kines 330 unit 4
1/165
Earn XP
Description and Tags
shoulder complex,
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
166 Terms
shoulder anatomy
ball and socket joint
consists of 3 bones
flat areas contain deeper muscles (scapula)
what helps to keep the ball in the shoulder socket?
ligaments
labrum
capsule
increased ROM =
decreased stability
muscle contractions of the shoulder help to dynamically ____ the joint
control
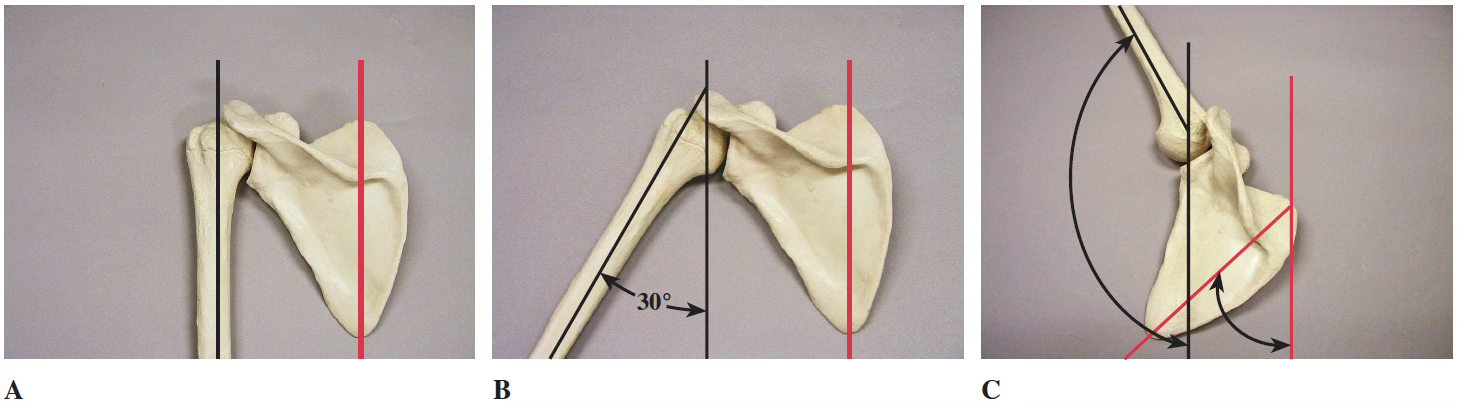
Scapulohumeral Rhythm
The movement of the scapula is relative to the humerus
first 30 degrees of glenohummeral (GH) abduction is all on its own (no scapular motion)
30-appx 120 degrees, there is a 2:1 ratio of GH: scapula movement
120-180 degrees is a 1:1 ratio
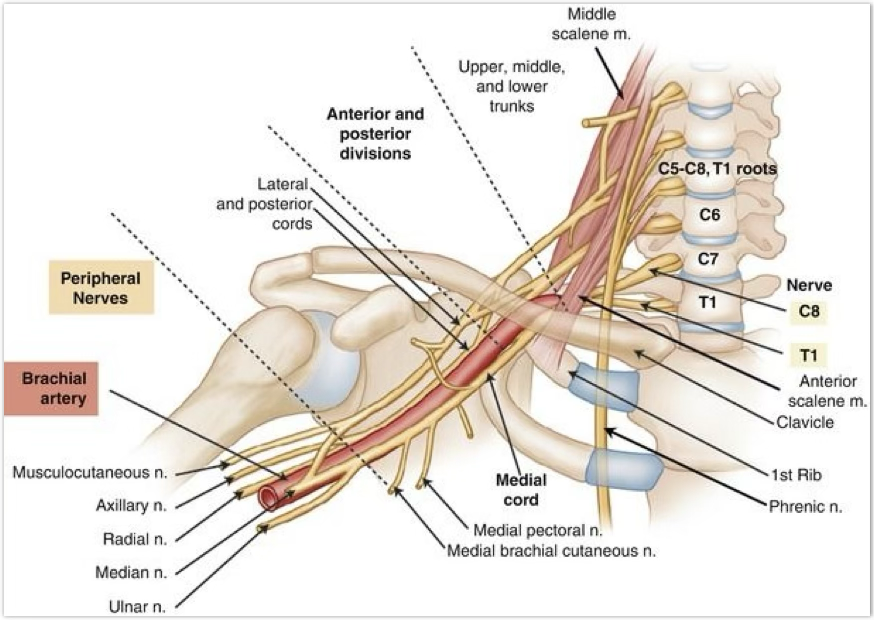
brachial plexus
starts at cervical and runs under clavicle
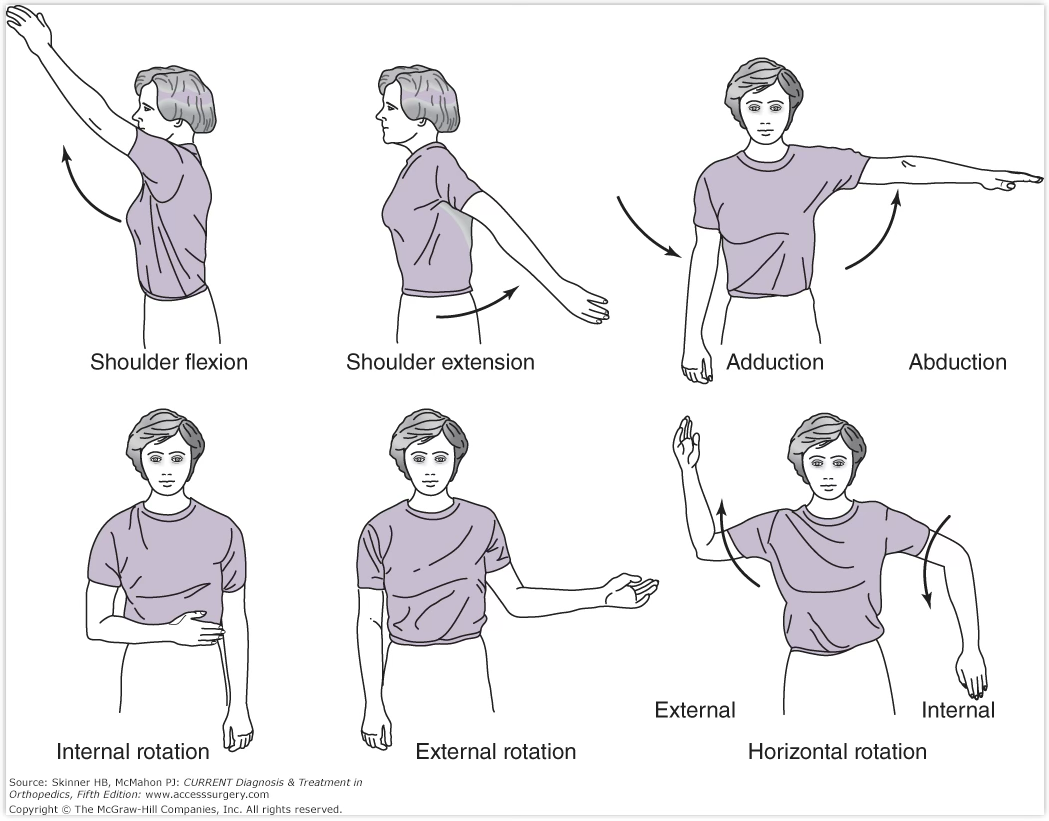
Shoulder ROM: GH joint
flexion
extension
abduction
adduction
internal
external
horizontal rotation
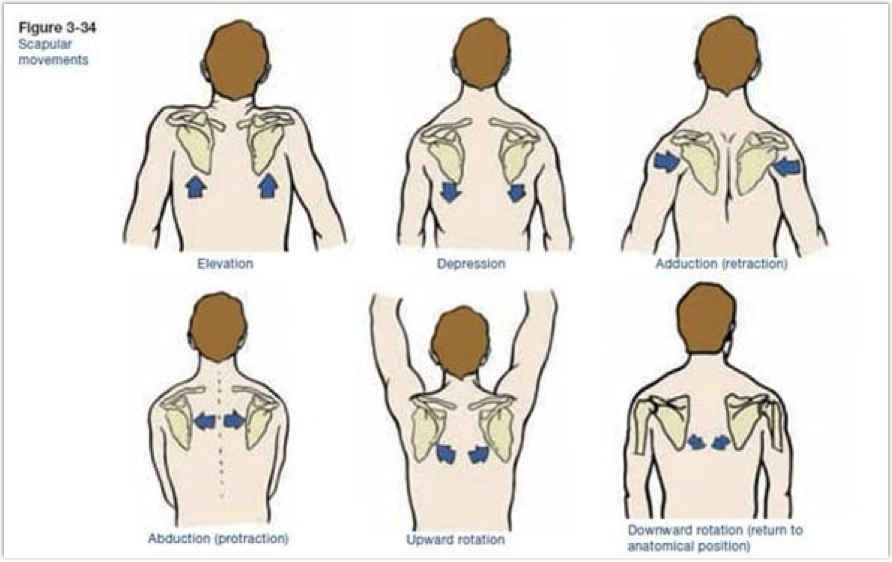
Shoulder ROM: scapular
elevation
depression
adduction
abduction
upward rotation
prevention of shoulder injuries
proper physical conditioning is key
proper warm ups that include a full ROM
especially for overhead activities or those doing explosive arm movements
think tubing exercises, medicine balls, weighted water
helps with activation of rotator cuff muscles as well as scapula and humeral muscles
focus on follow through
teach how to fall, proper throwing/throwing/dance/stunt/serving/spiking/how to hold instruments techniques
protective equipment and braces
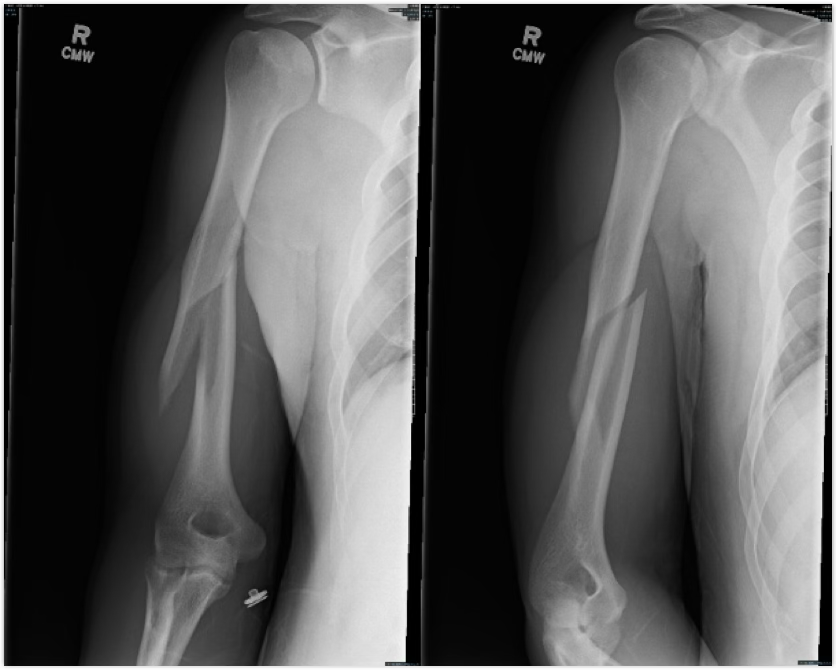
how do humeral fractures occur?
tends to occur with a direct blow or foosh, and can fracture with an eccentric load
watch for growth plate fractures as well
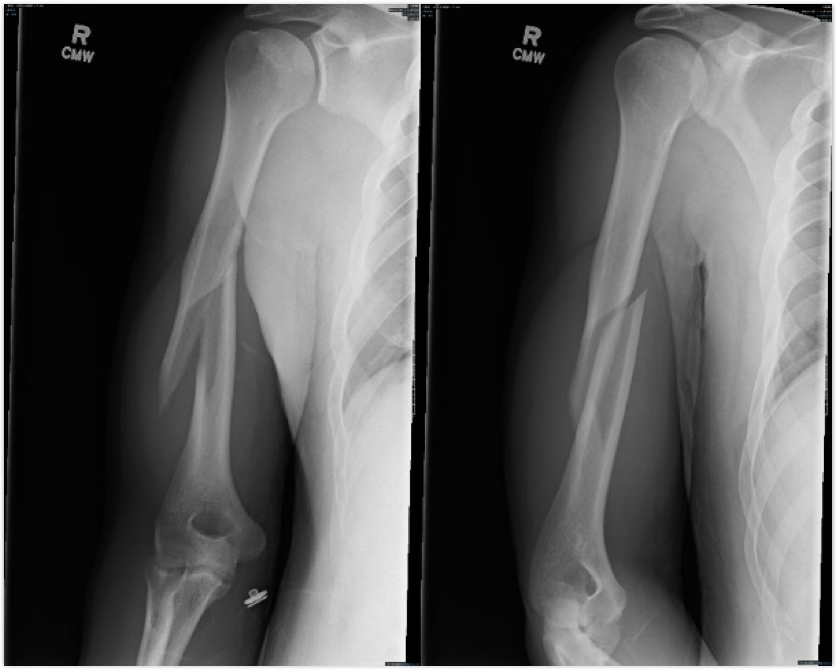
symptoms of a humeral fracture
deformity, pain, swelling, decreased ROM
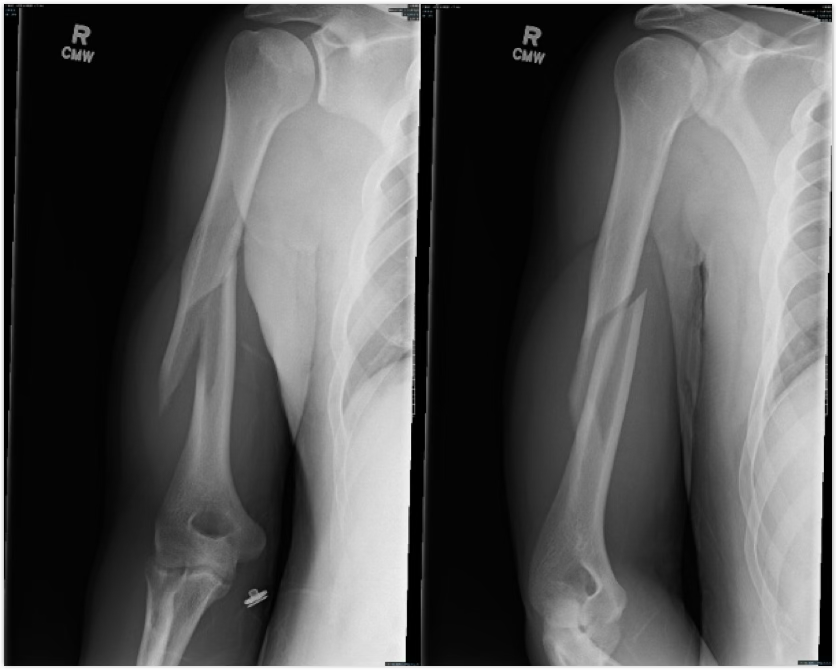
treatement of a humeral fracture
splint and ship off for a cast or surgery
tends to be 4-8 wk heal time

how does a clavicle fracture occur?
falling on outstretched hand or a direct hit

symptoms of clavicle fracture
pain, deformity, lack of ROM, swelling, and a snap

treatment of clavicle fracture
Check for neurovascular injuries
If in alignment, they get a figure 8 brace or sling and eventually PT
If not in alignment, they get new hardware, sling, and PT

how does a SC sprain occur?
force on outside shoulder

SC sprain symptoms
anterior is better, posterior will cause trachea to be compressed and loss of breathing
grade 1: might be pain and discomfort
grade 2: possible deformity and lack of ROM
grade 3: deformity

