
Necrotic core formation in center
Smooth muscle migrates to top later to create a “Fibrous cap”
IF FIBROUS CAP OPENS
Tissue factor released by necrotic core
Clotting cascade activated
Blockage of blood vessel occurs
Atherosclerotic Plaques + Fatty Streaks
Fibrous cap =
Top “Cap” layer = endothelial cell
Macrophage
Soft muscle cells
Lymphocytes
SHOULDER = les reinforced side portion
Fatty streaks = collection of foam cells
Highest risk locations of athersclerosis
Abdominal aorta + iliac arteries
Proximal coronary arteries
Thoracic aorta, femoral, and popliteal arteries
Internal carotid arteries
Vertebral, basilar, and middle cerebral arteries
1st = HIGHEST RISK
CHEST/ ABD comes first, then the mroe peripheral brain is the last lukily
Peripheral Arterial Disease (PAD)
ALSO known as Peripheral arterial “occlusive” disease (PAOD)
Increased atherosclerosis = Increased chance for PAD
Atherosclerosis plaque obstructs blood flow to a LOWER extremity
Acute vs chronic
Risk factors
Age
HTN
DM
SmokingHigh fat/LDL diet
Sedentary lifestyle
Obesity = increase LDL
Family history
Hyperlipidemia
PAD Steps
Occlusion of arterial blood flow (due to athero)
Reduciton in arterial blood flow
Decrease tissue oxygen supply = hypoxic damage
Ischemia(dec bloodflow and O2 to an are) AND anaerobic metabolism
Sx
Pain
Pain with exertion (due to lwo O2), less pain when resting
Pallor + coolness
Weak pulses
paresthesia- tingling and numbness
Ankle, Brachial Index
Comparison of BP in leg vs BP in arm
BP in leg/ BP in arm
Normal ratio is OVER 1 (higher BP in ankles than brachial)
SEVERE PAD = less than 0.5
Arterial vs Venous Disease
Arterial = PAD
No pulse
Color = pale to necrotic blue
Sharp VERY painful
Paresthesia (numbness or tingling)
Paralysis
Venous Disease = PUD
Pulse
Pink warm dark red - stasis dermatitis
NOT as painful, achy instead
Edema congestion (blood can’t move back to heart well)
Ulcer development
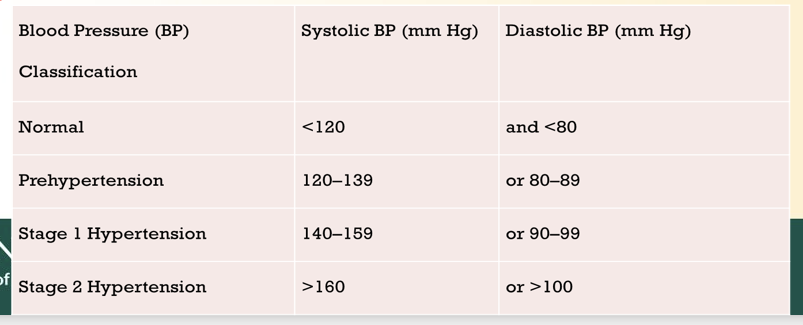
Hypertension
Damaging force on endothelial linings of arteries - leads to atherosclerosis
High resistance = inc aferload = cardiac hypertrophy = heart failure
HTN = inflammation = atheroslcerosis
High BP = High afterload
Systole = contarction
Diastole = relaxation
Know hypertension ranges??
