Interpretation and Application of Common Lab Work
1/42
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
43 Terms
Purpose of Lab Tests
screening
diagnosis
monitoring
modification of therapy program according to laboratory findings
screening
used to screen for occult disease
diagnosis
used as a supplement to physical signs/symptoms, thus aiding diagnosis
monitoring
used to follow the course of a disease or conditions; look at trends
Parkinson’s Disease
a neurodegenerative disease characterized by a loss of dopaminergic neuron function resulting in bradykinesia, rigidity, tremors, & postural instability
MS Changes
CT Scan head: no acute abnormality
medications unchanged
complete blood count (CBC): WBCs 12K, N 79%)
urinalysis (UA): 20-30 WBCs, nitrite + LE + (leukocyte esterase), many bacteria; C/S pending
basic metabolic panel (BMP): normal
Dx?
Complete Blood Count (CBC)
Common Indications:
infections - look at WBC(white blood cells) & individual sub-types of white cells
bleeding, bruising, petechiae - look at hemoglobin (Hgb), platelets
Trends: more important than one point in time
is the white blood cell count or hemoglobin trending up or down over the clinical course?
take into context the past medical hx or surgical history
is there a history of cancer, recent surgery, medication (blood thinners, steroids, chemo), cardiac, or pulmonary problems
CBC Format
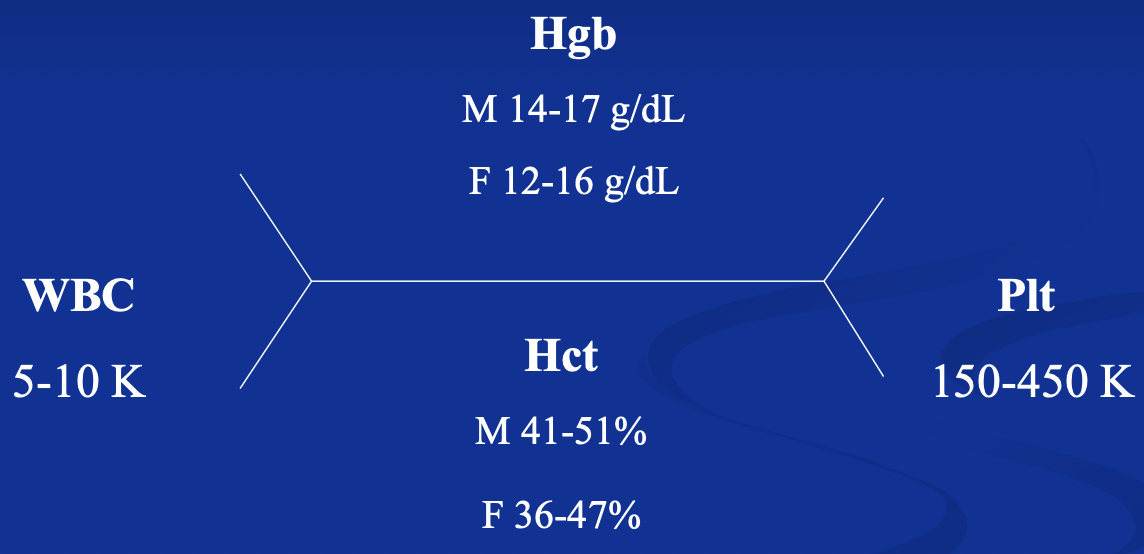
Hemoglobin (Hgb)
iron metalloprotein in RBCs responsible for binding oxygen; 1RBC has approx 280K Hgb molecules
measures the amount of Hgb in the body
low Hgb = anemia
high Hgb = polycythemia
Normal female: 12-16g/dL Normal male: 14-17g/dL
critical cut-off level is <8g/dL
case by case basis
essential ADLs may be permitted (as per Acute Care section-APTA)
pulse oximeter
pulse oximeter
reflects % O2 saturation; not necessarily a reflection of Hgb levels
Hematocrit (Hct)
proportion of blood volume that is occupied by RBCs; assists in evaluating hydration status, anemia or polycythemia
norma female: 36-47% Normal male: 41-51%
increased in polycythemia, high altitudes, heavy smoking, chronic lung disease, congenital heart defects
decreased in anemia and hemodiltion
critical cut-off level is <25%
case by case basis
may participate in essential ADLs with assistance

Red Blood Cells
Low levels = anemia (different types)
acute blood loss-normocytic (normal size)
slow blood loss (Fe deficiency) or chronic disease-microcytic (small)
Vitamin B12 or folate deficiency-macrocytic (big)
High levels = polycythemia
polycythemia vera
secondary polycythemia
vigorous exercise
high altitude
smoking
MCV (mean corpuscular volume) - Size of RBC; helpful in determining anemia type
Platelets
tiny cellular fragments that form clots; stop or prevent bleeding
normal value is 150,000-350,000/uL
thrombocytopenia (low levels) lead to poor clotting; easily bruised or bleeds
thrombocytosis (high levels) occur during infection inflammatory processes, neoplasm