treatment of SC sprain
sling and ship for imaging, might be 3-5 weeks in sling/brace with gradual PT
how does an AC sprain occur?
foosh or blow to outer shoulder
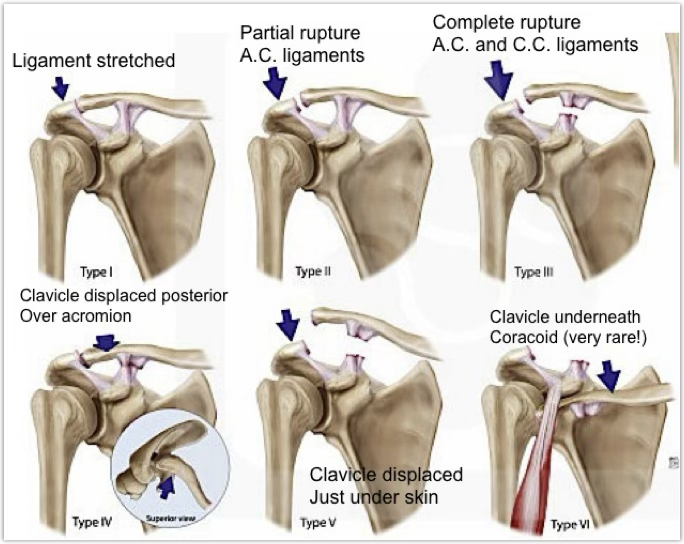
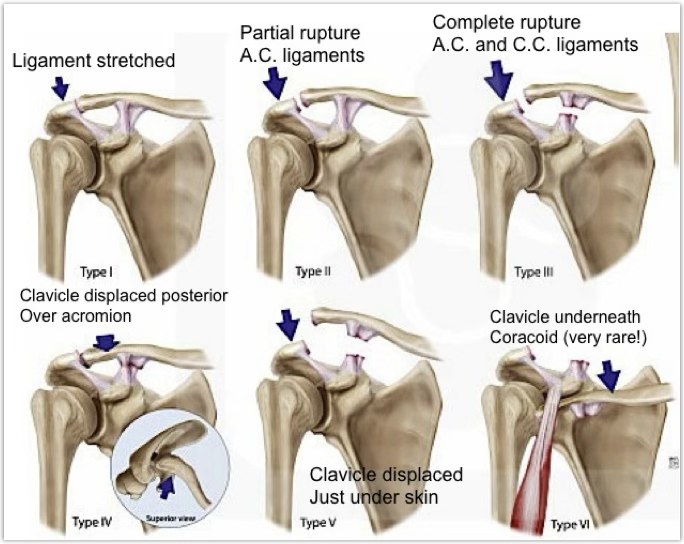
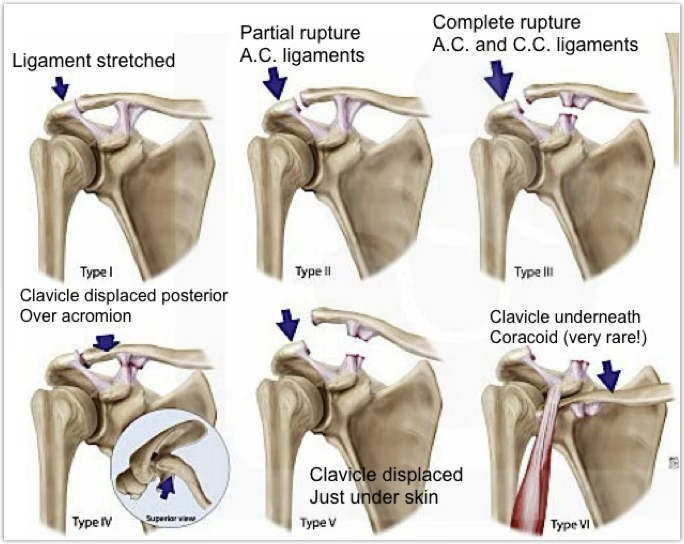
symptoms of AC sprain
grade 1: ligament stretched
grade 2: partial rupture A.C ligaments
grade 3: complete rupture A.C and C.C ligaments
grade 4: clavicle displaced posterior over acromion
grade 5: clavicle displaced just under skin
grade 6: clavicle underneath coracoid (very rare)
AC sprain treatment
stabilize and ship for imaging to see how to best treat
grades 1-3 tends to be sling and gradual PT after apprx. 2 weeks
grades 4-6 are surgical
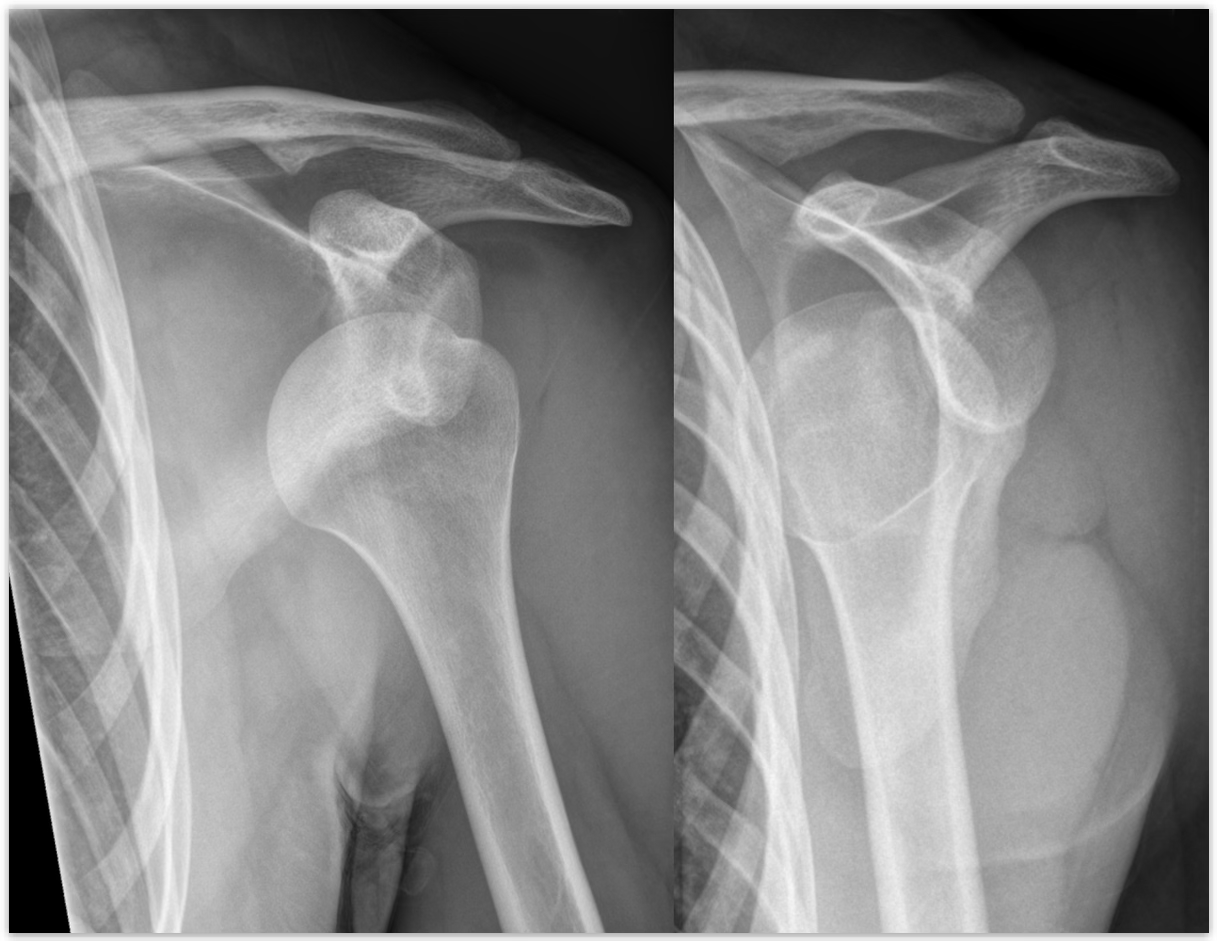
how does a GH Subluxations/Dislocations occur?
force on shoulder, can have anterior (most common), posterior, and inferior (rare) dislocations
GH Subluxations/Dislocations symptoms
A sublux will have pain, limited ROM, while a dislocation will have a deformity, pain, and no ROM
GH Subluxations/Dislocations treatment
If trained, reduce it and ship; if not, splint and ship
first time dislocation = always suspect a fracture
chronic inj. = may brace to reduce the chance, as the labrum is torn
person needs to keep up with a rehab plan, as the dynamic muscles are the best thing to keep the GH head in
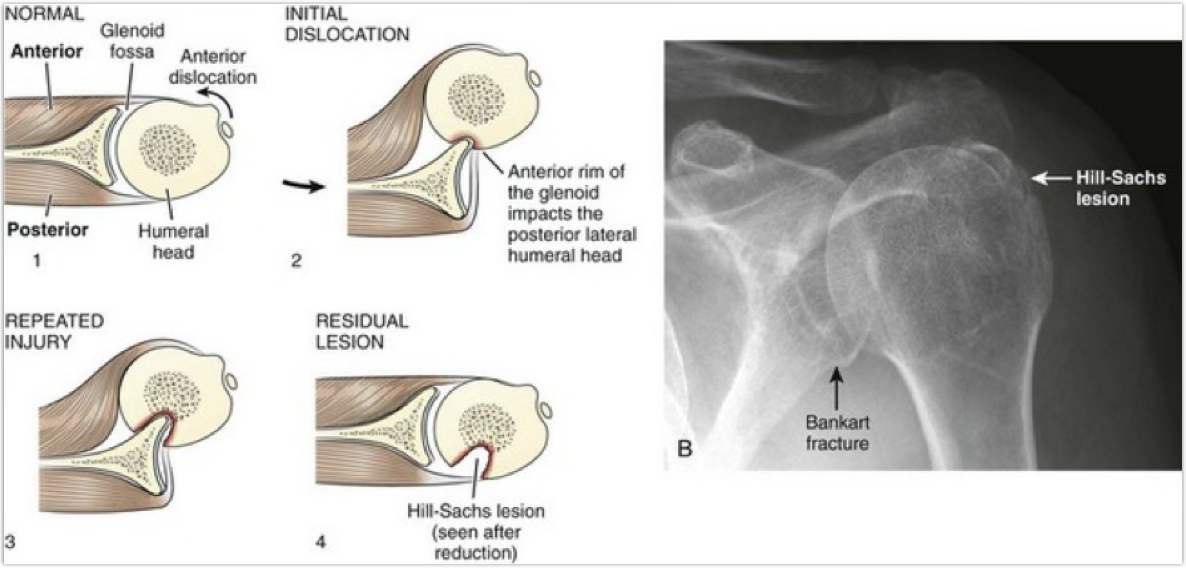
bankart lesion
anterior defect of labrum
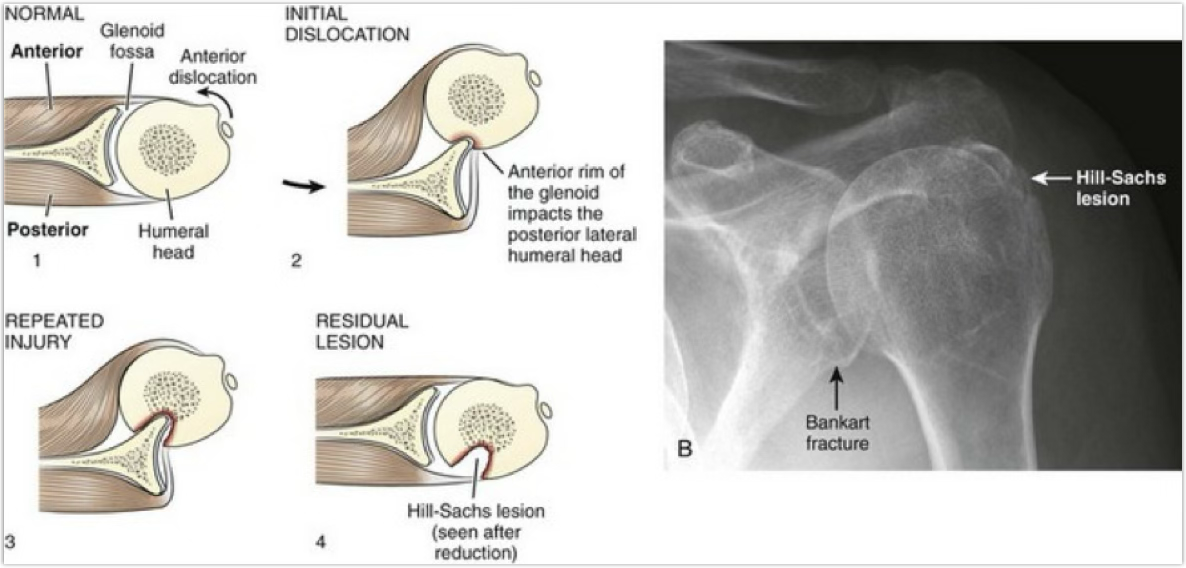
hill sachs lesion
divot in humeral head
what are complications of GH dislocations?
Hills sachs and bankart lesion
how are Hills Sachs and Bankart lesions treated?
surgeon will try to fix these is the GH patient ops for surgery to fix their labrum
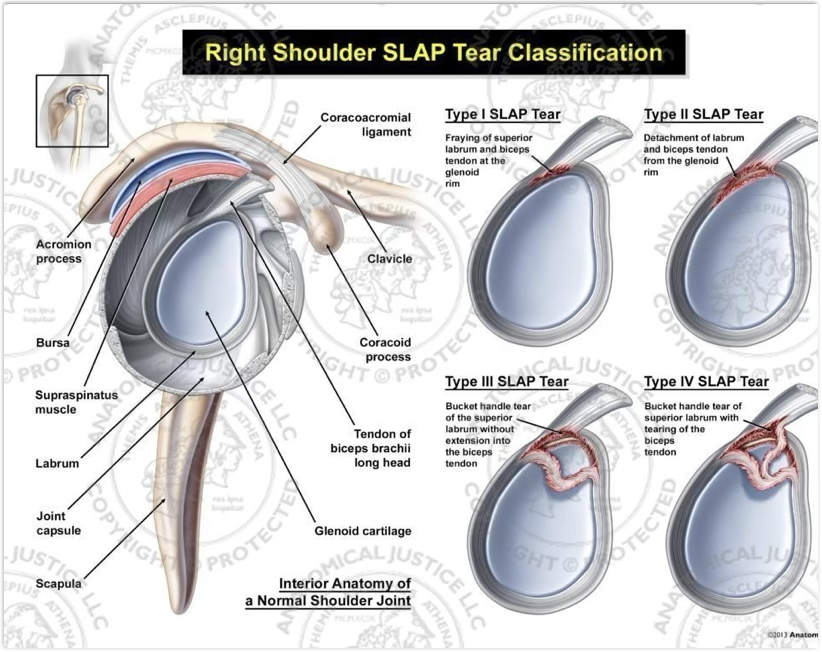
how does a SLAP lesion occur?
can occur due to dislocation or on it’s own