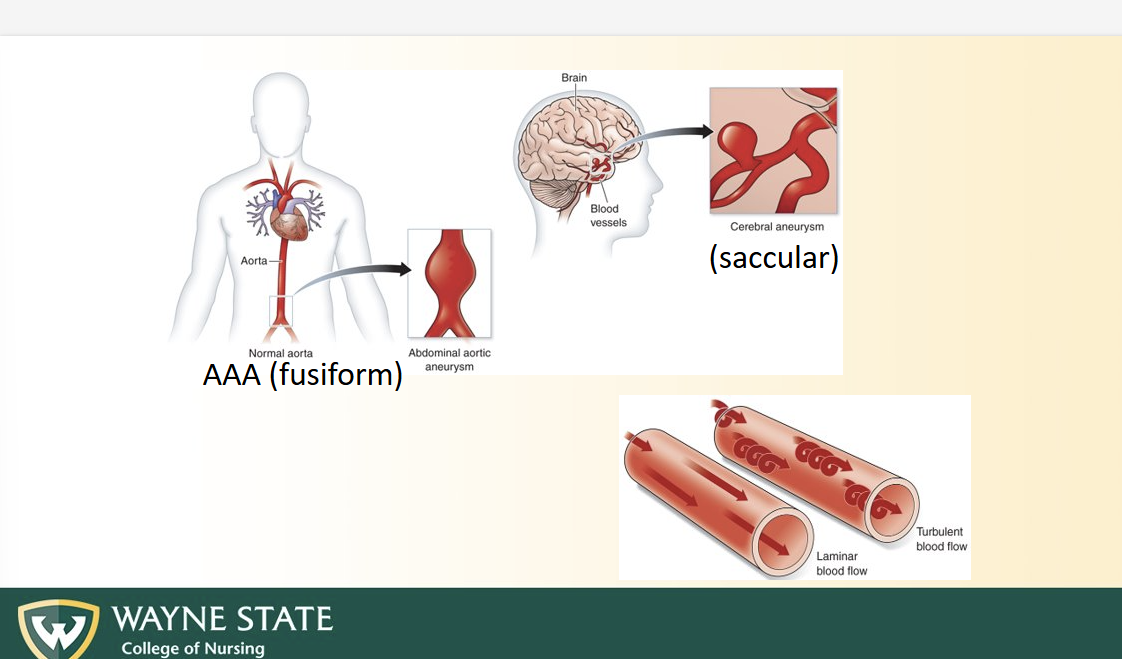
Aneurysms
Weakening in artery wall causing local BULGING + DILATION
Susceptible to RUPTURE = internal hemorrhage
Lead to turbulent blood flow: Erratic blood movement and velocity changes rather than “smooth parallel movement”
Risk factor:
HTN
Athero
Smoking
S/Sx: vary based on severity, size, locaiton
Asymptomatic UNTIL RUPTURE
Bruits = indicative of turbulent blood flow
Diminshed pulse
Common
Aorta and cerebral arteries
Laminar vs Turbulent Bloodflow
Laminar = straight, smooth, parallel blood flow
Turbulent = winding, erratic speed, erratic overall
Aneurysm types
AAA/ fusiform = buldge of an artery
Saccular = sac coming off of blood vessel
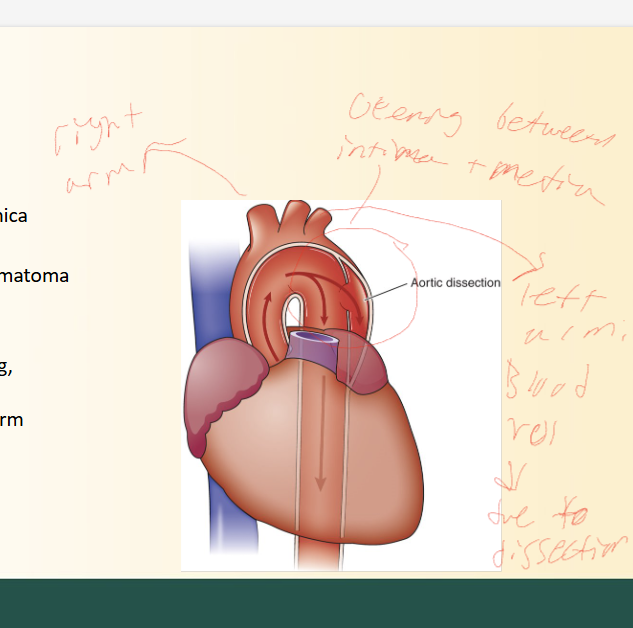
Aortic Dissection
Tear in arterial lining between tunica intima and media
Forms HEMATOMA in blood wall
S/sx
Pain in chest or back (sharp, ripping pain_
BP difference in arms
Due to tear being in aorta, effects blood flow to body depending on where (LOOK AT PICTURE)
WIDE pulse pressure
Hypercholesterolemia
More HLD is GOOD, More LDL is BAD
LDL = low density lipoprotein
Less protein, more cholesterol
Transports cholesterol FROM LIVER to CELLS
Can be oxidized + Despotized onto artery walls = athero
HDL = high density
More protein, less cholestorl
Transports cholesterol FROM CELLS TO LIVER
CLEAN UP/ regulates LDL storage + promoted excretion
Smoking
Causes endothelial damage + initiate athero
Nicotine
Potent vasoconstrictor, ESPECIALLY in coronary arteries
Diabetes
Uncontrolled diabetes intiates athero
WHY? idk its not in the slides
Coronary Artery Orifice
How blood gets to heart muscle
Anterior view
Aortic valve sits between LV and aorta
Just above valve = aortic sinuses
Right AS - goes to right coronary art
Left AS- goes to left cornoar art
Posterior sinus
Aortic sinus = catch blood when valve closes
Systole/ valve open
Coronary arteries DONT get much blood here
Valve leaflets block opening to coronary arteries
Diastole/ valve closed
Blodo flows backward slightly into aortic sinuses
Blood flow in sinuses = blood enter coronary arteries which FEEDS myocardium
IMPORTANT
Perfusion happens in diastole
Shorten diastole (like tachy) = REDUCED coronary blood flow
Aortic valve malformation = impact perfusion
Etc.