Acute Care Section APTA Guidelines:
<10,000 &/or temp >100.5 = bed rest
10,000-20,000 = therapeutic exercise/bike (no resist)
>20,000 = therapeutic exercise/bike
WBC Types
indicates the functional status of the immune system
neutrophils 60-70% increased in infection
Eosinophils 1-4% remember NAACP
Basophils 0.5-1% leukemias, certain drugs
lymphocytes 20-40% increased in viral infections inflammation
monocytes 4-8% increased in viral, bacterial and/or parasitic infection
WBC - Neutrophils
normal values 60-70%
primary infection fighters; first line of defense
left shift (proliferation of immature cells from the bone marrow-normal response)
acute infection or inflammation
certain medications
right shift (proliferation of mature cells)
WBC-Lymphocytes
normal 20-40%
often increased in chronic inflammation
important cells that determine the “type” of response the immune system mounts
natural killer T cells attack body cells that have become cancerous or taken over by viruses
B cells make antibodies that attack bacterial cells and toxins
WBC - Eosinophils
normal 1-4%
elevated in hay fever, asthma, dermatomyositis, parasitic infections, neoplasm
remember → NAACP
Neoplasms
Addison’s Disease (disease of the adrenal gland)
Urinalysis
for suspected renal disease, urinary tract infection (UTI), diabetes (DM), cancer
Protein: normally very little
pH: normally 6-7 (1-3 acidic = gout)
Glucose: normally none in urine, if detected indicates DM, gestational diabetes, pancreatic or other endocrine disorders
WBC: normal is <10/hpf; indicates inflammation or infection
Nitrite: E.Coli makes an enzyme that ionizes normal urine nitrates to nitrites
Leukocyte esterase (LE): enzyme released by WBC in the urine; indicator of infection
a urine culture is the gold standard for diagnosis of a UTI
Diagnosis
urinary tract infection - treated with antibiotics
implications for physical therapy - resume rehab after mental status returns to baseline for this patient; may still be on antibiotics, but should not be febrile
Complete or Basic Metabolic Panel (CMP or BMP)
Indications:
electrolytes (Na+, K+, CO2, Cl-)
renal function (BUN, Cr)
liver function (ALT, AST)
Protein levels (albumin)
Glucose
Na+
sodium
normal values between 135-145 mEq/L
hypernatremia can result in confusion and/or lethargy
hyponatremia can result in muscle cramps, confusion, lethargy, and/or nausea
K+
potassium
normal value between 3-5-5.0 mEq/L
hyper/hypokalemia or abnormally high/low levels increase risk of cardiac arrhythmia
review medications, check renal function
PT contraindicated when 3.4>K+>5.1
Serum CO2
bicardbonate
normal value between 22-27 mEq/L
abnormal levels indicate renal or pulmonary problems
PT contraindicated when 10>CO2>40
Serum Glucose
normal value between 70-130 mg/dL
concern in diabetics — low/high levels can lead to mental status changes, seizures, fatigue, headache
guidelines will vary from facility to facility
consider the patient’s “trend”; treat the patient-not the paper!