labral tear that has a specific location (superior labrum anterior to posterior)
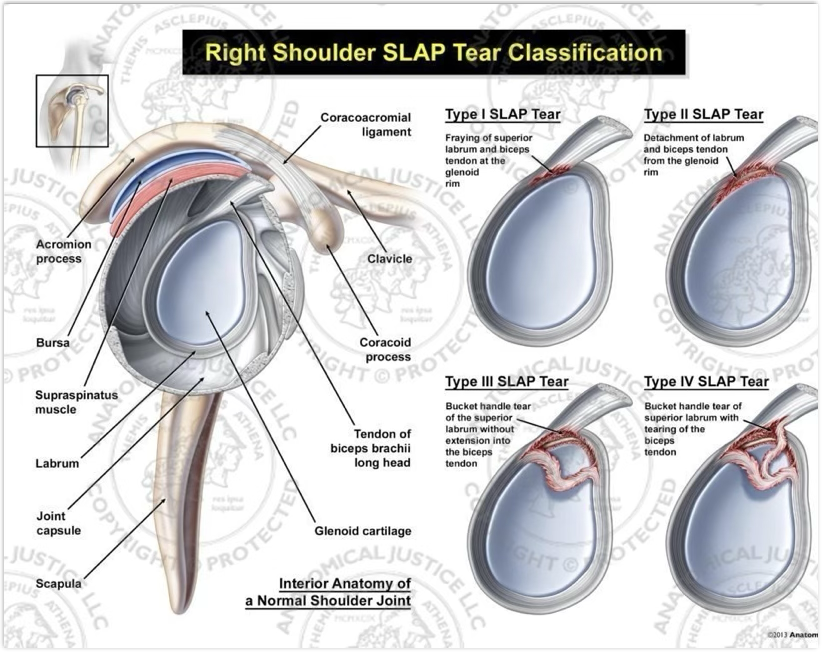
SLAP lesion symptoms & treatment
A defect in the superior labrum that begins posteriorly and extends anteriorly, which means it will affect the long head of the biceps
Bicep movements will tear the labrum more
4 types of tears, last 2 focus on the biceps tendon
most are surgical cases
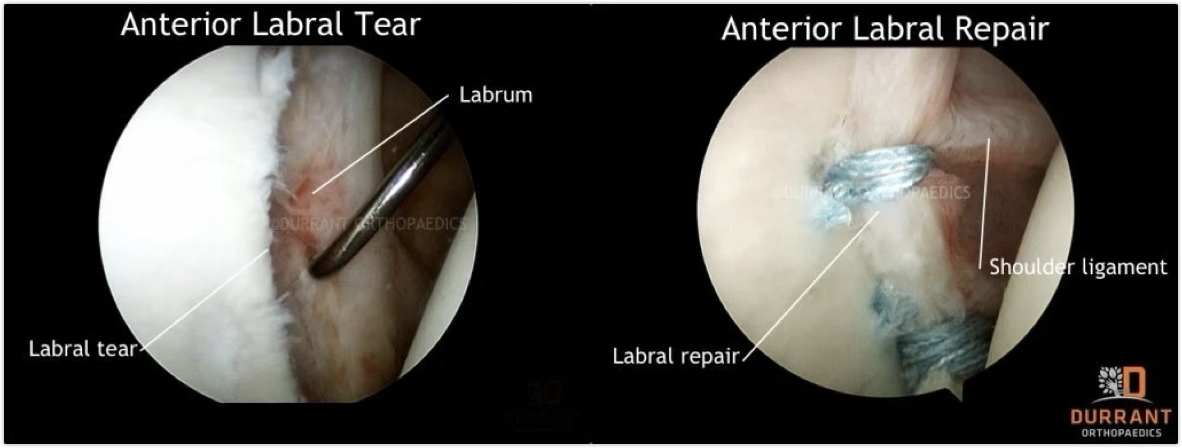
how does a GH labral tear occur & symptoms?
may complain of grinding, catching, pain deep in the shoulder, and instability
can have soreness post-eccentric contractions
tends to be overhead athletes
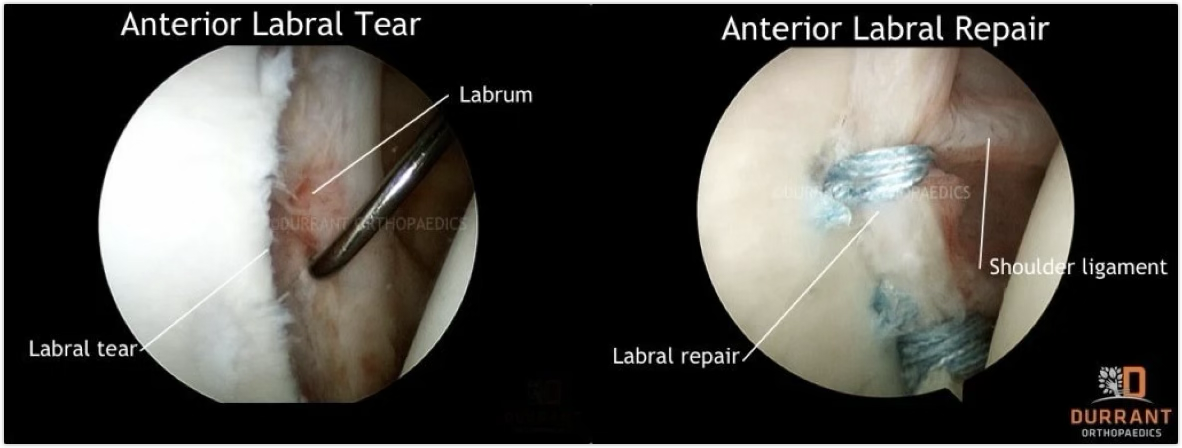
GH labral tear treatment
might be surgically repaired esp. if patient begins to sublux or dislocate
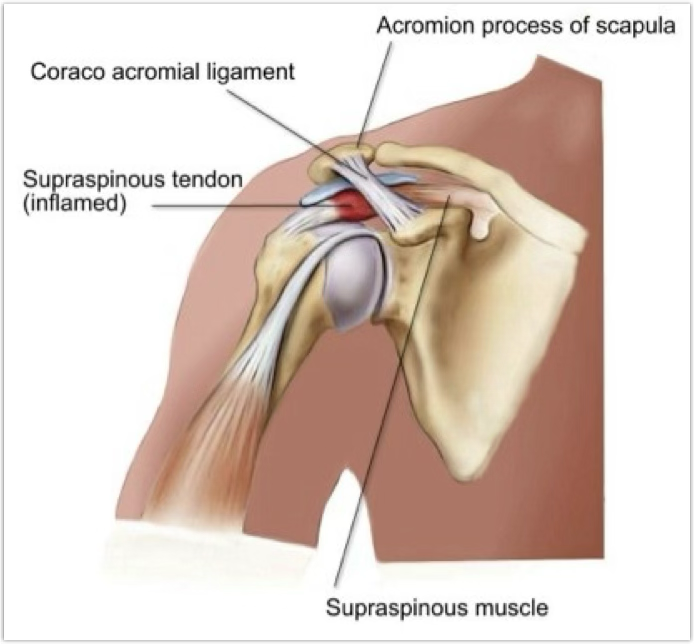
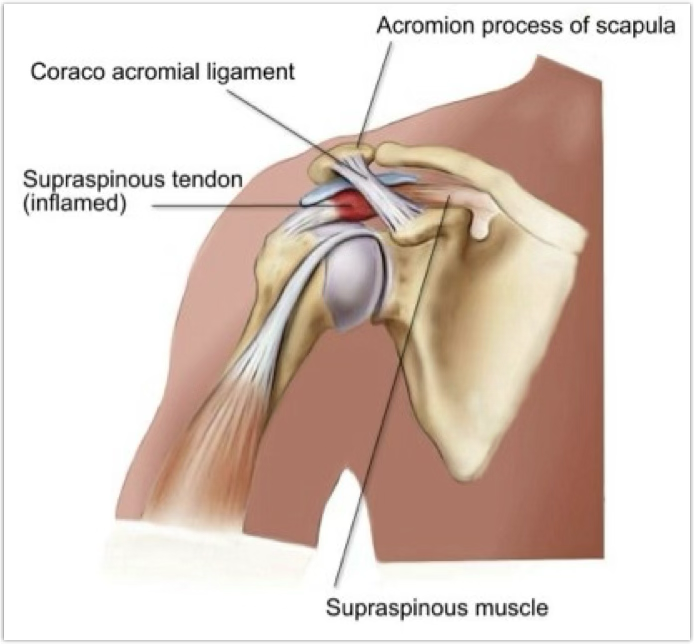
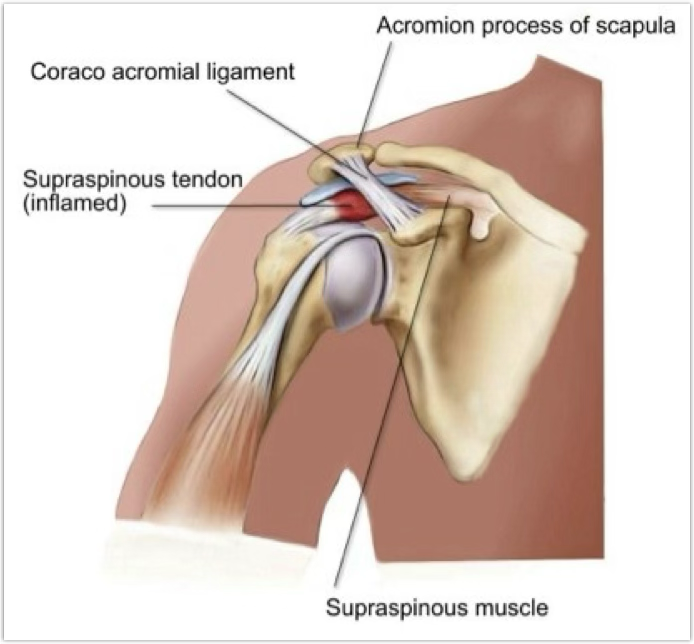
how does a impingement occur?
compression of the supraspinatus tendon, subacromial bursae, or long head of the biceps tendon as the space below the coracoacromial arch is limited (getting hit, an inflamed area)
seen a lot in overhead athletes
symptoms of impingement
pain that comes over time, increased GH ER with decreased GH IR
treatment of impingement
if we let it rest, it tends to calm down
use modalities, stretches, and work on mild strength
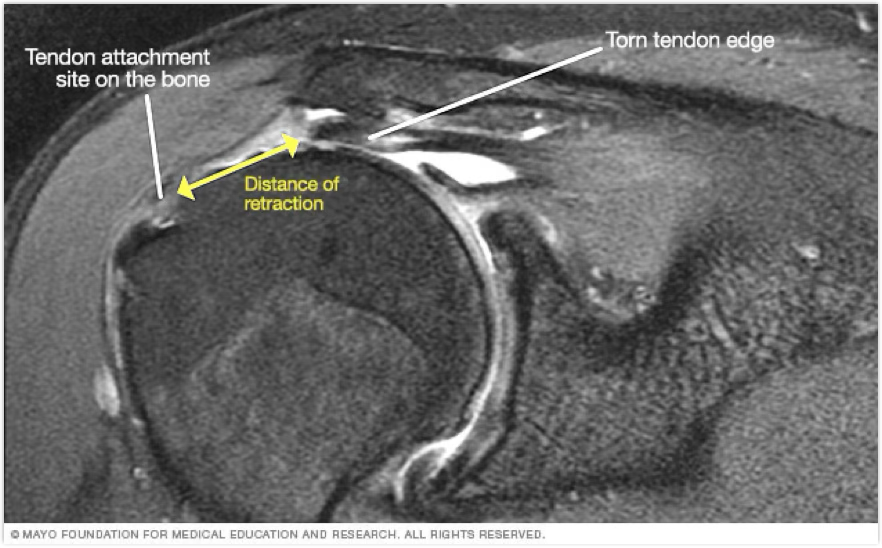
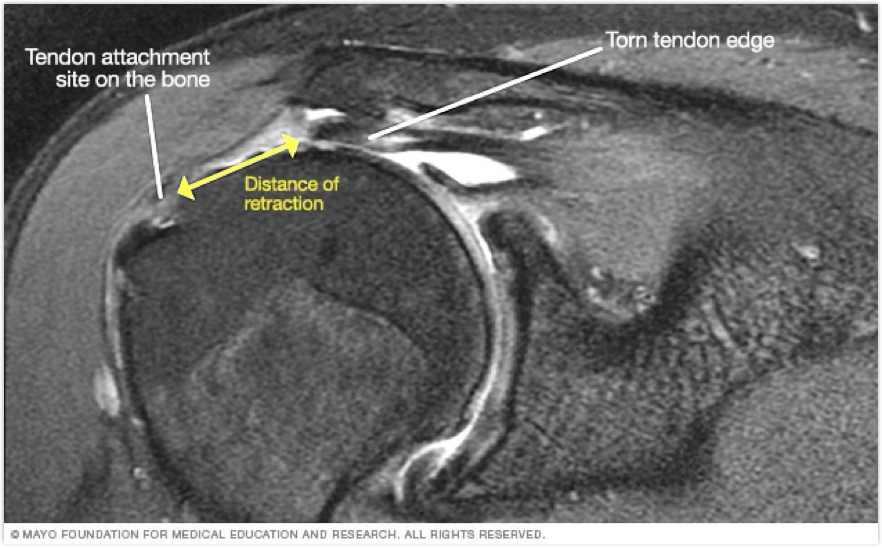
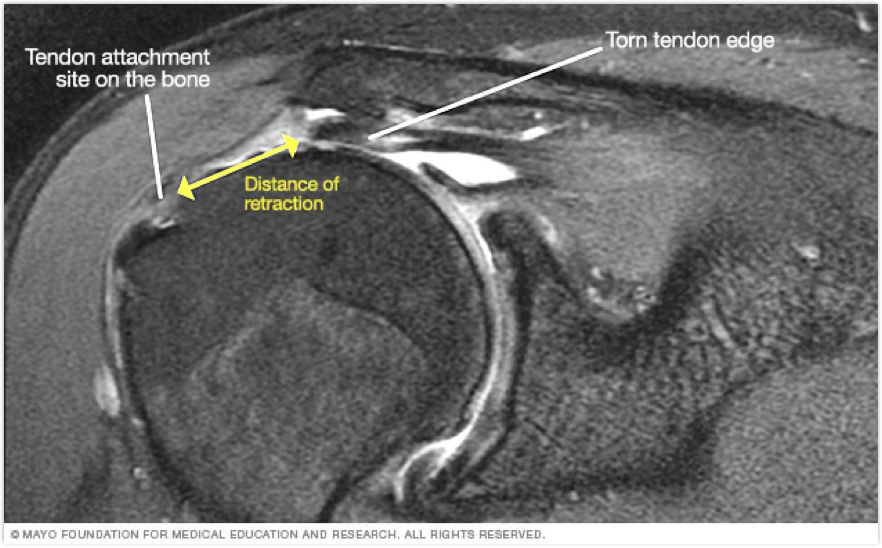
how does a rotator cuff tear occur?
tends to come at the insertion of the muscles
can be partial or full thickness tear
full thickness tends to be overhead athletes over 40 y/o with history of RC injuries
rotator cuff tear symptoms
pain and lack of IR/ER ROM
rotator cuff treatment
management depends on tear
Partial is conservative with PT
Full is surgical and immobilization
rotator cuff is how many muscles?
4