Coronary Art Disease (CAD)/ Coronary heart disease CHD/ Ather erotic heart Ds.
Disease from impaired blood flow
Leads to chronic ischemic heart ds
Stable angina, silent ischemia
Ischemia = schemia is a condition characterized by insufficient blood flow to a part of the body, leading to a shortage of oxygen and nutrients necessary for cellular metabolism.
Angina = pain or pressure
Leads to Acute Coronary Syndrome
Unstable angina, possible MI
Atherosclerosis leads to CAD
Steps Stable angina
Asymp atherosclerotic plaque buildup
Larger, stable atherosclerotic plaque (stable fibrous capsule) = dec blood flow = stable angina
Steps acute coronary syndromes
Unstable plaque buildup, plaque disruption + platelet aggregation (sudden onset, more painful, bigger risk)
CAN LEAD TO
Non - ST segment elevation MI
Minor thrombus in blood vessel = minor blockage
ST- segment elevation MI
MAJOR
Full blockage thrombus
Chronic Ischemia Heart Disease
Ischemia = imbalance between myocardial oxygen supply + demand
Sx:
PAINFUL, very
Stable angina better than unstable angina// stable acts up when exerted du eo diffeirng emands, wheras unstable will hrut EVEN at rest
Atherosclerosis
Asymptomatic when O2 demand = O2 supply
Symptomatic when O2 demand is higher than supply
2 types:
Partial occlude = reduced blow flow
When supply less than demand = symptomatic
Like with exertion
Fully occlude
ALWAYS symptomatic
Supply ALWAYS less than demand
Stable angina
Chest pain at times of increased myocardial O2 deamnd
Relieved by: Rest or NITROGLYC (vasodilator)
Due to fixed atherosclerotic plaque = ischemia
VERY COMMON, initial presentation for many people with CAD
Acute coronary syndrome
Acute results of CAD that are most often disruption of unstable plaques
Unstable angina = minor atherosclerotic plaque rupture
Myocardial infarction = major rupture atherosclerotic plaque
Necrosis or death of myocardial tissue (due to lack of blood/O2)
Severity: determined by ECG + lab results
