Liver pathology study guide
1/30
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
31 Terms
Cirrhosis
a diffuse process destroys the normal architecture of the liver lobules following inflammation
most common causes are hepatitis and other viruses, and alcohol abuse
Increased risk for HCC – Hepatocellular carcinoma
Symptoms fatigue, weakness, weight loss, nausea, and itchy skin
presents with jaundice (yellow skin/eyes), severe abdominal swelling
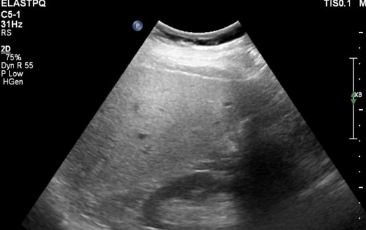
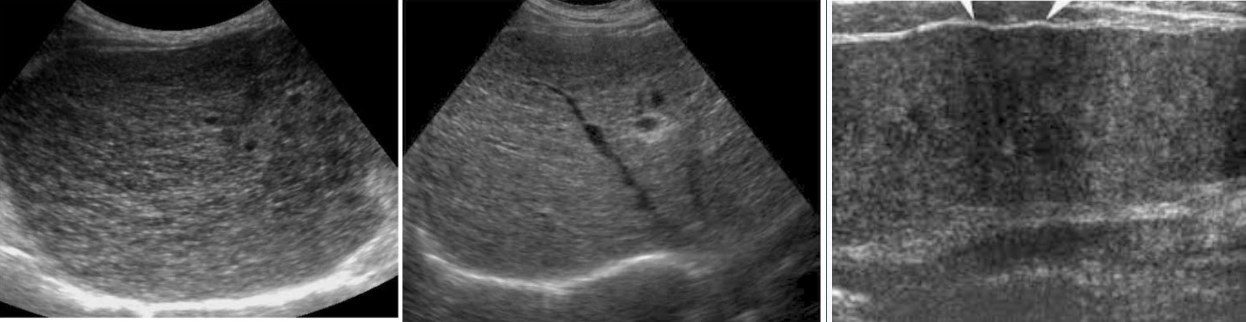
Fatty Infiltration
Steatosis; also known as fatty liver
Alcohol and obesity are the leading cause
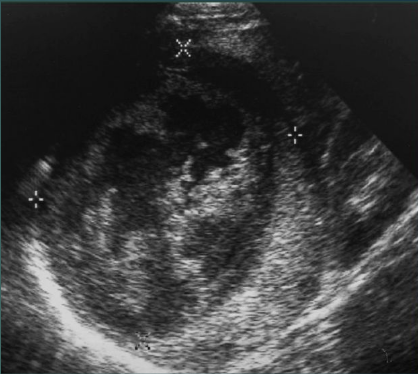
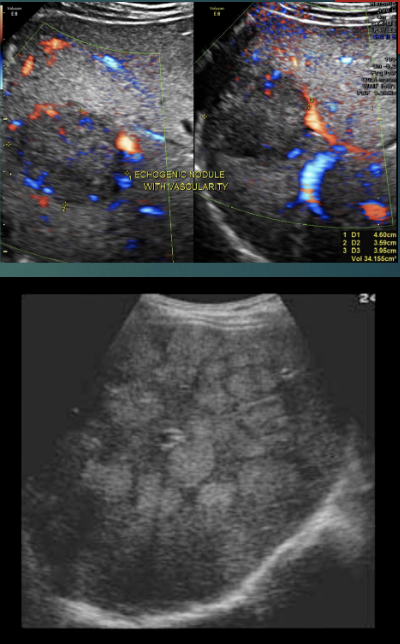
Primary Malignant Tumors
Hepatocellular carcinomas (HCC) AKA Hepatoma
80% to 90% of the primary malignant liver tumors
Cholangiocarcinoma
Second most common primary malignant tumor
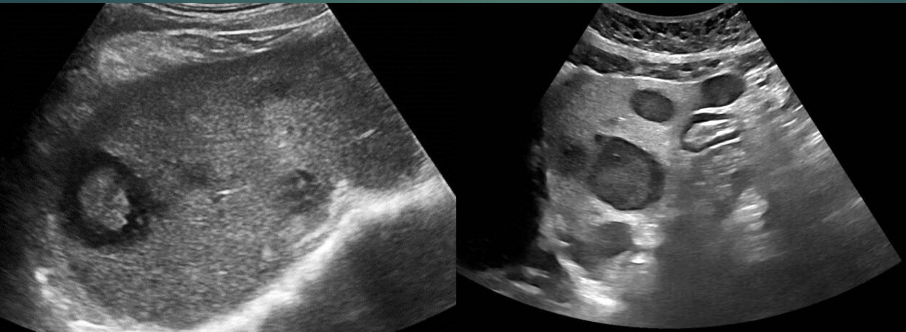
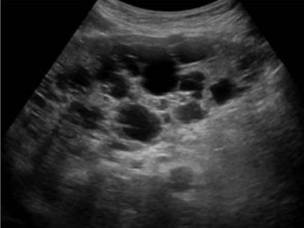
Hepatic Cysts
Congenital cysts: True hepatic cysts

Isolated polycystic liver disease (PLD)
cysts are only in liver, Caused by inherited developmental defect in formation of bile ducts
Acquired Cysts - hematoma
Bleeding within simple cyst, hematocrit levels drop, Repeated episodes of bleeding may result in calcification within the cyst