biceps tendon rupture occurance & symptoms
tends to be a powerful contraction where the bicep avulses off of insertion or origin
if it’s insertion area, you have little ROM and a popeye muscle
it it’s origin, you may still have ROM (as it has two heads)
both have pain, bruising, swelling and will feel a pop

biceps tendon rupture treatment
ice, splint and ship
tend to have surgery, but only exception is elderly at origin
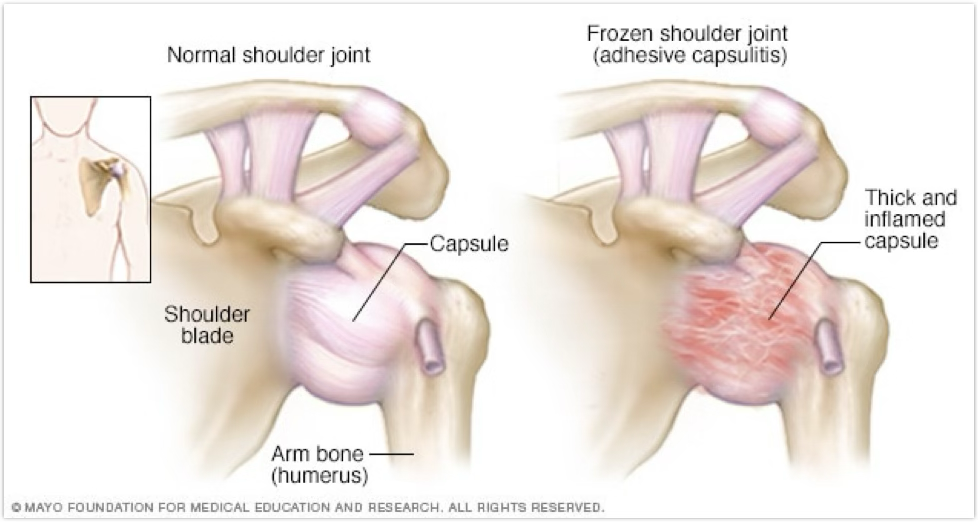
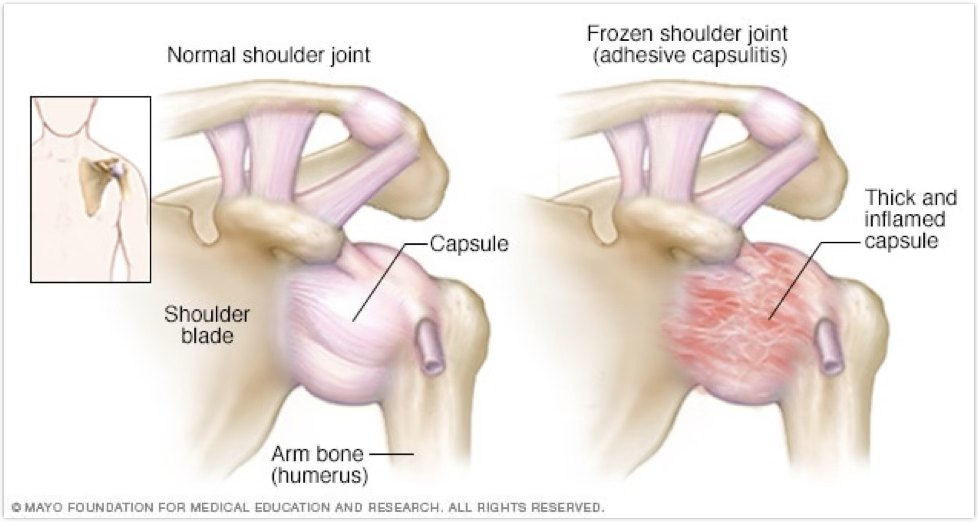
Frozen Shoulder/Adhesive Capsulitis symptoms & occurrence
joint capsule becomes thickened, contracts and becomes inelastic
pain with all motions no matter if active or passive
Frozen Shoulder/Adhesive Capsulitis treatment
might have to hurt the patient
aggressive joint mobs will be the best thing
use modalities to help with pain
have to stretch post-mob or else we lose what we gained
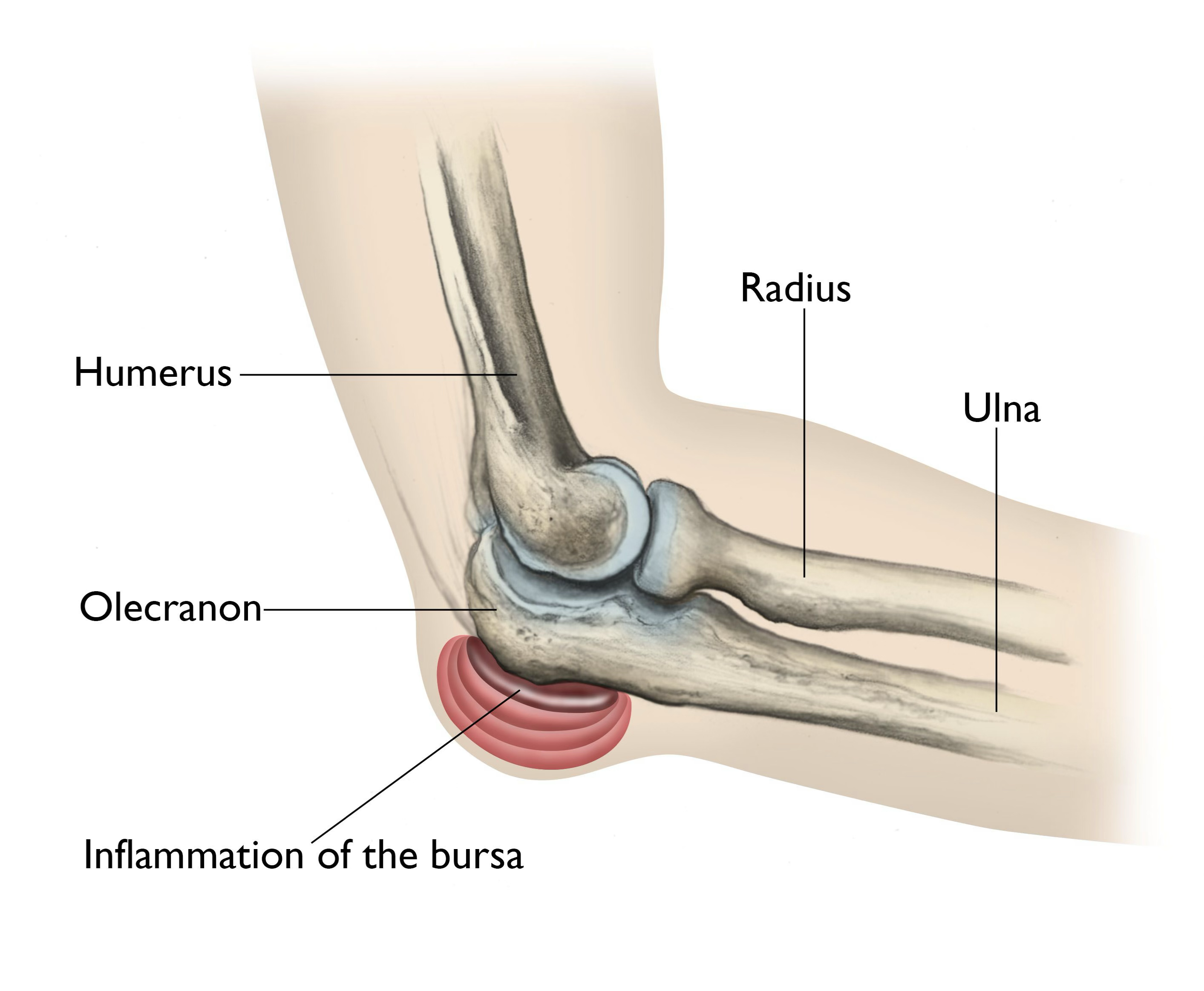
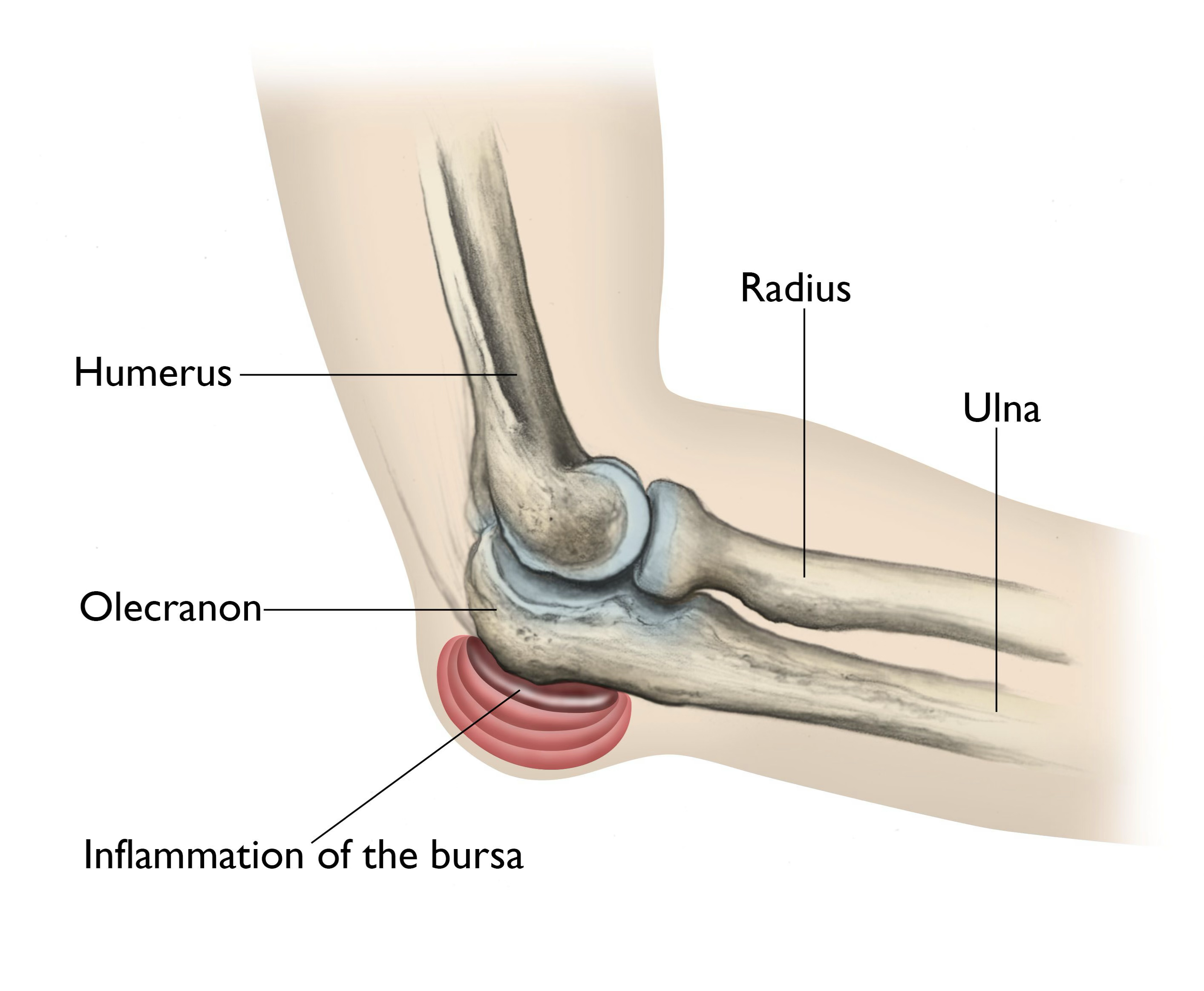
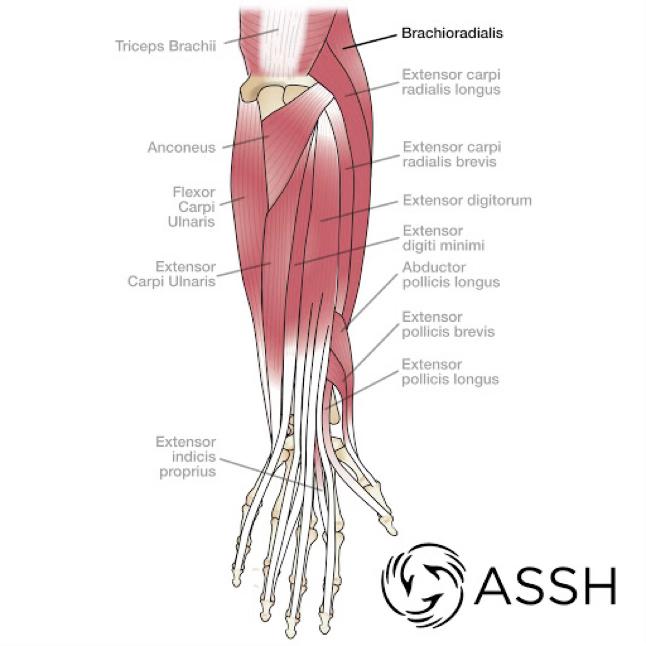
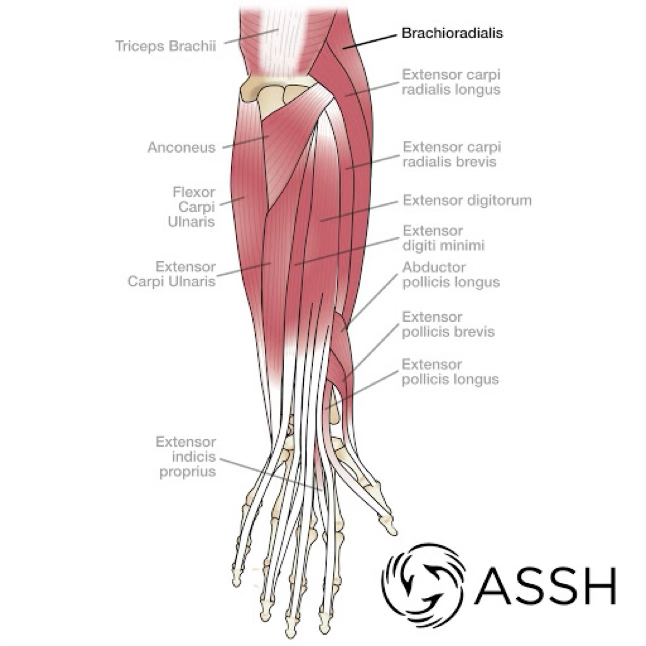
elbow and forearm anatomy & pathology
The radius and ulna have an interosseous membrane to help hold it together
3 bones have 3 joints: humeroulnar, humeroradial, and radioulnar
MCL/Ulnar ligament has 3 bands
LCL/Radial has 1 part
the elbow bones have what joint?
humeroulnar
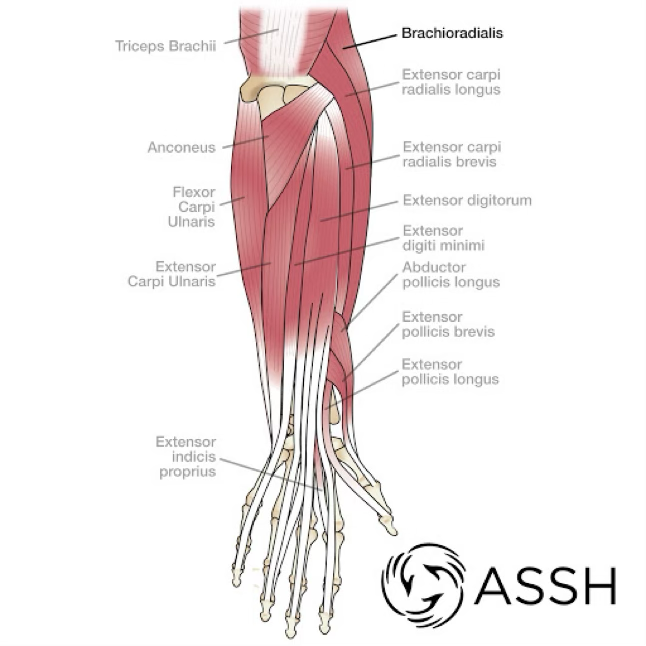
forearm flexor muscle
medial side
forearm extensor muscle
lateral side
vascular aspects of the elbow/forearm
vessels and nerves can’t go over the olecranon process so it wraps around
elbow & forearm ROM
145 degrees flexion
90 degrees supination or pronation
0 degrees extension (hyperextension can happen)
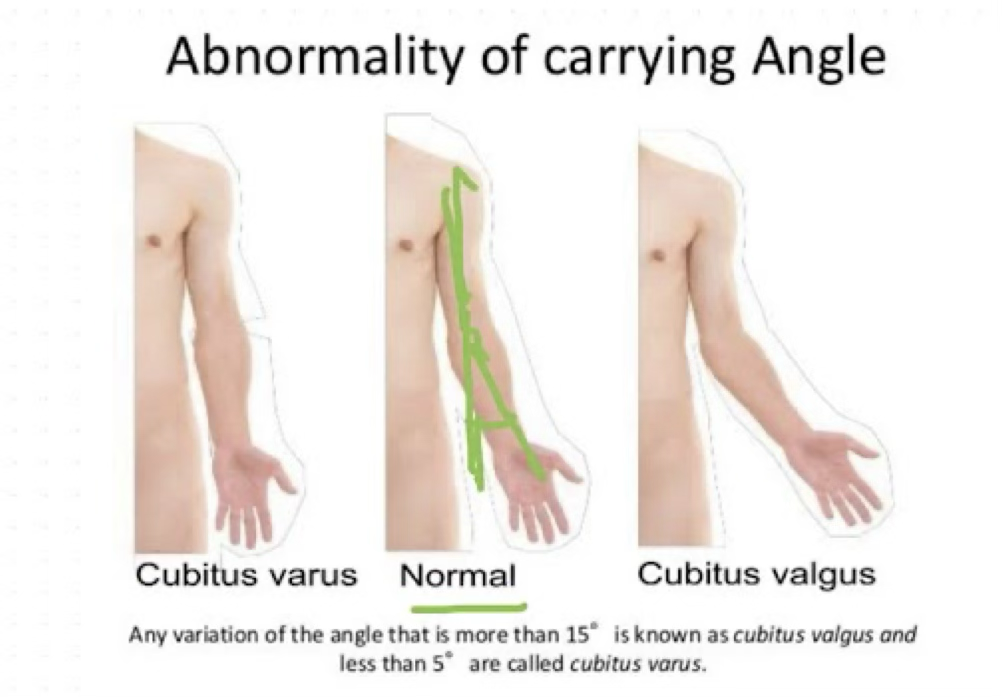
carrying angle of eblow
normal, it just tells us the distal projection of the humerus (hands cant slam into hips)
can see when we put someone in anatomical position