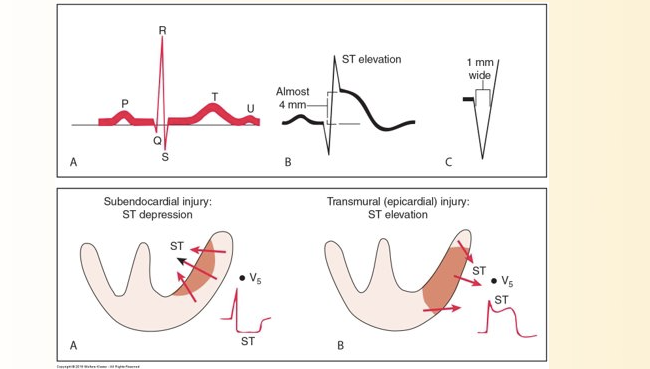
EKG Changes of Acute Coronary Syndrome (ACS)
ST seg elevation
T wave inversion
Development of Q wave
T wave + ST seg, ventricular repolarization USUALLY first affected by myocardial ischemia + infarction
Serum Biomarkers/ Cardiac Enzymes
Increased cardiac enzymes = increased cardiac myocyte damage
Troponin I, troponin T, and creatinine kinase, and myoglobin
Biomarker timelineORDER = MTC
Myoglobin elevated 1 hour after myocardial cell death (peak 4-8 hr)
Troponins rise 3 hours after onset of MI (stay 7-10 day)
CK-MB elevate 4-8 hours after myocardial injury (stay 2-3 day)
Unstable angina/ NSTEMI (partial blockage)
NSTEMI = Non St seg elevation MI
Chest pain:
At rest
Minimal exertion
Worse chest pain than before
NO ST seg elevation
Can involve infarction, but with NO ST seg changes
MUST look at serum biomarkers with NSTEMI
STEMI
ST elevated + Full blockage
Necrosis of myocardial tissue, causing SEVERE pain
Tranmural infarction = full thickness of ventricular wall (EKG + labs needed)
Prolonged, nitroglycerin does NOT help
Jaw pain, arm pain, GI complaints (NV)
Consequences of major plaque rupture
Complication
Replacement by fibrous tissue (less elastic_
= decreased contractility of heart
Can develop rupture of papillary muscles, heart wall rupture (bc cant strech)
STEMI S/Sx
Ischemia/infarction
Severe pain
Pale,cool skin
Nausea, vomiting
Dyspnea
Organ dysfunction (heart)
Fatigue
Pale,cool skin
Dyspnea
Hypotension
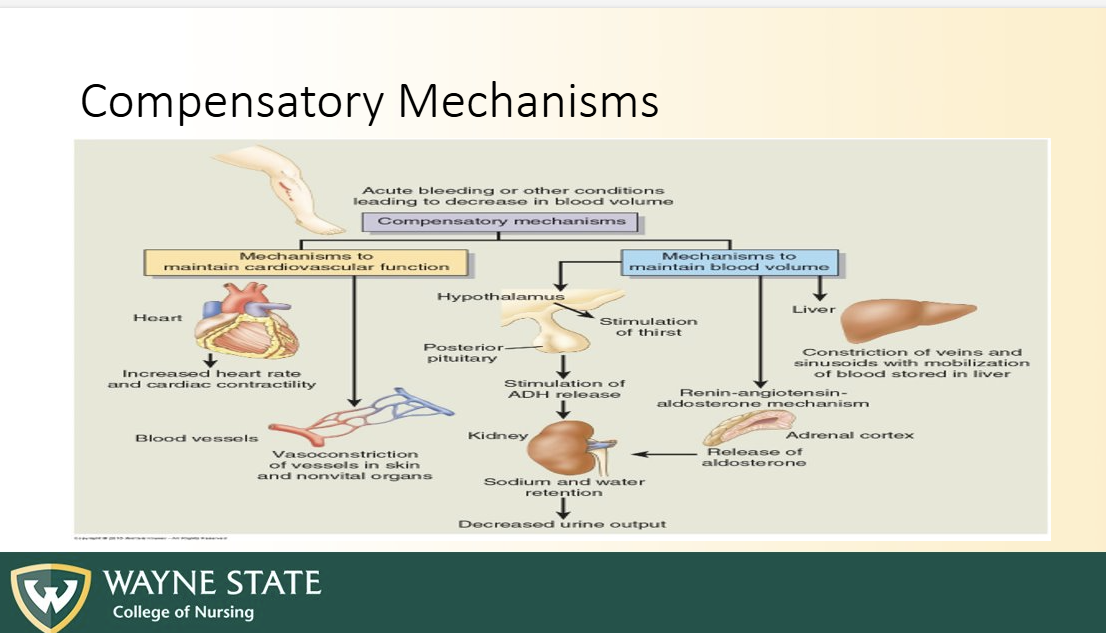
Compensatory mechanism/ SNS
Tachycardia
Heat sounds
S1
Tricuspid + mitral valve closure
These are AV valves
LUB
S2
Pulmonary + aortic valve closure
SL
DUB
Heart Murmur
Sounds caused by TURBULENT BLOOD FLOW thru heart or great vessels
Commonly due to valve deformities, dysfunction, or defects in heart wall (ASD, VSD)
OR by backflow of blood
Valve Defects (2)
Stenosis
Valve wont open all the way
HARDER to force blood = inc afterload??