PT contraindicated when 60>glucose>300
Hemoglobin A1c (Let’s talk about diabetes)
measures the amount of glycosylated hemoglobin (portion of Hgb that has glucose attached to it) over a 3-month span
used to screen, diagnose, and monitor diabetes
separate measurement from CMP/BMP panels
given as a percentage
Hgb A1c <5.7% = normal level
Hgb A1c 5.7-6.4% = pre-diabetes
Hgb A1c 6.5-7.9% = diabetic patient
Hgb A1c >8% = poorly controlled diabetic
Coagulation Markers
Labs: measure TIME needed to clot
PT: prothrombin time (12-15 secs)
INR: international normalized ratio (0.8-1.2)
PTT: partial thromboplastin time (25-35 secs)
Medications:
Coumadin
Heparin:
Lovenox
Eliquis
Therapy is contraindicated if prothrombin time is 2.5x greater than reference range - could result in spontaneous bleeding
coumadin
acts on extrinsic clotting factors; measured by PT and INR
Heparin
acts on intrinsic clotting factors; measured by PTT
Lovenox
injectable anticoagulant; does not require monitoring; peak effectiveness at 3-5 hours after administration
Eliquis
oral anticoagulant; does not require monitoring; peak effectiveness at 1.7 hrs after administration (many others)
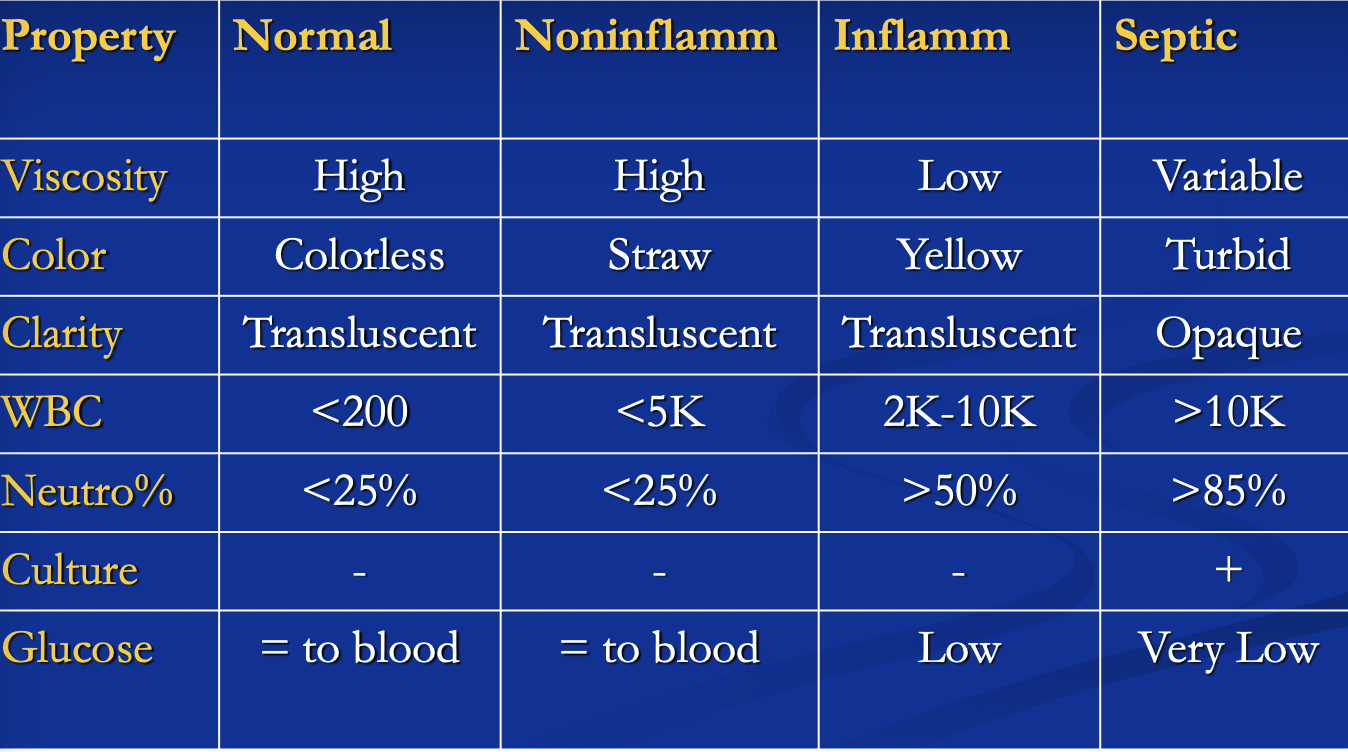
Red Incision
aspiration performed by the orthopedic provider reveals turbid, opaque fluid with > 10k WBC and low glucose
ESR = 78, CRP = 3.6, WBC = 15k
the surgeon schedules the patient for an I&D of the joint, IV antibiotics, and possible extraction of the hardware with revision anthroplasty
Red Incision Lab Values
C-Reactive Protein (CRP = 3.6 (normal range 0.0-1.0mg/dL)
erythrocyte sedimentation rate (ESR) = 78 (normal range 0-20 mm/hr)
joint fluid analysis
erythrocyte sedimentation rate (ESR)
during inflammation, fibrinogen increases causing RBCs to stick together becoming heavy
rate of settling of RBCs in anticoagulated blood measured in mm/hr
marker of inflammation, infection, or neoplastic process
indications infection or inflammatory conditions (RA, myopathy, not OA)
high sensitivity, low specificity
C-Reactive Protein (CRP)
also a marker of inflammation
an acute phase protein produced by the liver
elevated earlier than ESR in acute inflammation
6-8 hrs inflammatory process
can be used instead of/in conjunction with an ESR level
antinuclear antibody (ANA)