“normal” is 5-15 degrees, cubital varus is less than 5 degrees (closer to body), while cubital valgus is over 15 degrees
males are typically 5-10 degrees while women are 10-15 degrees
prevention of elbow/forearm injuries
braces help prevent injuries typically for a secondary injury
how to fall
FOOSH causes a mess for UE, try to teach how to brace without putting arm down
decrease overuse by cross training
if we cross train children, they have less injuries
also helps them to decrease their chances at burnout
proper biomechanics
adequate recovery
adolescent and post-injury— number of throws/hits & types
theres charts on this dependent on age, league, position, etc. we need these protocols so that kids don’t get overuse injuries
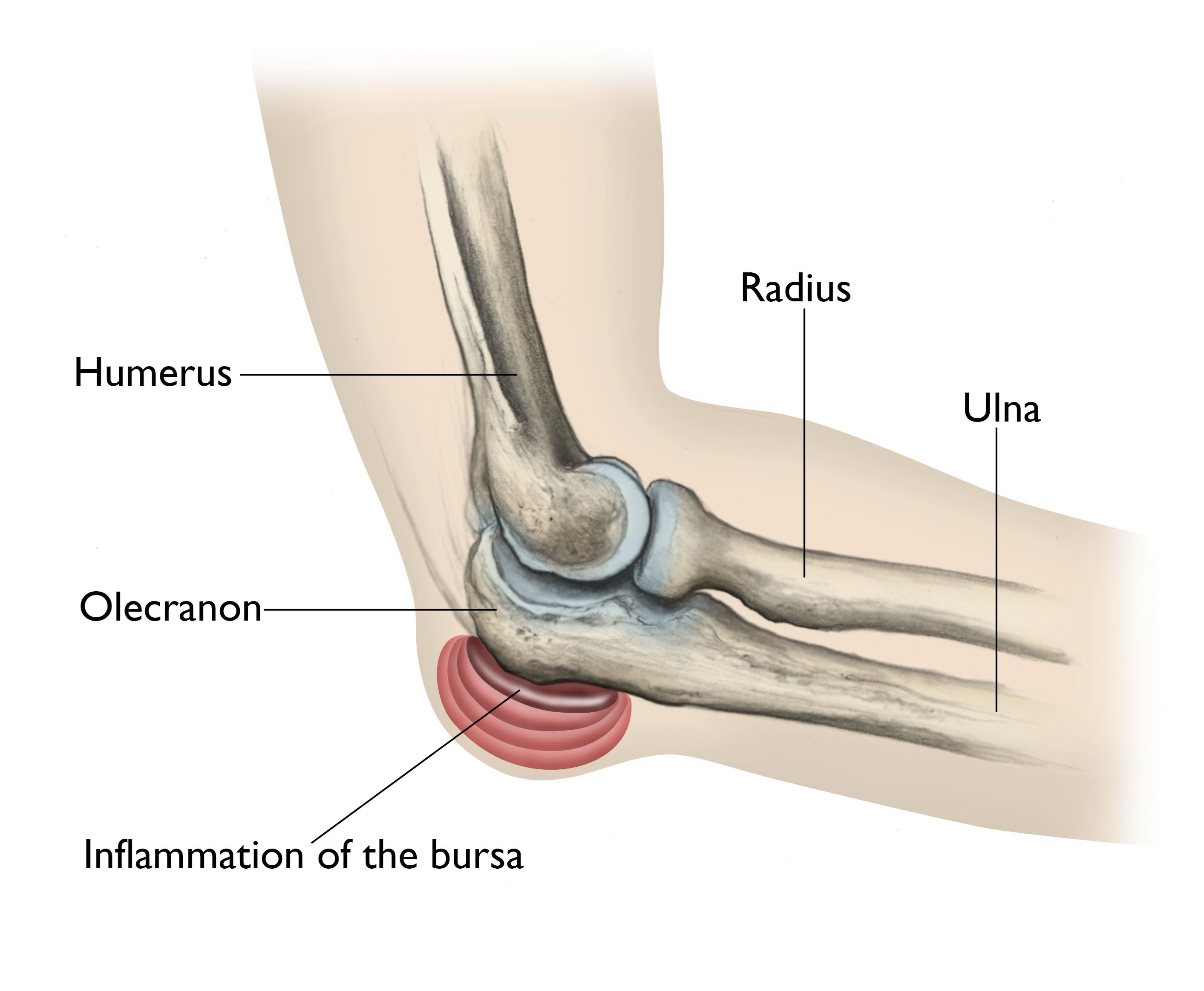
olecranon bursitis
as the bursae is superficial, we tend to injure it a lot with direct blows
symptoms of olecranon bursitis
mild pain, pressure, swelling, tenderness
treatment of olecranon bursitis
compress and ice it
if swelling doesn’t resolve, we can drain it
if athlete, we tend to pad the area so it doesn’t keep happening
muscle strains & avulsions
tends to occur with resistive motion or repeated microtears due to overuse
symptoms of muscle strains & avulsions
pain during motion as well as tenderness, reduced strength
treatment of muscle strains & avulsions
depends on the severity of strain, usually ice and rest works wonders
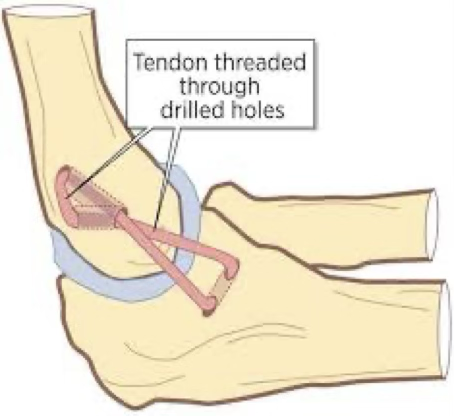
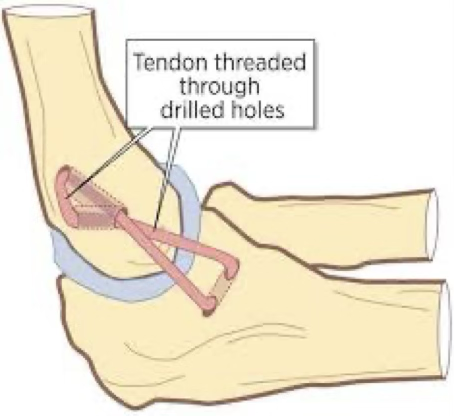
UCL sprain
UCL’s tend to rupture with valgus forces on the elbow
the more repetitive they are, the more microtears you get
symptoms of UCL sprain
can hear or feel a pop, pain and tenderness on medial elbow, possible tingling, and laxity at joint line
treatment of UCL sprain
in depth, if grade 1 or 2, we hope conservative treatment will scar the area and stabilize it
grade 3= 12-18 month rehab after surgery