Murmur of blood shotting through narrow opening
Regurgitation (insufficiency)
Valve NOT CLOSE all the way
Leaks
Murmur of blood leaking
Valvular disorders (4, 2 for each valve)
Mitral stenosis
Mitral insufficiency/prolapse
Aortic stenosis
Aortic insuffiency
Mitral Stenosis (2 pathways)
Narrow MV, does NOT eject enough blood in LV during DIASTOLE
2 part impacts
Blood congestion in LA (2 parts)
Blood backup
= increase in hydrostatic pressure
= edema in lungs
= dyspnea, cough orthopnea
Dilated LA
= overstretched myocardium
= atrial fibrillation
= thrombus formation in LA
= Ischemic stroke
Less output to LV
Decreased SV and CO
Ischemic heart
Mitral Insufficiency (2 pathways)
MV doesn’t close completely = leaking blood in LA during systole
Blood congestion in LA (2 parts)
Pulmonary congestion
Blood flows back in LA from LV
LA congestion
Pulmonary vein congestion
Inc hydrostatic pressure
Pulmonary congestion + edema
Dyspnea, cough, orthopnea
Overstretched LA
Atrial fibrillation (take blood thinners to prevent thrombus)
Thrombus formation (bc blood pools up and cant move)
Less output output LV
Decreased SV CO
Chest pain + faitgue
Aortic stenosis (2 pathways)
Narrowed Aortic valve opening does NOT enject enough into aorta during systole
Blood backup into LV
LV congstion
LA congestion
Pulm vein congestion
Pulm edema
Pulm congestion
Exertion dyspnea
Forward (2 things)
Less output to aorta
Dec SV,CO
Ischemic chest pain, MI
Inc afterload
LVH, LVF
Aortic Insufficiency
Aortic valve does NOT close completely
Leaks blood into LV during diastole
2 pathways
Backup
Blood backups into LV
Blood backups into LA
Pulmonary congestion
Exertional dyspnea
Forward
Less output to LV (BC ITS ALREADY FULL??)
Decreased SV, CO
Chest pain, fatigue, syncope
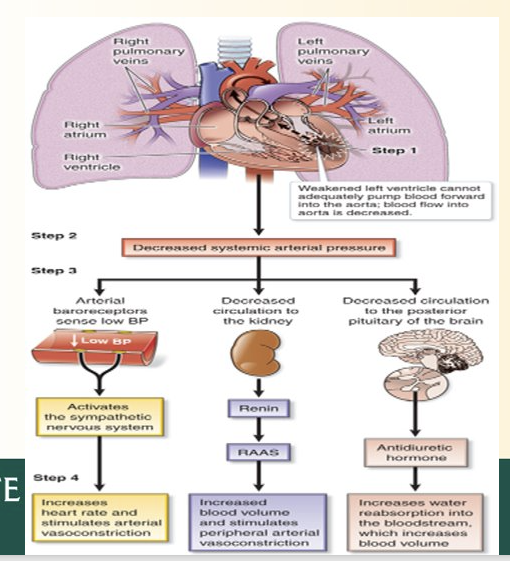
Heart Failure (3 types)
Weakened ventricular muscle CANNOT pump blood into arterial circulation well enough
Most common cause of hospitalization
3 types
Right side vs left side heart failure
Systolic vs diastolic dysfunction
Backward vs forward failure
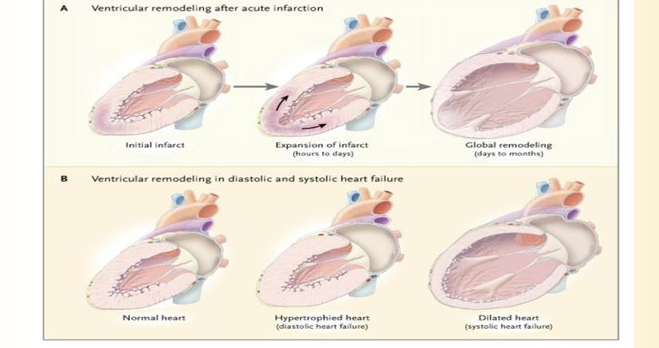
Systolic vs Diastolic
Systolic = NOT ENOUGH OUT
Weak ventricle cant pump enough out
Dec empty = Dec CO + SV
Blood accumulation + backup into atrium = INCREASED PRELOAD ?? why, not blood coming in its the total blood
Diastolic = NOT ENOUGH BLOOD IN
Stiff ventricle is less elastic = cant accept enough blood
Dec EDLVV = Dec CO + SV
EDLVV (end diastolic left ventricular volume)
Backward vs Foward effects
Backward
Backup of blood into atriums + pulmonary vessels
LVF backup = pulmonary edema/congestion (MAKE SURE TO KNOW PROCESS FROM PREVIOUS SLIDES WILL BE ON EXAM)
=Dyspnea, cough, orthopnea SHORT OF BREATH LYING DOWN, paroxysmal (sudden) nocturnal dyspnea
Forward
Cant pump blood out
LVF = Dec SV, CO
Neurohormonal responses (RAAS, ADH, SNS)
Body thinks BP low due to some stuff and tries to compensate
Fluid retention + weight gain
Orthopnea
LVF patients = difficulty breathing when lying flat (dyspnea)
Fluid congestion in lung tissue
Pt must sleep upward
When propped up, fluid in lungs remain in bases = easier to breathe
Paroxysmal Nocturnal Dyspnea (PND)
Patient with HF awake in middle of night SUDDENLY
Due to pulmonary fluid buildup = hypoxia while sleep
= Smothering feeling or nightmare
Forward vs backward effects of LVF
Backward LVF = pulmonary congestion pathway
Forward LVF Steps
Cant pump enough blood into aorta
Decreased systemic arterial pressure
Renin, ADH, and SNS stuff activate from earlier
Causes fluid retention, increased BP, Incrase HR, Increase Vasoconstrict, etc.