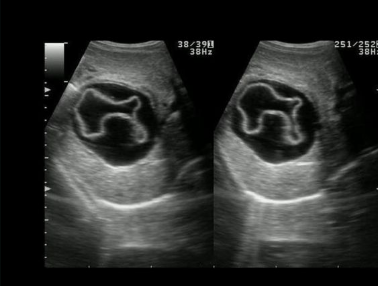
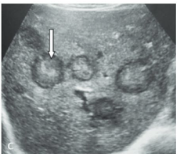
Acquired Cysts Echinococcal Cyst - Hydatid Diseases
Most common caused by Taenia echinococcus or Echinococcus granulosus—parasitic tapeworm
Elevated LFT’s
demonstrate increased levels of ALP, AST, ALT
Glycogen storage disease
Liver Cell Adenoma: Benign
Hepatomegaly
More often solid liver masses (adenomas)
Type 2 and 3 are associated with cirrhosis and HCC
Adenomas. Can occur in up to 40% of patients with type 1 von Gierke disease.
Liver cell adenoma
❖ Association with long-term oral contraceptive use in
women is well documented.
❖ Liver cell adenomas are significantly more common in
women, with a reported female-to-male ratio of 4:1
Elevated AFP
in your blood—greater than 400 ng/mL—could be a sign of liver tumors.
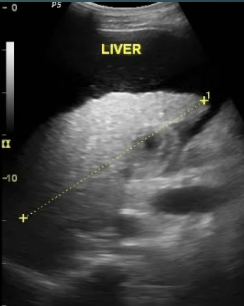
HEPATOMEGALY
Most ultrasound references state that a liver greater than 15.5 to 16 cm in size is considered enlarged
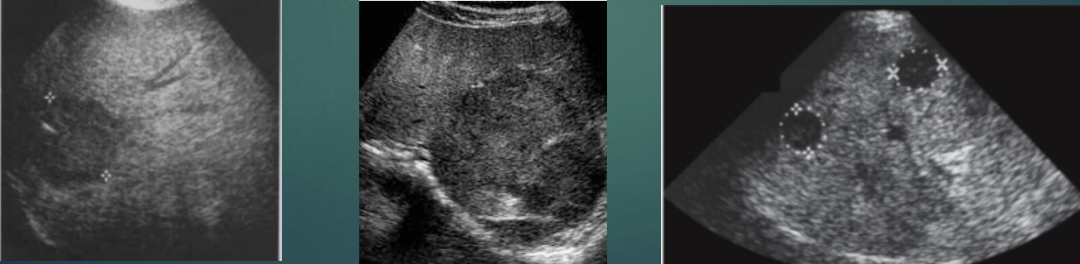
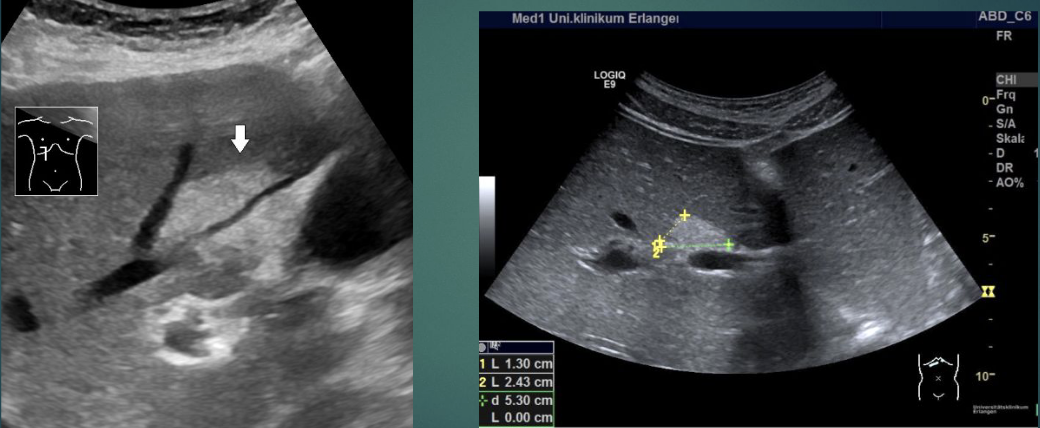
Metastatic masses
liver tumors incidence: 8 to 20 times more common than HCC, liver disease are: Gallbladder, colon, stomach, pancreas, kidney, ovaries, breast, and lung.