throwing athletes can return to activity 22-26 weeks post-surgery with full recovery at 18-24 months
grade 3 rehabs are slow for a reason for overhead athletes
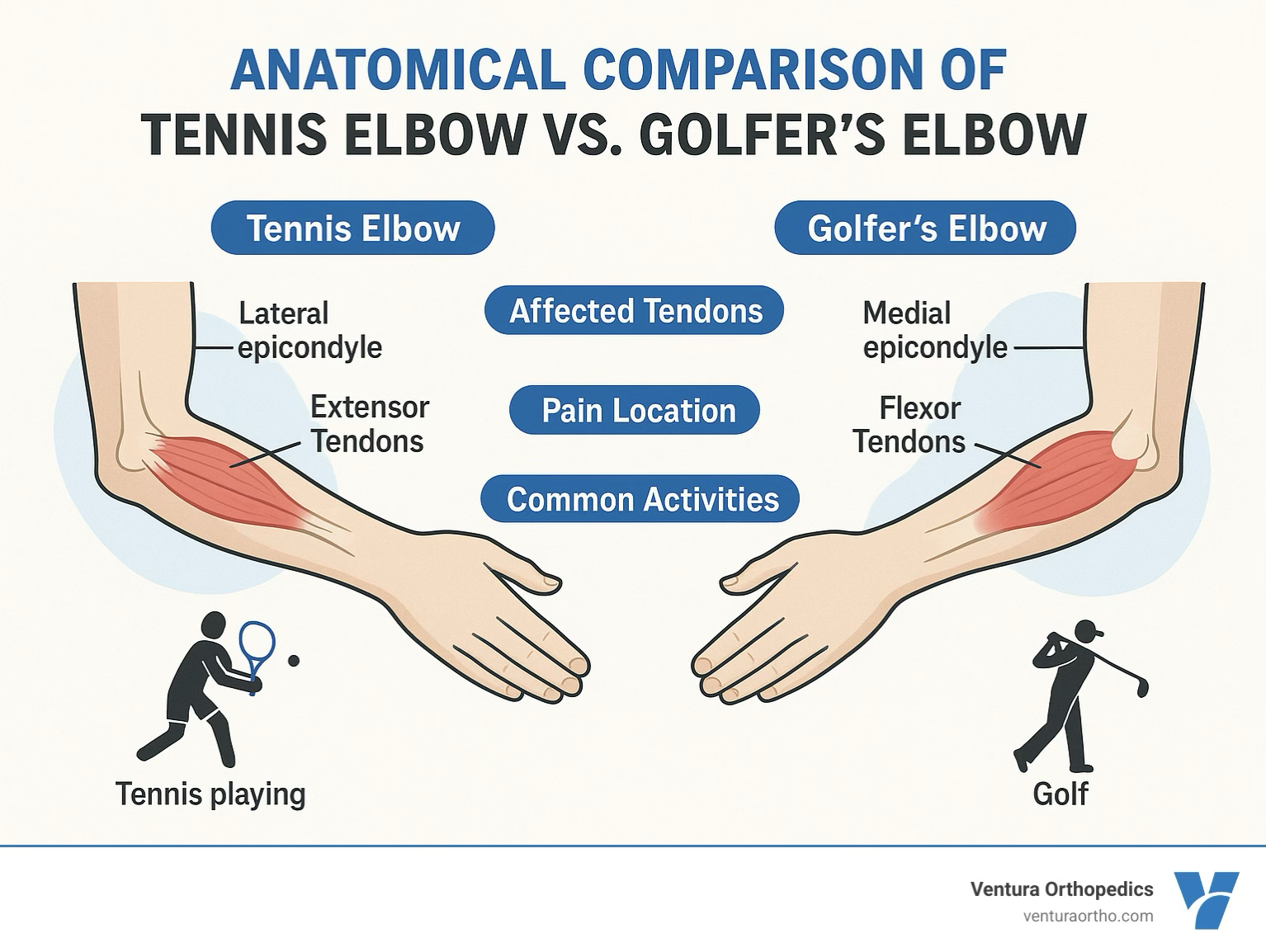
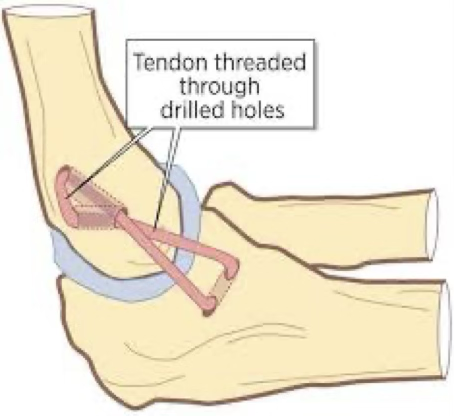
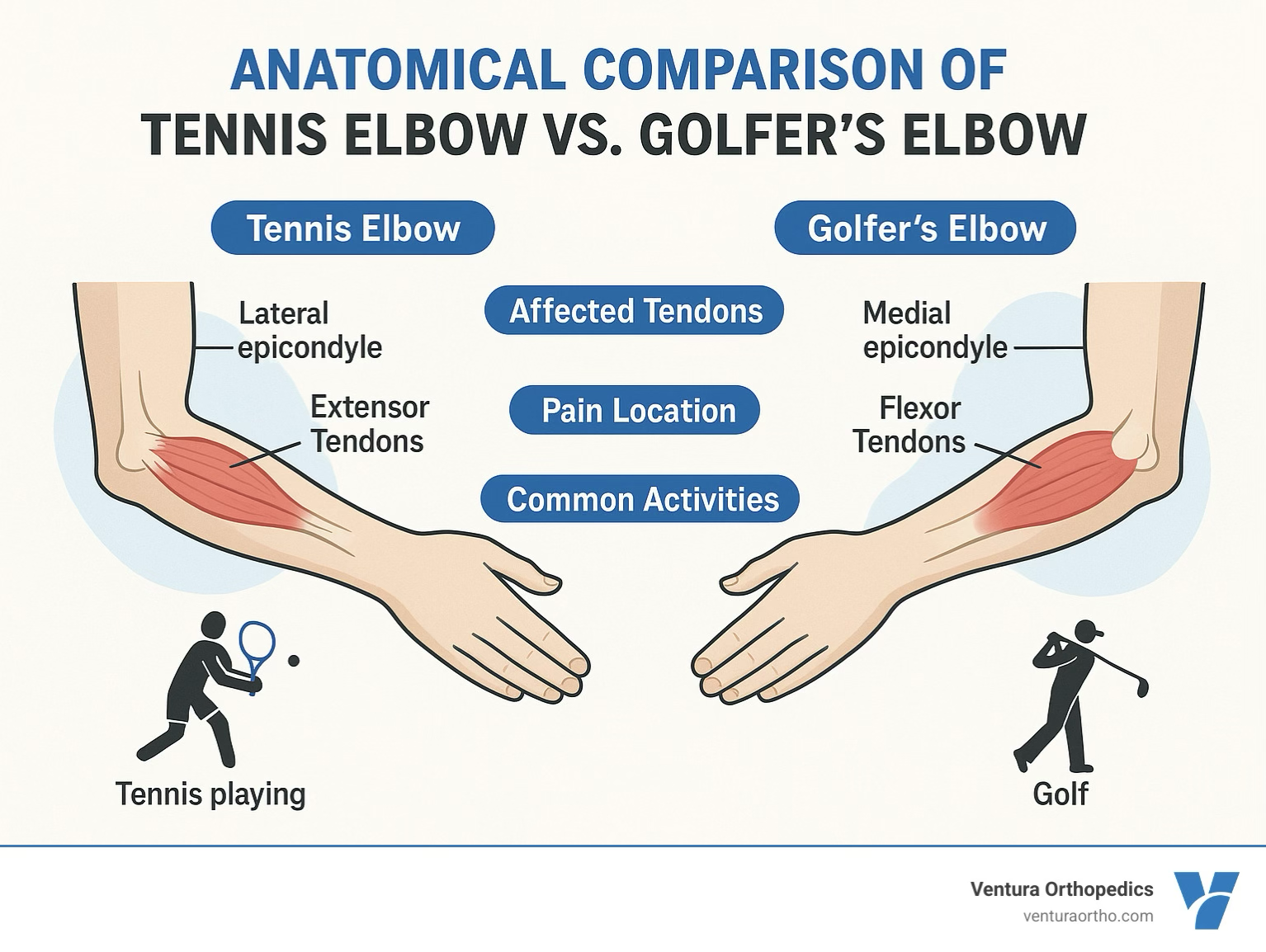
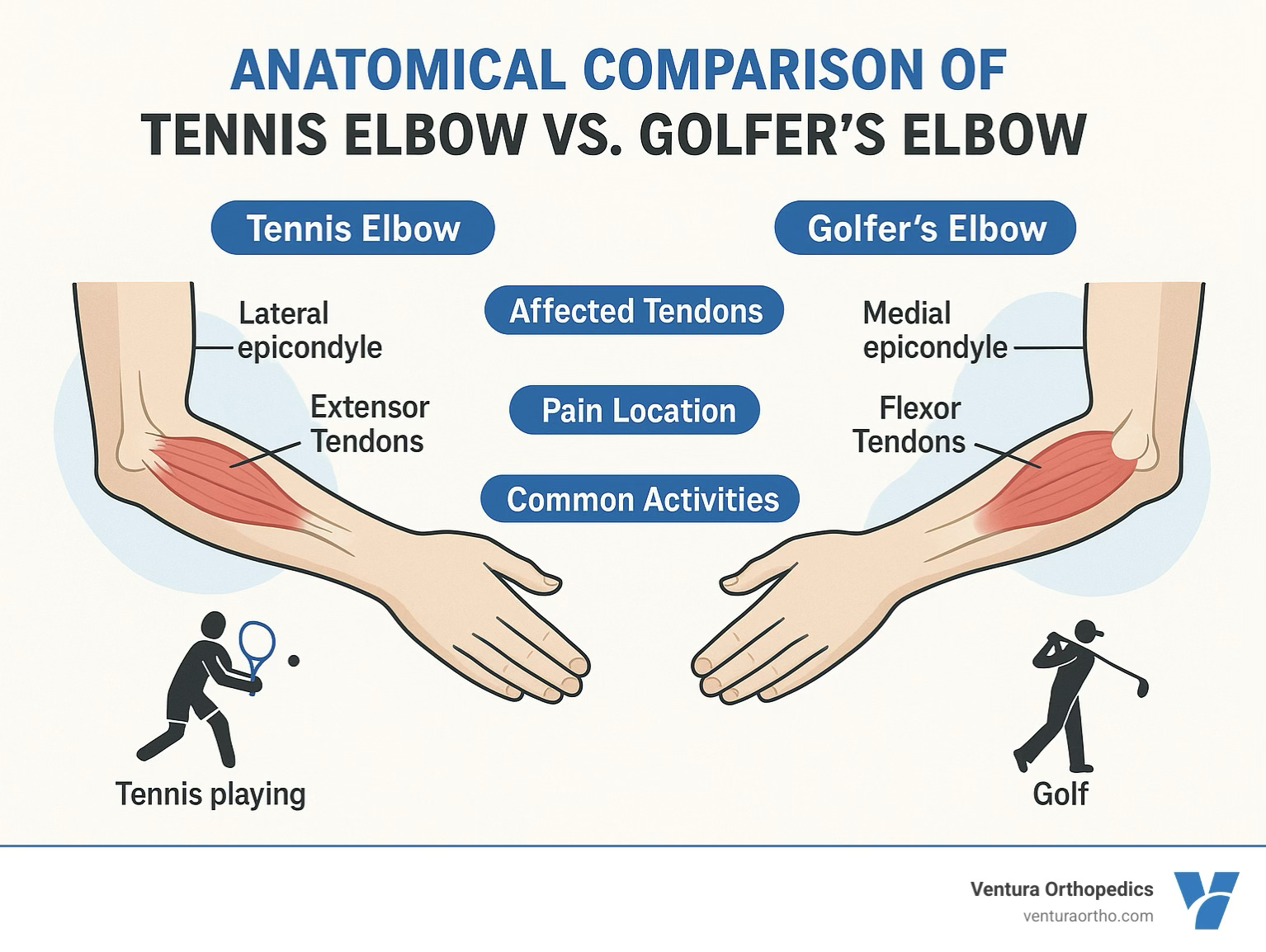
lateral & medial epicondylitis
lateral epicondylitis: tennis elbow
medial epicondylitis: golfers elbow
both are where muscle groups insert and are inflamed due to overuse
symptoms of lateral & medial epicondylitis
aching pain, possible tenderness, weakness in muscle group, pain worsening as muscle group is used, decreased ROM
treatment of lateral & medial epicondylitis
rest, NSAID’s, ice, and seeing if we can slightly change biomechanics
eventually slight stretches, slow strengthening exercises, massage and use counterforce brace
elbow dislocation
tends to occur due to a FOOSH
we usually see a posterior dislocation, but weird things can happen
can also fracture with dislocation
symptoms of elbow dislocation
deformity, pain, and swelling
treatment of elbow dislocation
check neurovascular stat
sling and ship so they can be reduced and imaged
usually will need to be in that sling for at least 3 weeks
rehab will consist of a lot of hand things until we feel they are stabilized
stay away from stretching for those weeks
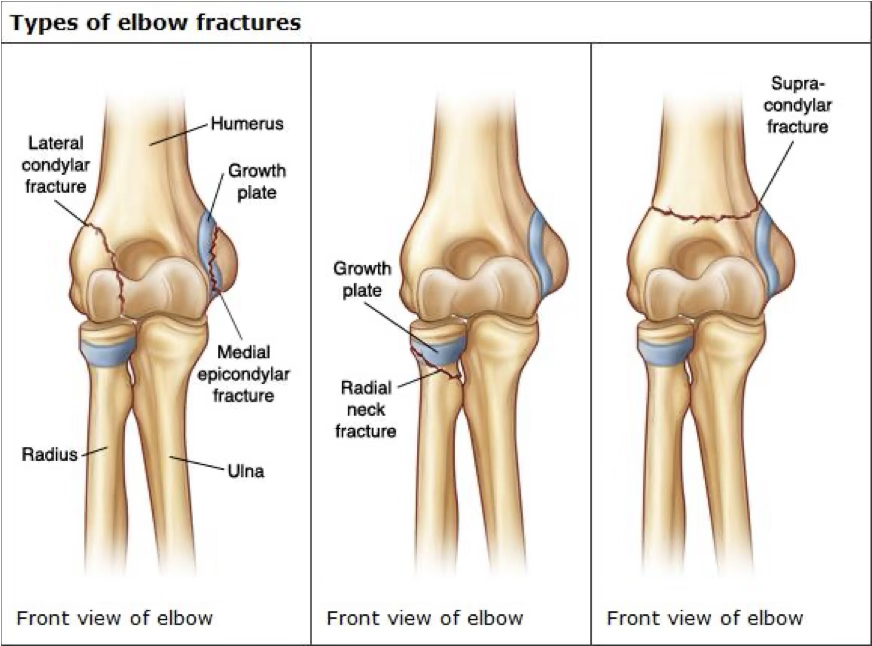
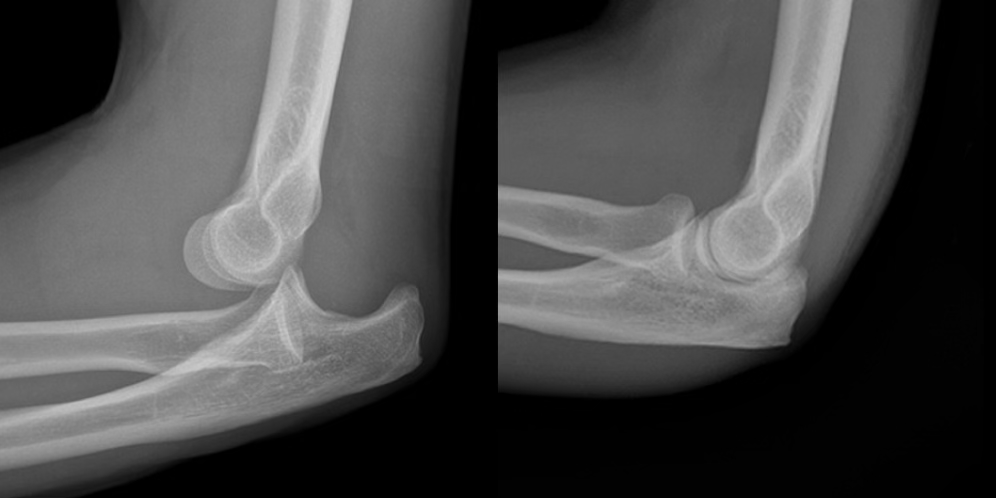
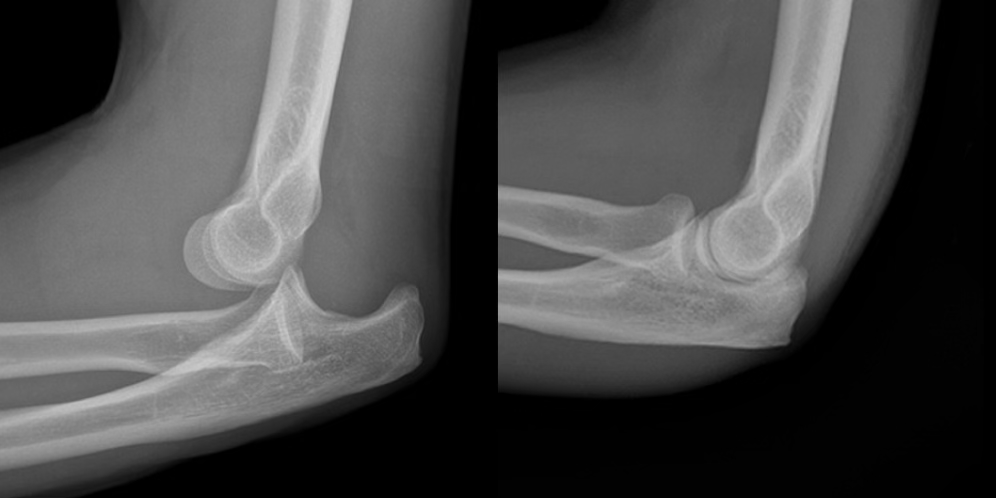
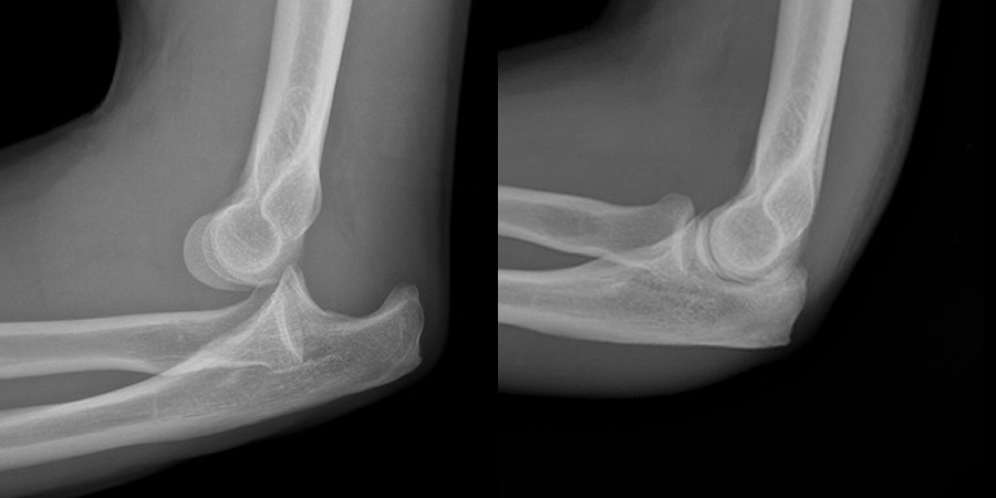
elbow fracture
FOOSH mechanism or direct hit
possible even incorrect reduction with elbow
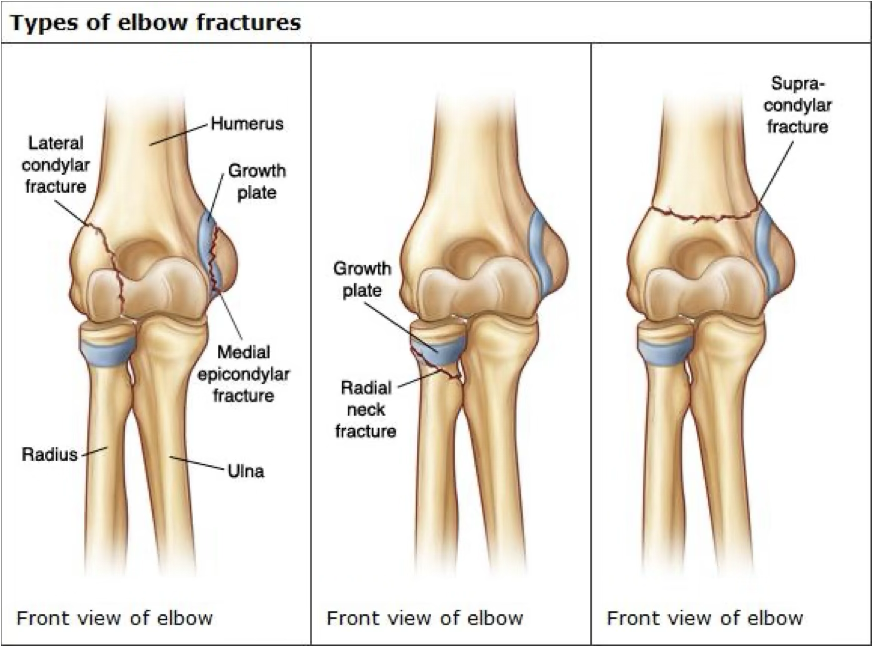
symptoms of elbow fracture
swelling, muscle spasm, pain, possible deformity, reduced ROM, compromised neurovascular
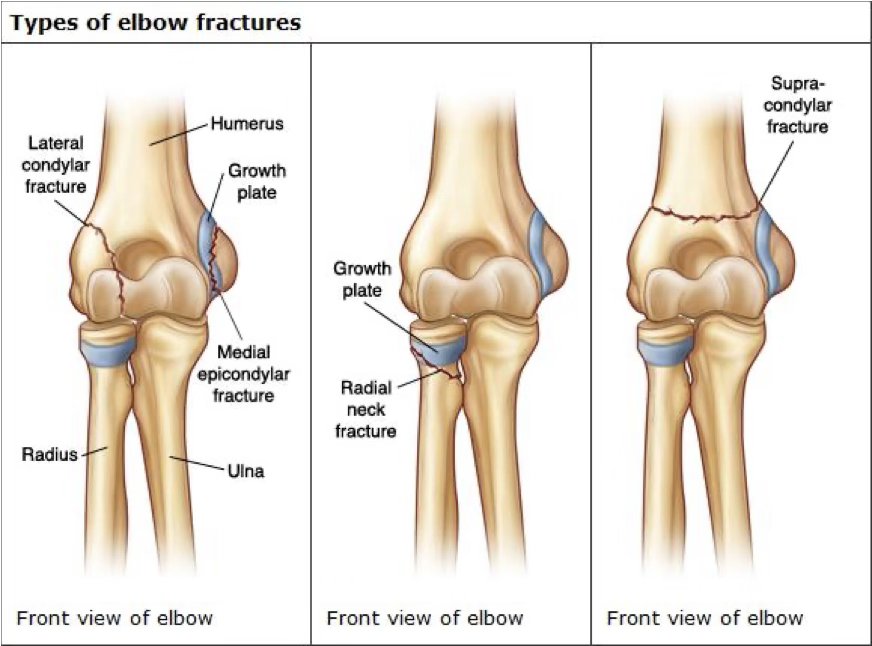
treatment of elbow fracture
stabilize and ship
may need a sling or cast or surgery
depends on cast vs. surgery