screening test for autoimmune disease
seen in systemic lupus erythematosus (SLE), rheumatoid arthritis (RA), scleroderma, polymyositis, dermatomyositis
absence rules out SLE
found in 3-4% of the normal population
normal titers: 1:20-1:40 blood volume to dilution agent; ANA still detectable
higher titers (i.e. 1:160) necessitates further workup
Rheumatoid factor (RF)
usually present in RA 75% of the time and occasionally in other connective tissue diseases
Normal is <15 U/mL
absent in early RA
absent (RF-) in seronegative spondyloarthropathies (types of inflammatory diseases that affect the spine and nearby joints)
Thyroid Stimulating Hormone (TSH)
is a peptide hormone synthesized & secreted by the anterior pituitary. It regulates secretion of thyroid hormones
often overlooked cause of diffuse joint pain & myalgias
usually affects shoulders & hips
may experience swelling of knee joint & small joints of hands & feet similar to rheumatoid disease
considered an autoimmune disease; women are more commonly affected than men with a 4-6:1 ratio
Human Leukocyte Antigen B27 (HLA-B27)
HLAs are glycoproteins found on the surface of the leukocytes; used in cell communication
can be found in up to 10% of the population
present in seronegative spondyloarthopathies
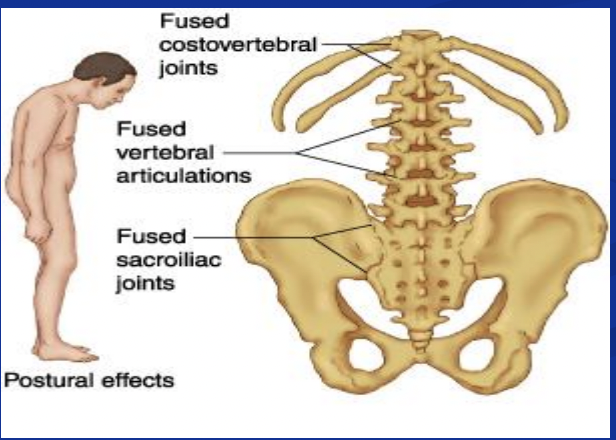
a spondyloarthopathy is any joint disease involving the vertebral column
seronegative
means rheumatoid factor is NOT present in the patient’s serum
Seronegative Spondyloarthropathies (HLA-B27 +, RF-, ANA-)
ankylosing spondylitis (90%)
reactive arthritis/formerly reiters syndrome (75%)
psoriatric arthritis/arthritis of ulcerative colitis or Crohn’s
Creatine Kinase/Creatine Phosphokinas (CK or CPK)
muscle enzyme present in sarcoplasm
mechanism: injury or disease of skeletal (CK-MM) or cardiac muscle (CK-MB) releases it into blood stream
Normal levels (24-194 IU/L)
seen with MI, CVA, inflammatory myopathies, rhabomyolysis, trauma, post surgical, vigorous exercise; reaction to cholesterol-lowering drugs (statins)
Uric Acid
elevated in purine-rich diet (organ meats, sardines, seafood), high fructose diet, alcohol
3.6 mg/dL to 8.3 mg/dL considered normal levels
increased in gout, renal disease, dehydration, chemotherapy
gout attacks can occur due to beer consumption, diuretics, trauma, obesity