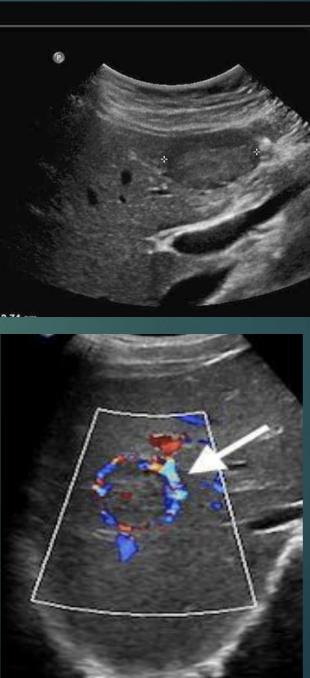
Increased vascularity
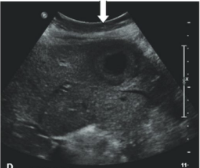
Lung metastases
Hyperechoic lesion (white bold arrow) with peripheral halo-target sign-highly specific for metastases-lung cancer
TIPS (Transjugular Intrahepatic Portosystemic Shunt)
performed to treat severe complications of portal hypertension, typically caused by cirrhosis or liver scarring. It creates a shunt to lower high blood pressure in the liver's veins, managing refractory ascites, bleeding esophageal varices, and hepato-renal issues
normal velocity: 90-190 cm/s
Common collaterals or varices of cirrhosis include
• Recanalization of the paraumbilical vein
(ligamentum teres)
• Esophageal varices
• Splenic varices
• Splenorenal shunt
Secondary findings of cirrhosis should be documented and can include:
• Portal hypertension
• Splenomegaly
• Varices
• Collaterals
• Ascites
Cavernous Hemangioma
The most common benign solid lesions of the liver
Most measure <3 cm but larger lesions are possible
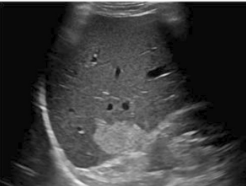
Autosomal dominant polycystic kidney disease
represents 80% to 90% of all PLD and cysts are present in both the liver and the kidney
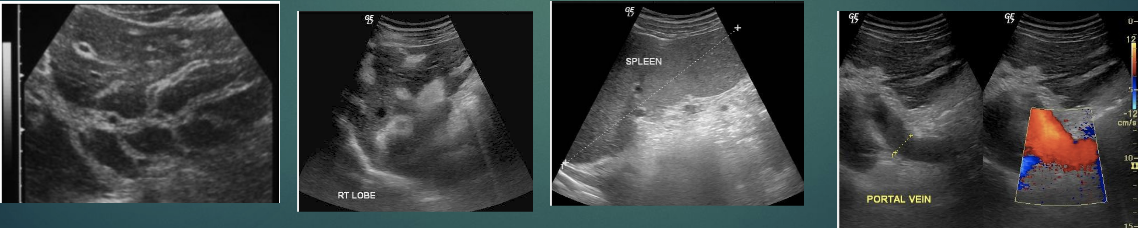
Schistosomiasis
Caused by a parasitic tapeworm, sometimes described as a turtle shell appearance
Splenomegaly with portal vein and splenic vein dilatation
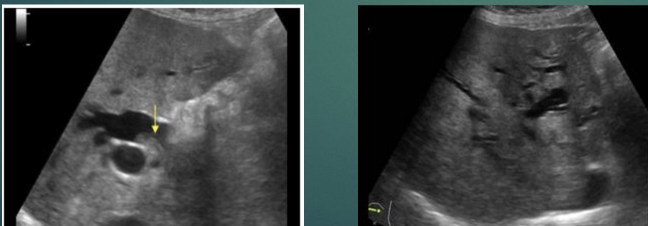
Focal fatty sparing
Porta hepatis classic location

Diffuse fatty infiltration
Focal fatty infiltration
Coronary vein
the most commonly involved portal systemic collateral pathway in liver cirrhosis, seen in roughly 80% of cases.