forearm fractures
FOOSH or direct blows
super common in youth due to the MOI, but rare to see it as ulanr and radial fractures simultaneously
Colles fx: radius & ulna fracture where they hyperextend (go dorsally)
smith fx: radius & ulna fracture and hyperflex (go volarly)

forearm fractures symptoms
pop, pain, swelling, possible deformity, lack of ROM

forearm fractures treatment
splint and ship, will need cast or surgery (4-8 weeks then therapy)
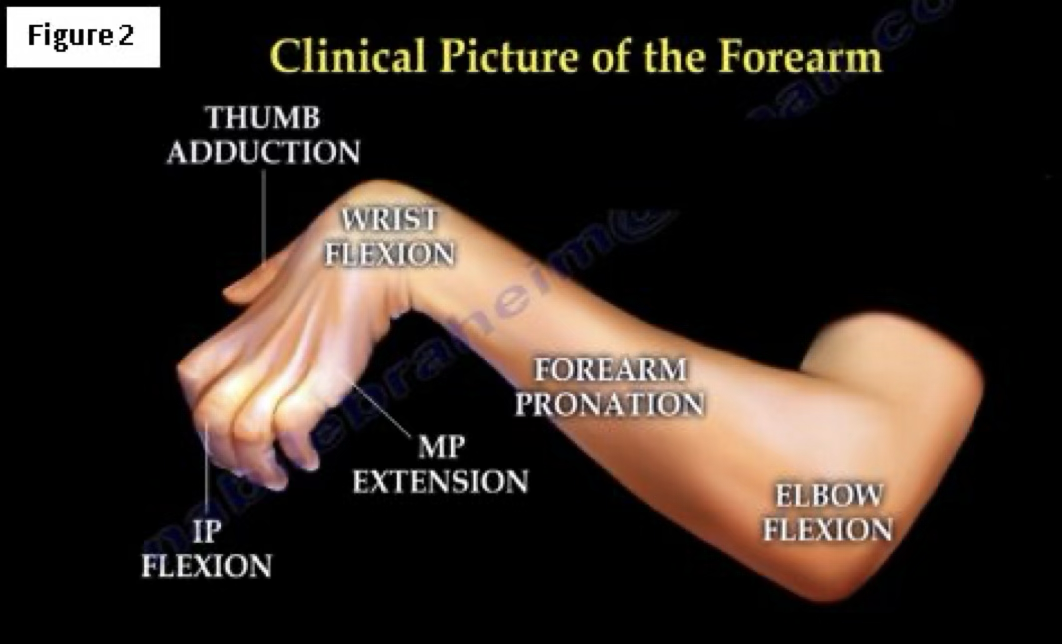
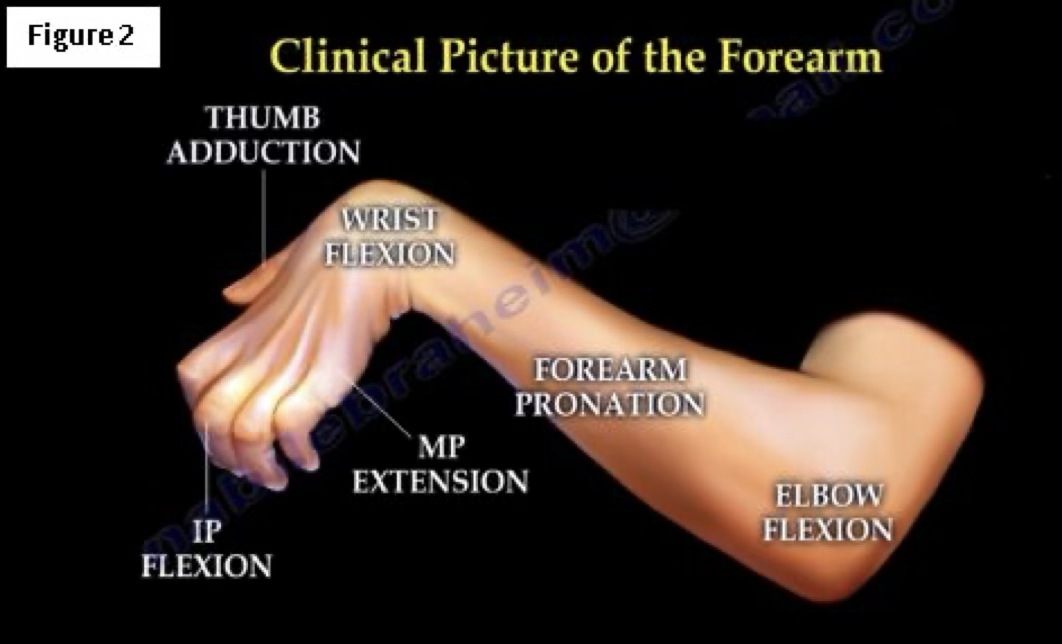
volkmann’s contracture
associated with forearm fractures which causes muscle spams, swelling, and reduced brachial artery flow
can be permament or temporary. If we can fix blood flow, should be temporary. Can still have muscle damage within hours
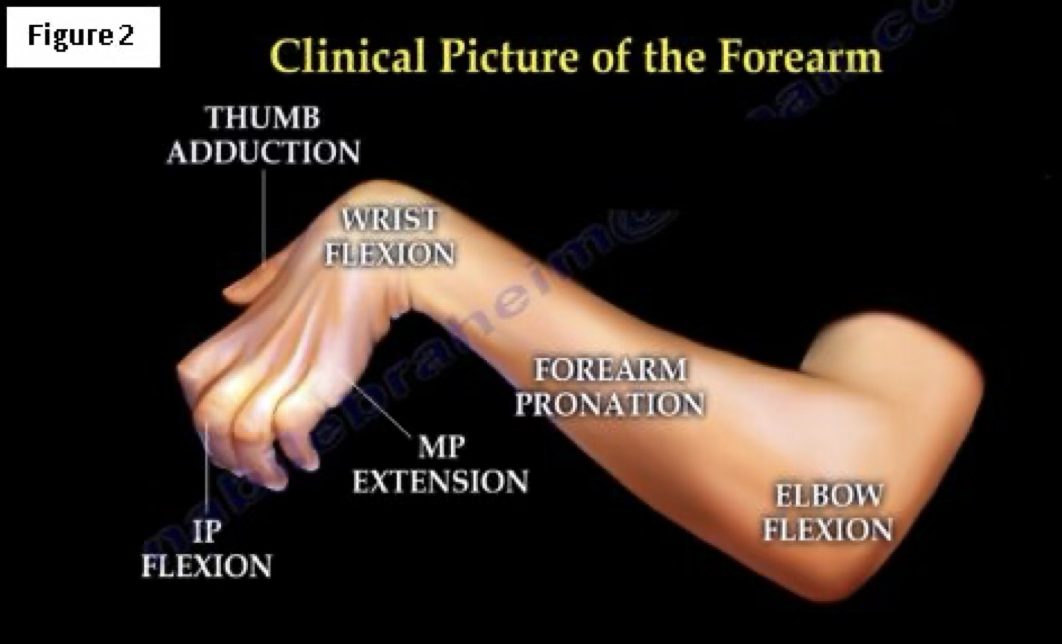
volkmann’s contracture symptoms
pain in forearm, passive extension of fingers, coldness in arm (no blood flow), decreased ROM
volkmann’s contracture treatment
if caused by a cast or wrap, take it off
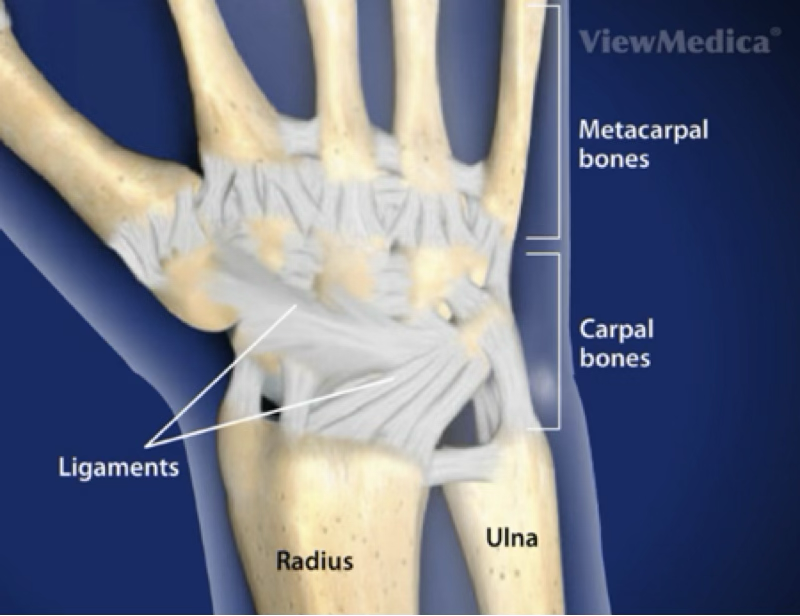
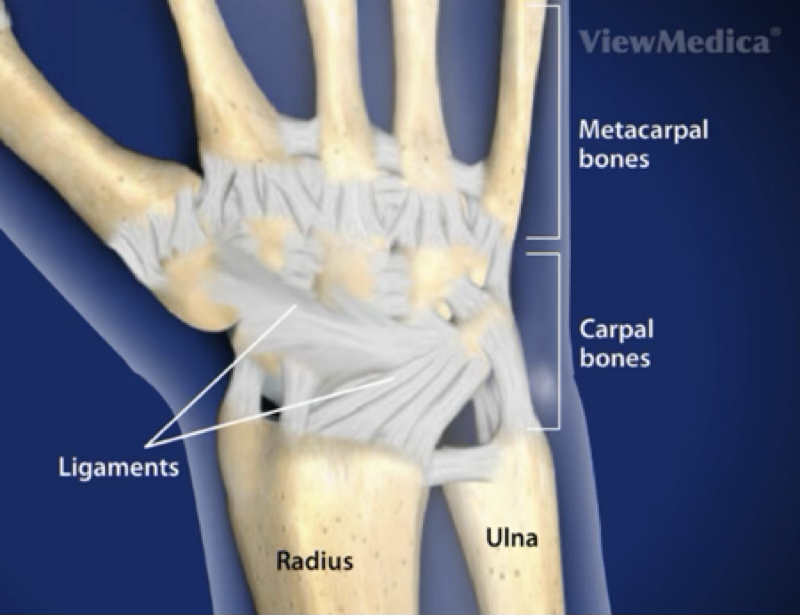
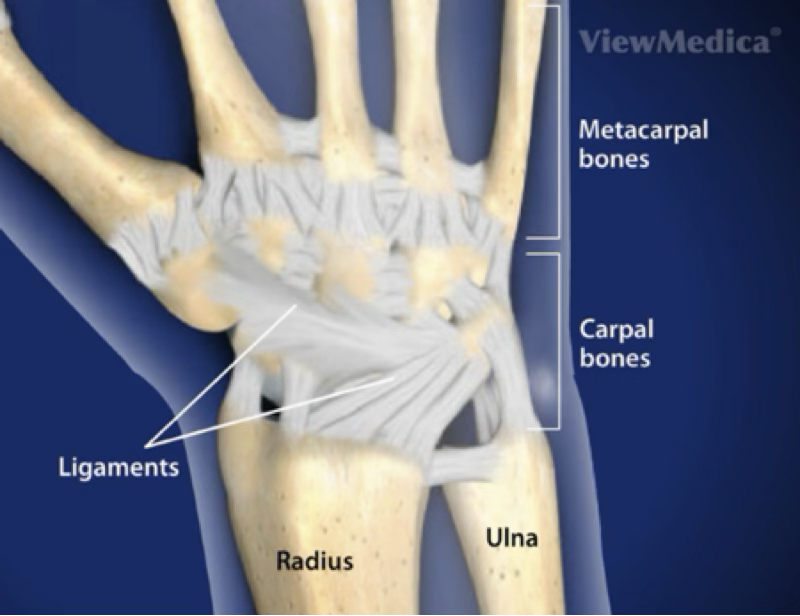
bones in the hand
8 carpals, 5 metacarpals, 2 sesamoids, 14 phalanges
MCP, MP, DIP, PIP joints
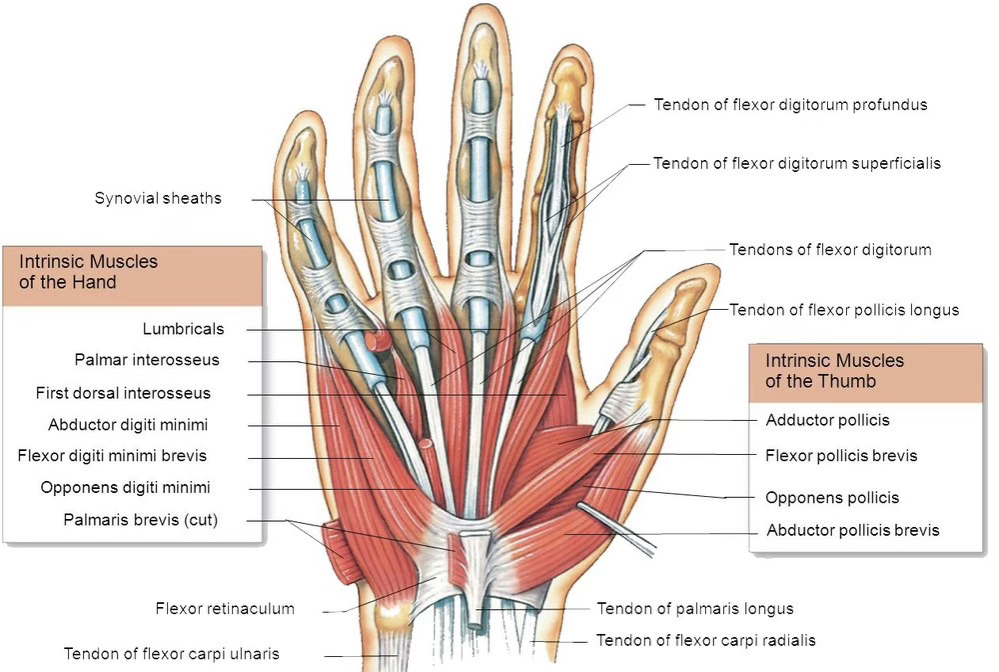
muscles of the hand
thenar: 4 thumb muscles
hypothenar: 3 pinky muscles
anatomical snuffbox: ext pollicus brevis and longus and adductor pollicus
retinaculum hold down tendons at joint areas
palmaris longus is sometimes not needed
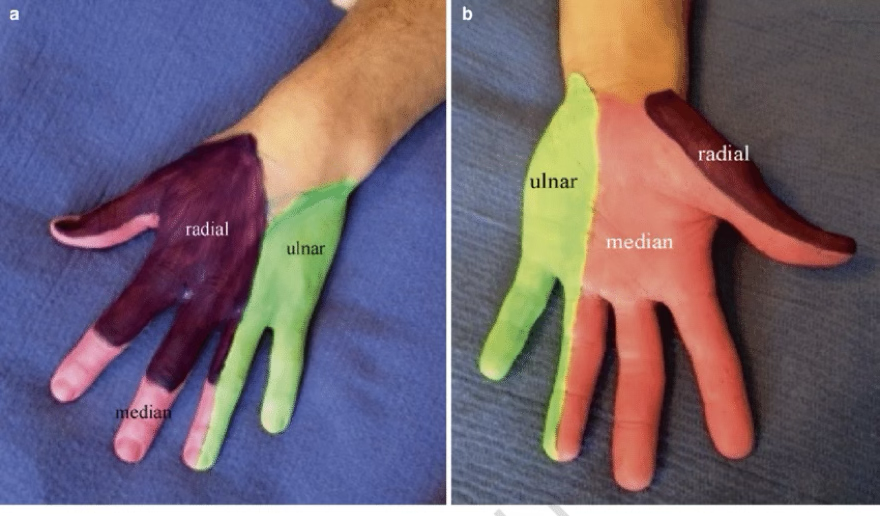
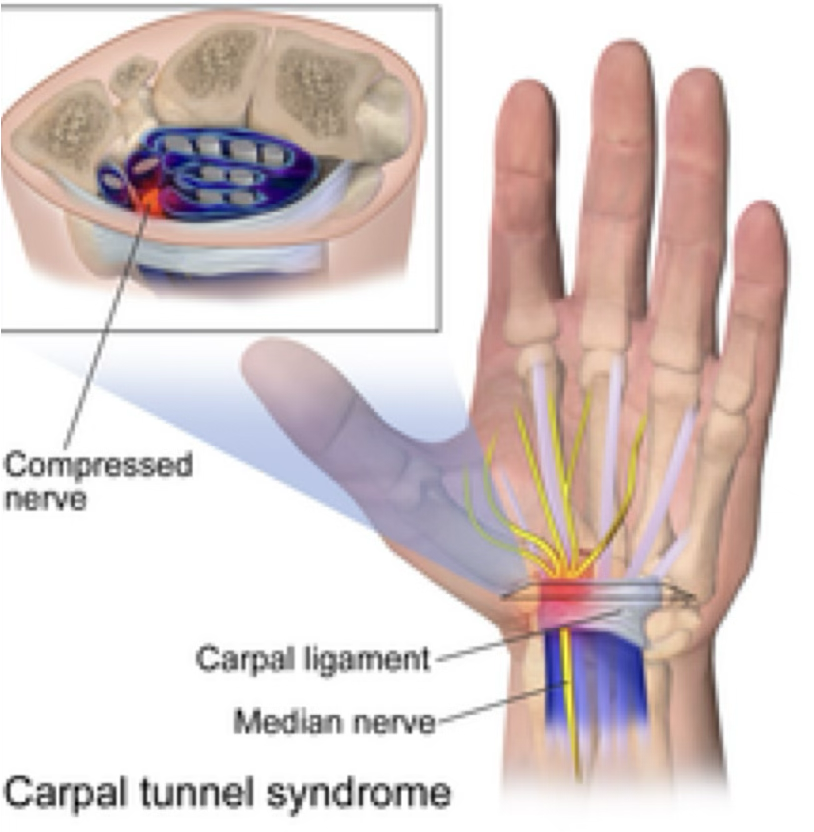
neurovascular aspects of the hand
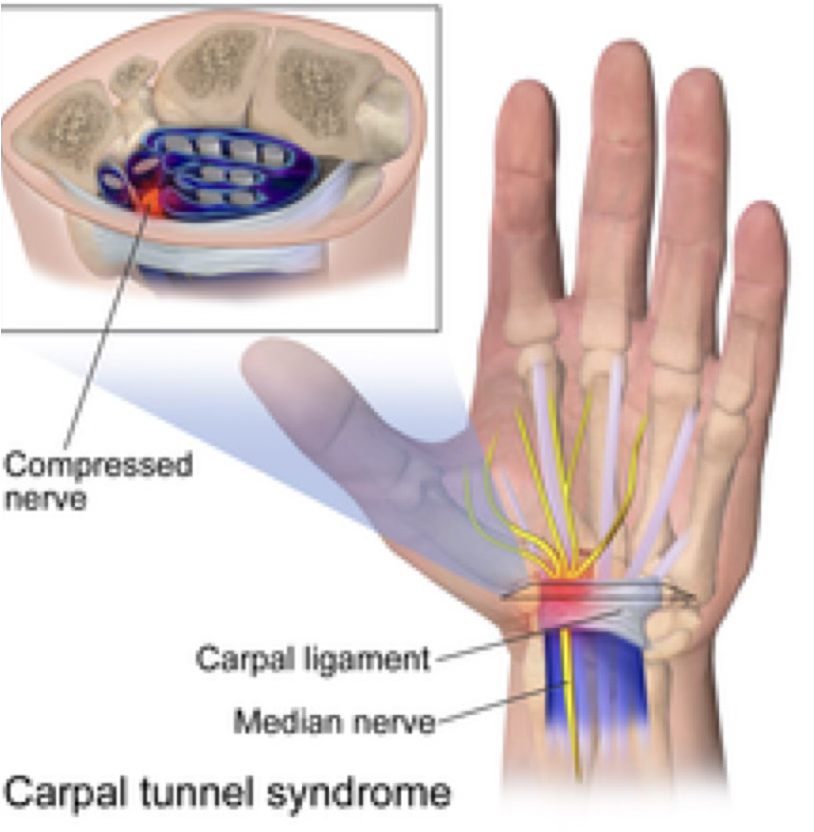
carpal tunnel: straight down wrist (dorsal side) and has median nerve
tunnel of guyon (hook or hamate is “roof”): is on ulnar side with the ulnar nerve
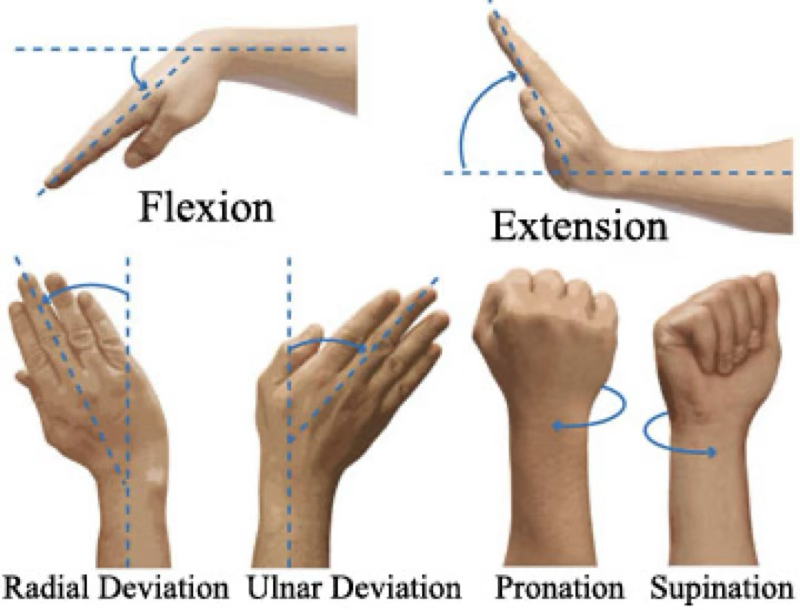
wrist and hand ROM
thumb is the only saddle joint in body, remember its motions are “abnormal” from all other joints
MCP, DIP, and PIP joints flex and extend
pinky does opposition, and fingers flex, extend, abd, adduct
wrist sprain
most common wrist injury
occurs with an abnormal, forced movement (falling on hyperext. wrist or violent flexion)
wrist sprain symptoms
pain, swelling, tenderness, difficulties with ROM
wrist sprain treatment
can send for images to rule out a fracture
can splint in brace if bad enough
treatment for pain management (meds, modalities)
can prevent or treat with wrist tape

TFCC injury
Triangular fibrocartilage complex (TFCC) is a combination of ligaments and “meniscus” cartilage on ulnar side
Gets injured when patient has a violent twist of the wrist, typically with a hyperextension

TFCC injury symptoms
pain on ulnar side, possible clicking, lack of wrist extension, swelling