Right Ventricular Failure (RVF)
Blood backup into RA, SVC (sup vena cava) and IVC
Leads to
Jugular venous distension (Bulging jugular vein)
Ascites (crackles)
Hepatomegaly (hepatic venous congestion)
Splenomegaly (splenic venous congestion)
Ankle or sacral edema
Backward effects are MOST apparent on physical examination (edema and distension, ascites, etc.)
HF compensatory mechanisms (5)
Frank starling
SNS
RAAS
ADH
Myocardial remodeling/muscle building
Frank Starling Mechanism (HF Comp)
Increasing SV through increase in end diastolic volume/preload
As SV + CP increase, Preload inc (VICE VERSA)
Increased filling = increased force of next contraction
SNS (HF Comp)
Steps
Dec Bp
Baroreceptor activate
SNS activate
Vasoconstriction
Increased HR?
Look back at old slide
RAAS (HF Comp)
Same as before
ADH (HF Comp)
Same as before
Myocardial Remodeling
Heart becomes hypertrophic due to increased demands
Then decreased imated ???due to systolic heart failure
Heart Failure Signs and Symptoms
Hemodynamic measuremnt changes in HF
Central venous pressure (pressure in vena cava)
Cardiac output decrease
Increase pulmonary capiallry pressure
Left ventricular ejection fraction (vol ejected/vol in LV)
Systemic BP Decrease (dec BP = dec CO)
Pharmacological treatment of HF (5)
ACE inhibitors/ angiotensin receptor blockers = vasodilation = dec afterload
Beta blockers = dec HR
Diuretics = inc excretino = low blood vol = low preload = low workload
Digitalis = inotrophic = supports contractility
Nitrates = vasodilation = dec afterload
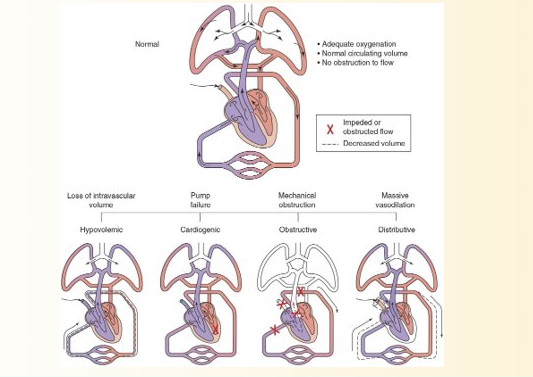
Shock/ circulator failure
Failure of circulatory system to supply O2 and nutrients = cellular hypoxia
Decreased CO, hypotension, hypoperfusion
4 types of shock
Hypovolemic = loss of intravascular volume
Cardiogenic = pump fialure
Obstructive shock = mechanical obstrucitn of blood flow through central circulation
Distributive shock = massive vasodilation
BE FAMILAR WITH EACH, LOOK AT PICTURE
Shock Compensation (3 types)
Shock = dec intravascular volume, heart fails to pump blood, or extensive vasodilation
Causes dec CO, SV, and BP
SNS: Vasoconstriction = Inc HR + contractility
RAAS = angiotensin II + aldosterone (what these do again)
ADH: what do again