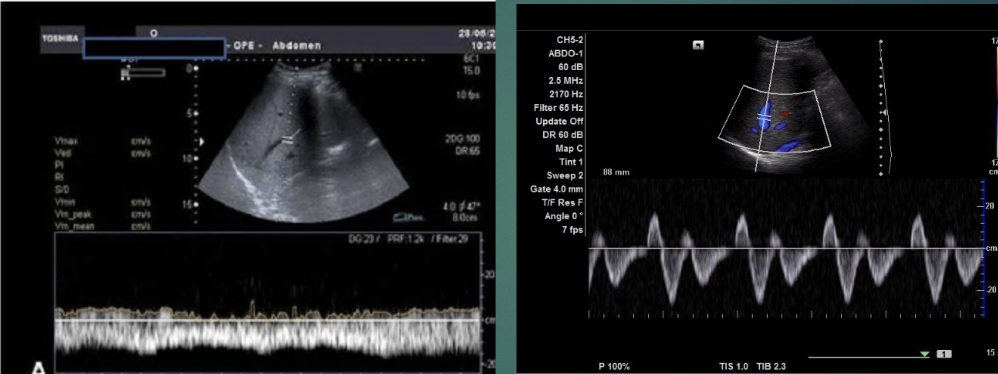
Cirrhosis PW
the hepatic vein waveform commonly becomes monophasic (flat or blunted) in patients with cirrhosis, departing from the normal triphasic pattern
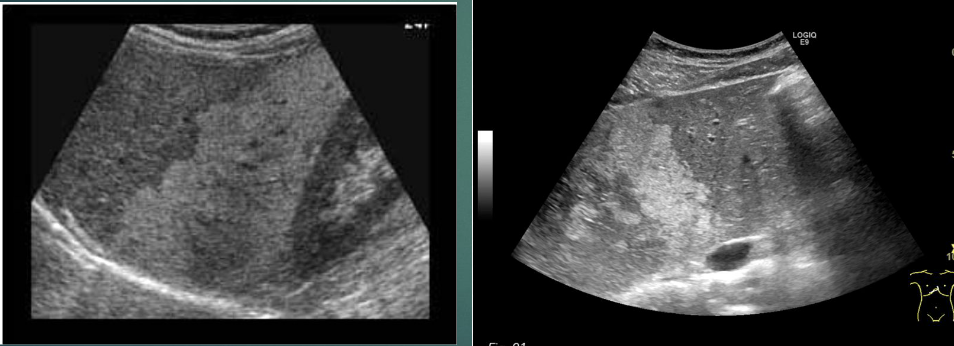
Hepatic Kaposi sarcoma
the most common hepatic neoplasm in patients with AIDS, reported in 34% of cases in an autopsy series. Hepatic KS is typically asymptomatic and rarely diagnosed in life
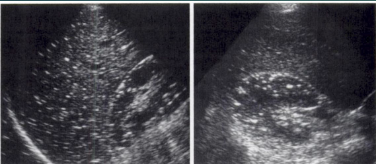
“starry sky” pattern
Budd chiari
Clinical: pain, jaundice, ascites, hepato/splenomegaly

Hepatic Artery Evaluation:
The primary goal is to exclude hepatic artery thrombosis (HAT) or stenosis, often evaluating the resistive index (RI). An RI less than 0.5–0.6, or a slow systolic upstroke (tardus-parvus), suggests possible complications.
Portal Vein (PV) & Hepatic Vein (HV) Monitoring:
Sonographers check for portal vein thrombosis (PVT) or stenosis, ensuring normal hepatopetal flow. They also verify HV patency to rule out outflow obstruction.
Bull’s eye target lesion