TFCC injury treatment
if suspected, should send to dr for images
may need splint for about 4 weeks (rest), then start with strengthening and ROM exercises (bad case may need surgery)
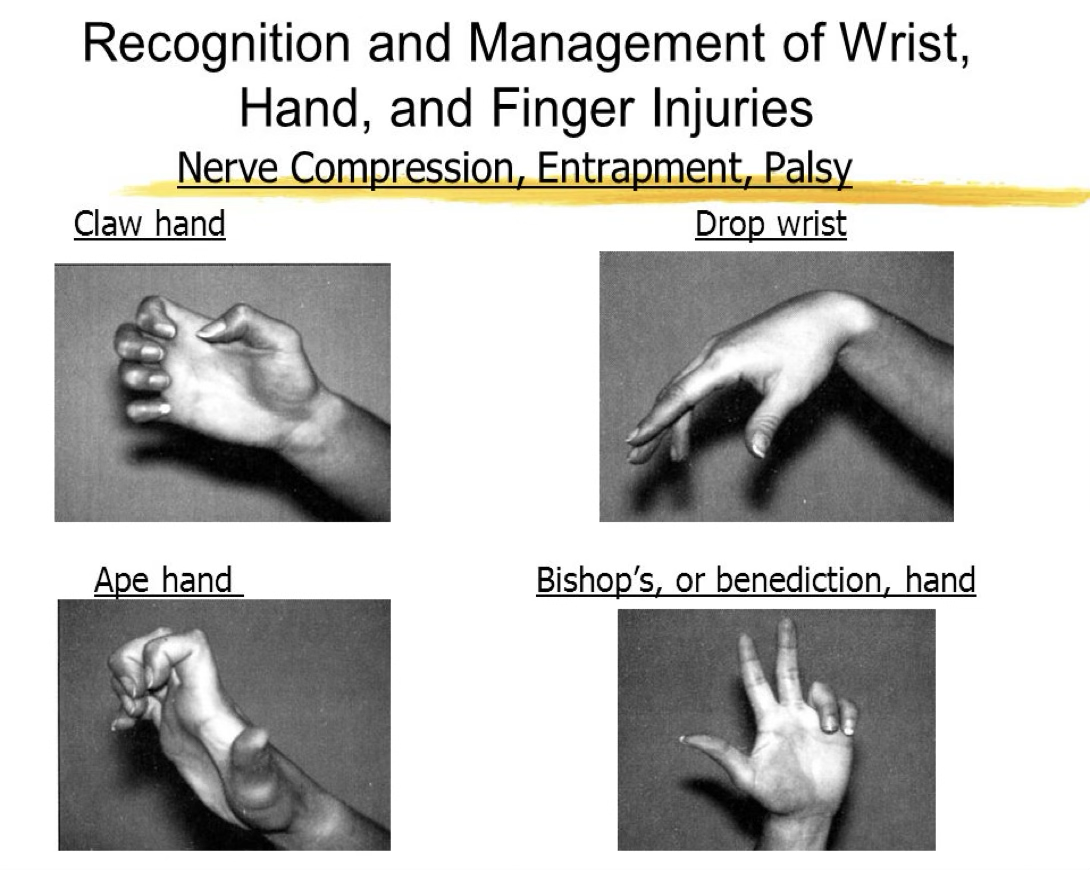
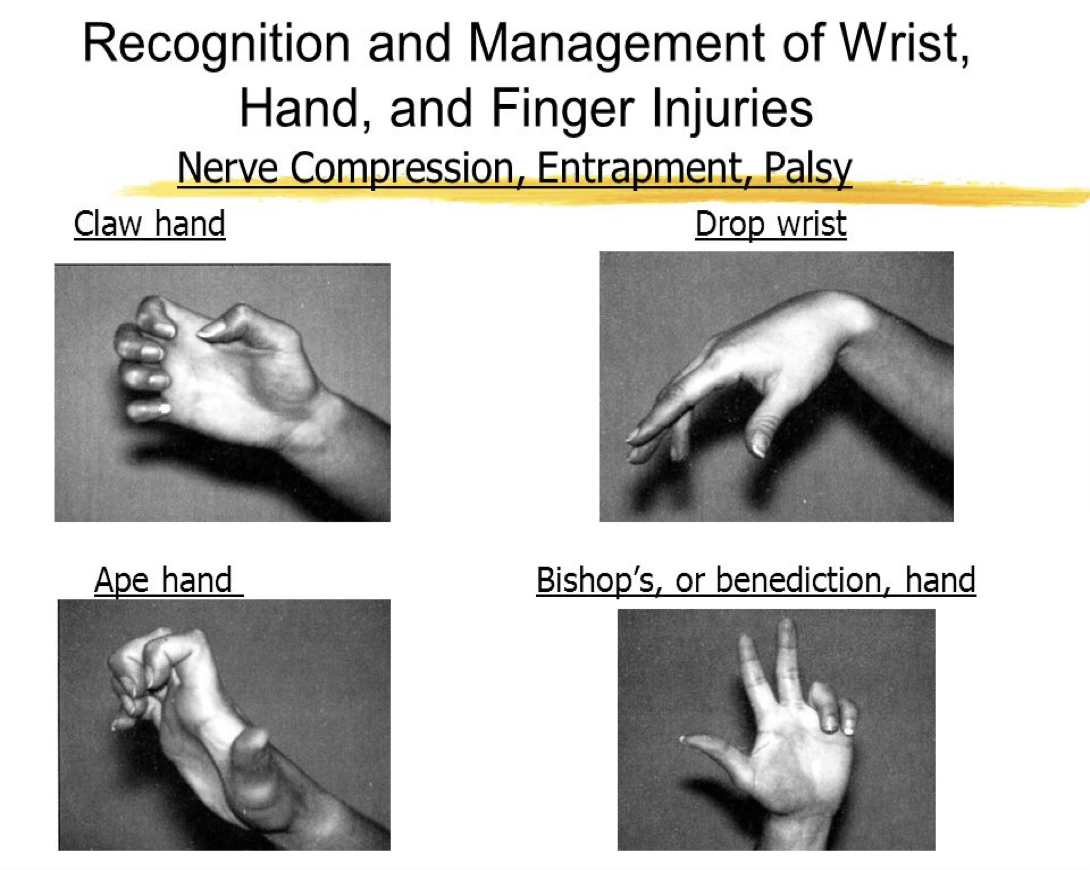
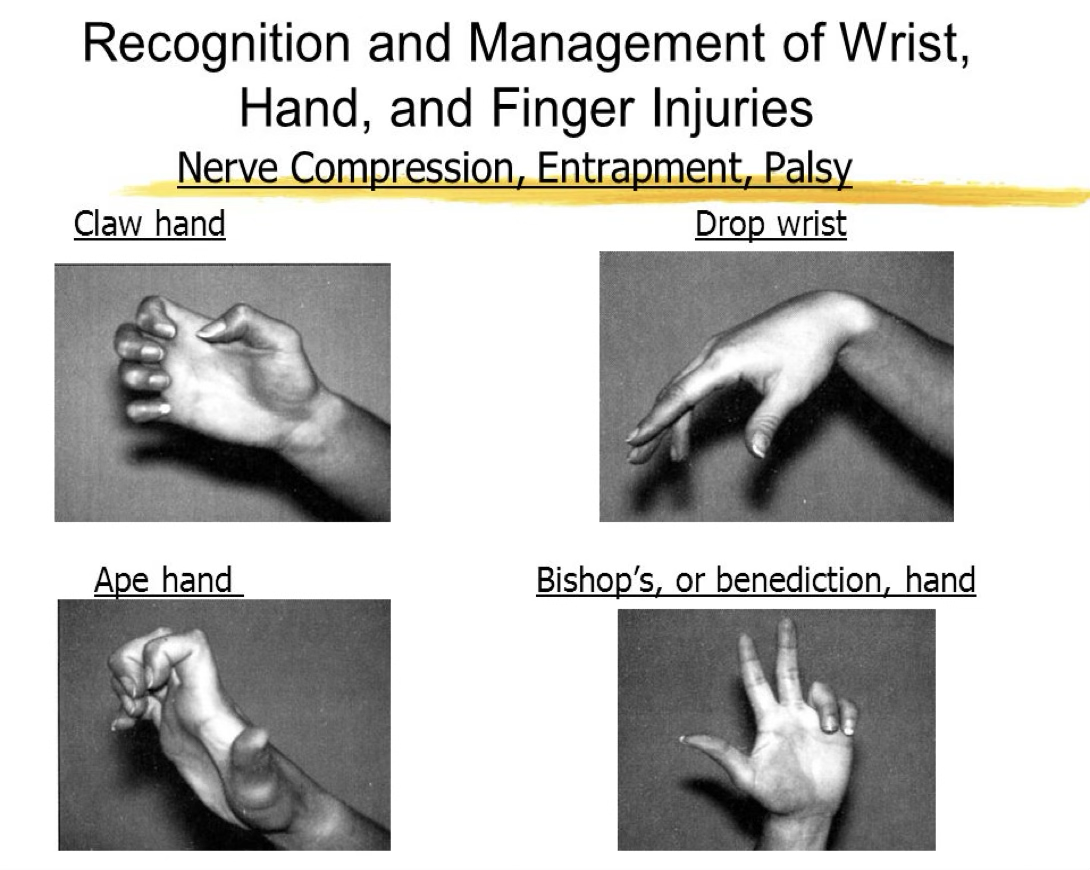
nerve compression
Bishop’s hand = median or ulnar nerve
Ape hand = median nerve
Claw hand = ulnar nerve
Drop wrist = radial nerve
direct trauma to area
nerve compression symptoms
sharp or burning pain, skin sensitivity, muscle atrophy, paralysis
nerve compression treatment
if chronic, may have irreversible damage
may need surgical decompression
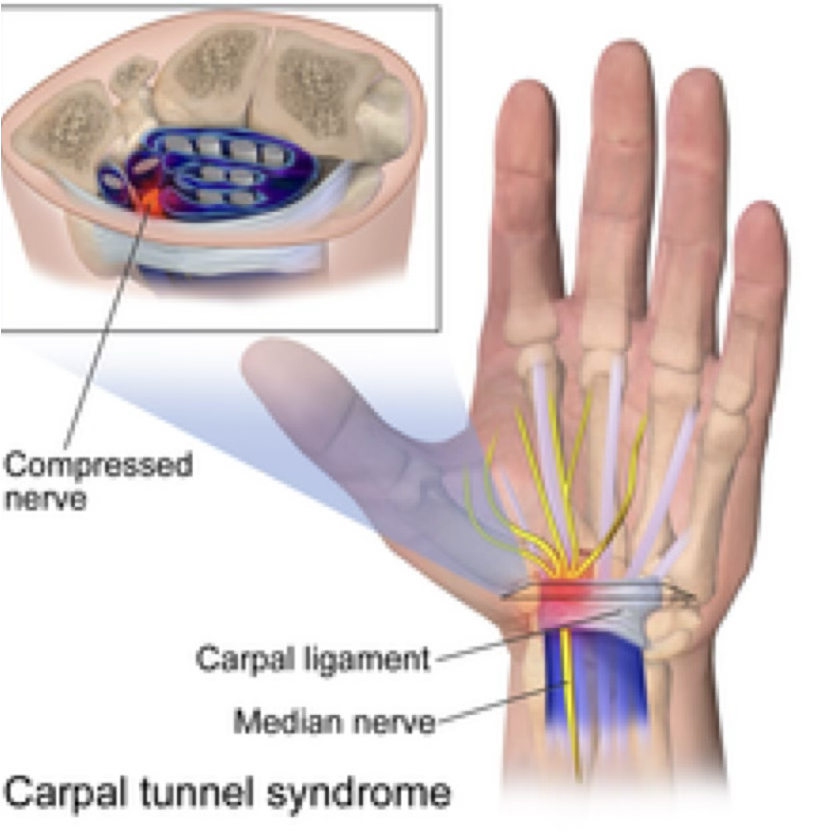
carpal tunnel syndrome
Compression of median nerve due to inflamed tendons running in this tunnel
Occurs with repeated wrist flexion or direct trauma to dorsal side of wrist
carpal tunnel syndrome symptoms
Pts tend to have sensory and motor deficits, weakness in muscles
carpal tunnel syndrome treatment
Start with conservative tx (rest, splint, meds). If it doesn’t work, try a corticosteroid injection or a surgical decompression
carpal fractures
Scaphoid fx caused by FOOSH and scaphoid gets compressed. Tends to fail due to poor blood supply
Hamate fx is FOOSH or contact where pt is holding something (think a bat)
carpal fractures symptoms + treatment
Sxs include pain, weakness, tenderness
Imaging needed. Cast or surgery. Possible padding needed

wrist ganglion cyst
tends to grow after a wrist sprain

wrist ganglion cyst symptoms + treatment
lump is present, also complains of pressure
can feel soft, hard or even rubbery
the more the pt uses the wrist, the more pain increases
Three things we can do: break down swelling then hold down with a pad, aspiration, or surgically remove. First 2 may come back. Last one, we need to get the root out or it will come back.
metacarpal fractures
due to direct axial or compressive force
metacarpal fractures symptoms + treatments
Sxs include pain, swelling, deformity, rotation of nail, loss of ROM
Can send in for imaging to see if they need to splint/buddy tape or possible cast. If rotational, will possibly need surgical repair
Bennett’s = 1st metacarpal
Boxer’s = 5th metacarpal
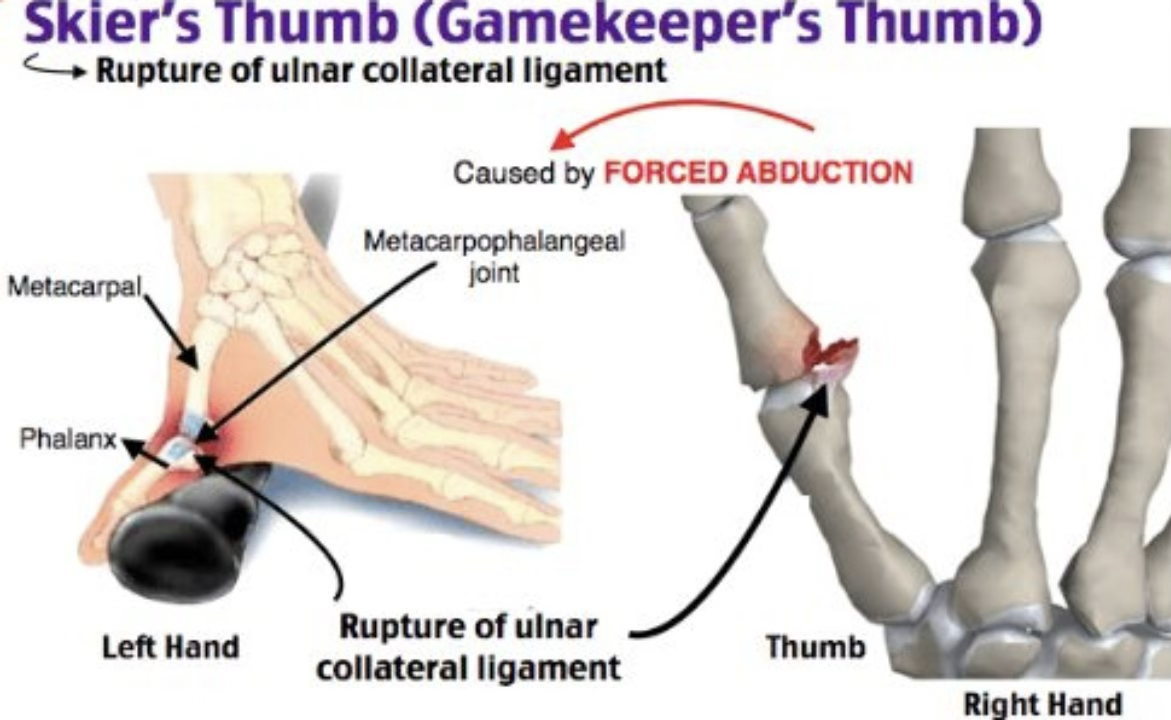
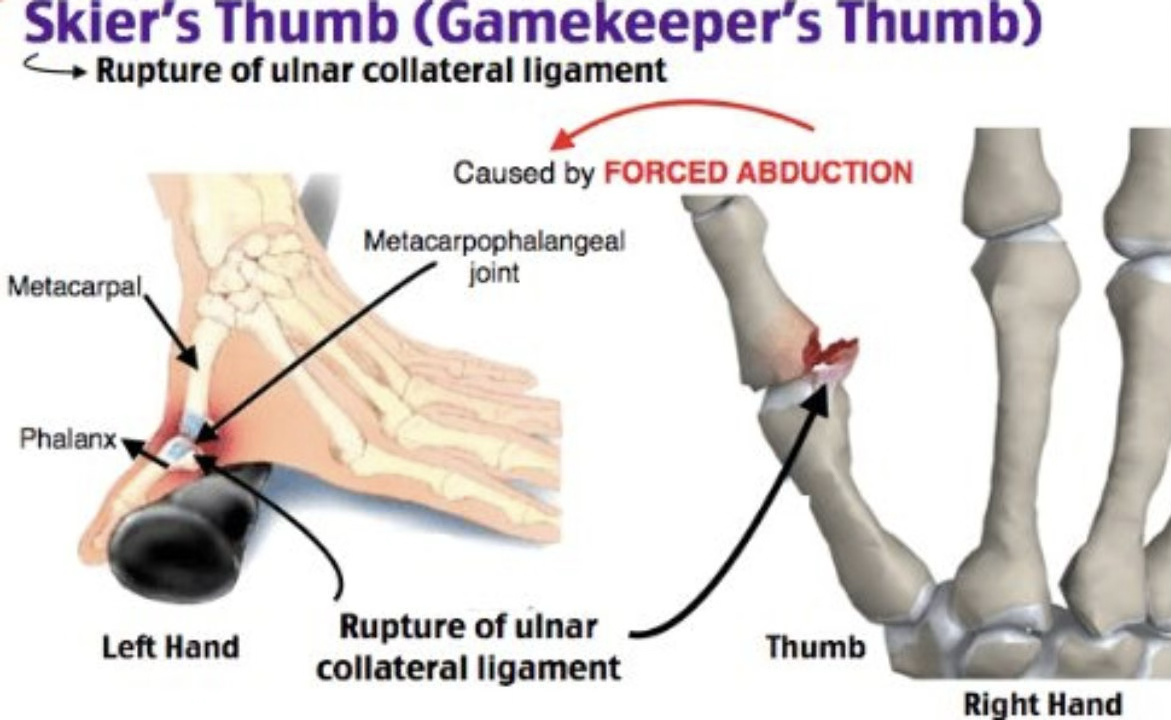
gamekeeper’s thumb
sprain of UCL of MCP jt
occurs from forceful abduction of proximal phalanx with slight hyperextension
gamekeeper’s thumb symptoms + treatment
pain in area and weak with thumb motions
imaging tells us treatment, may be able to splint 4-8 weeks in neutral position
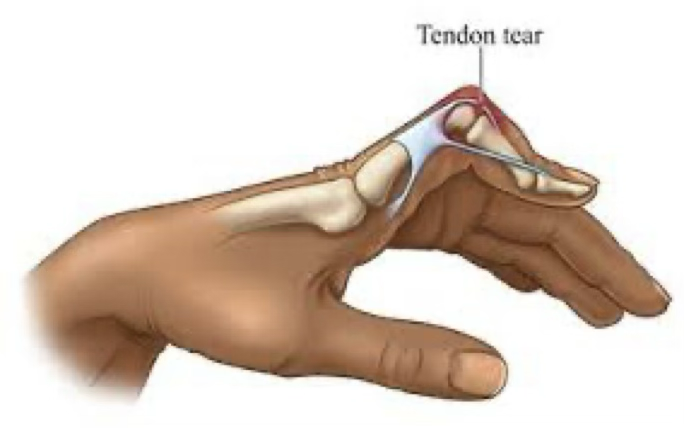
boutonniere finger deformity
rupture of extensor expansion dorsal to middle phalanx. Tendon slides below PIP and forces PIP into flexion & DIP into extension. Manage with splinting