Ch. 53 - Disorders of the Female Reproductive System
1/172
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
173 Terms
Gerontological considerations for female reproductive system
-vaginal flora change with age, causing the environment to become more alkaline, predisposing older women to vaginitis
-older women may develop perineal pruritis associated with diet, type of clothing worn, vaginal discharge, or other factors
-older women who experience uterine prolapse must carefully consider risks and benefits of various types of surgery, especially if surgery may have an impact on other chronic conditions
Disorders of Menstruation
-premenstrual syndrome (PMS)
-dysmenorrhea
-amenorrhea & oligomenorrhea
-premature ovarian failure
-polycystic ovarian syndrome
-menorrhagia
-metrorrhagia
-menopause
Premenstrual Syndrome (PMS)
a group of physical and emotional symptoms that occur in some women 77-10 days before menstruation
Causes of premenstrual syndrome (PMS)
Unknown, but may be from:
-excess estrogen, deficient progesterone, or both
-hypothalamic-pituitary dysregulation
-effect of reproductive hormones on brain chemicals such as endorphins, melatonin, and serotonin
Symptoms of premenstrual syndrome (PMS)
-weight gain
-headache
-nervousness
-irritability
-personality changes
-depression
-abdominal bloating
-pain or tenderness of the breasts
-breast enlargement
-craving for sweets
-swelling of ankles, feet, and hands
-anxiety
-increased physical activity
Diagnosis of premenstrual syndrome (PMS)
-data from a menstrual diary in which the client keeps daily recordings of her symptoms for at least 2 months
-classic finding: patient is symptom-free during the period between the onset of menstruation and ovulation
Treatment of premenstrual syndrome (PMS)
-hormonal drug therapy aims at manipulating the cyclic fluctuation in estrogen and progesterone (oral contraceptives, progesterone, synthetic androgens, gonadotropin-releasing hormone analogs, and nafarelin)
-short-term therapy with tranquilizers or antidepressants has been beneficial
-nonopioid analgesics for discomfort
-vitamin and mineral supplements may relieve symptoms
Recommendations for patients with premenstrual syndrome (PMS)
-eat 6 small meals per day
-increase complex carbs
-increase foods high in calcium
-reduce sugar and salt
-reduce or eliminate caffeine
-eliminate alcohol prior to menstruation
-aerobic exercise 30 mins most days of the week
-get sufficient sleep every night
-manage stress effectively
-take NSAIDs with food to decrease GI upset
Nutritional notes for premenstrual syndrome (PMS)
-vitamin B6: relieves irritability, fatigue, and depression
-vitamin E: reduce breast tenderness
-calcium: relieves bloating and body aches
-magnesium: relieves pain, water retention, and dysphoria
Dysmenorrhea
-painful menstruation
-primary: idiopathic, no abnormality found
-secondary: result of other disorders (endometriosis, displacement of uterus, fibroid uterine tumors)
Treatment for dysmenorrhea
-mild nonnarcotic analgesics
-treating underlying cause
-hormonal contraceptives
-heating pad/bottle
-knee-chest position to relieve discomfort caused by retroversion (backward tilt) of uterus
-adequate rest
-good nutrition
-stress relief
Assessment findings for dysmenorrhea
-lower abdominal pain
-cramping
-more severe with fatigue, cold, and tension
Amenorrhea and Oligomenorrhea
Amenorrhea
absence of menstrual flow
Oligomenorrhea
infrequent menses
Primary amenorrhea
when a woman of reproductive age has never menstruated
Secondary amenorrhea
if menstruation stops after menstrual cycles have occurred
-during pregnancy
-after menopause
-when ovaries or uterus are surgically removed
-some medications
-stress
-poor nutrition
Causes of amenorrhea and oligomenorrhea
-endocrine imbalances resulting from pituitary disorders (hypothyroidism)
-stress
-severely lean body mass
-anorexia
-low levels of estrogen
-premature ovarian failure (POF)
-polycystic ovarian syndrome (PCOS)
Treatment of amenorrhea and oligomenorrhea
correcting underlying cause
Premature ovarian failure (POF)
-a disorder where the ovaries cease to function in women younger than 40 years of age
-follicles do not respond to FSH or ovarian follicles are depleted
Causes of premature ovarian failure (POF)
-autoimmune attack that destroys the ovarian follicles
-the follicle that is programmed to mature with stimulation of FSH lacks the support of other less mature follicles to help its development. The dominant follicle becomes luteinized but it does not release an ovum
Assessment findings of premature ovarian failure (POF)
-irregular menses
-symptoms that resemble natural menopause
Diagnostics for premature ovarian failure (POF)
-determine level of FSH in the blood
-a higher-than-normal level of FSH combined with the history of irregular menses or premature cessation of menstruation suggests POF
Polycystic ovarian syndrome (PCOS)
-endocrine disorder associated with chronic anovulation
-affects women 20 - 40 years old
-affected follicles neither secrete progesterone that suppresses menstruation nor release an ovum
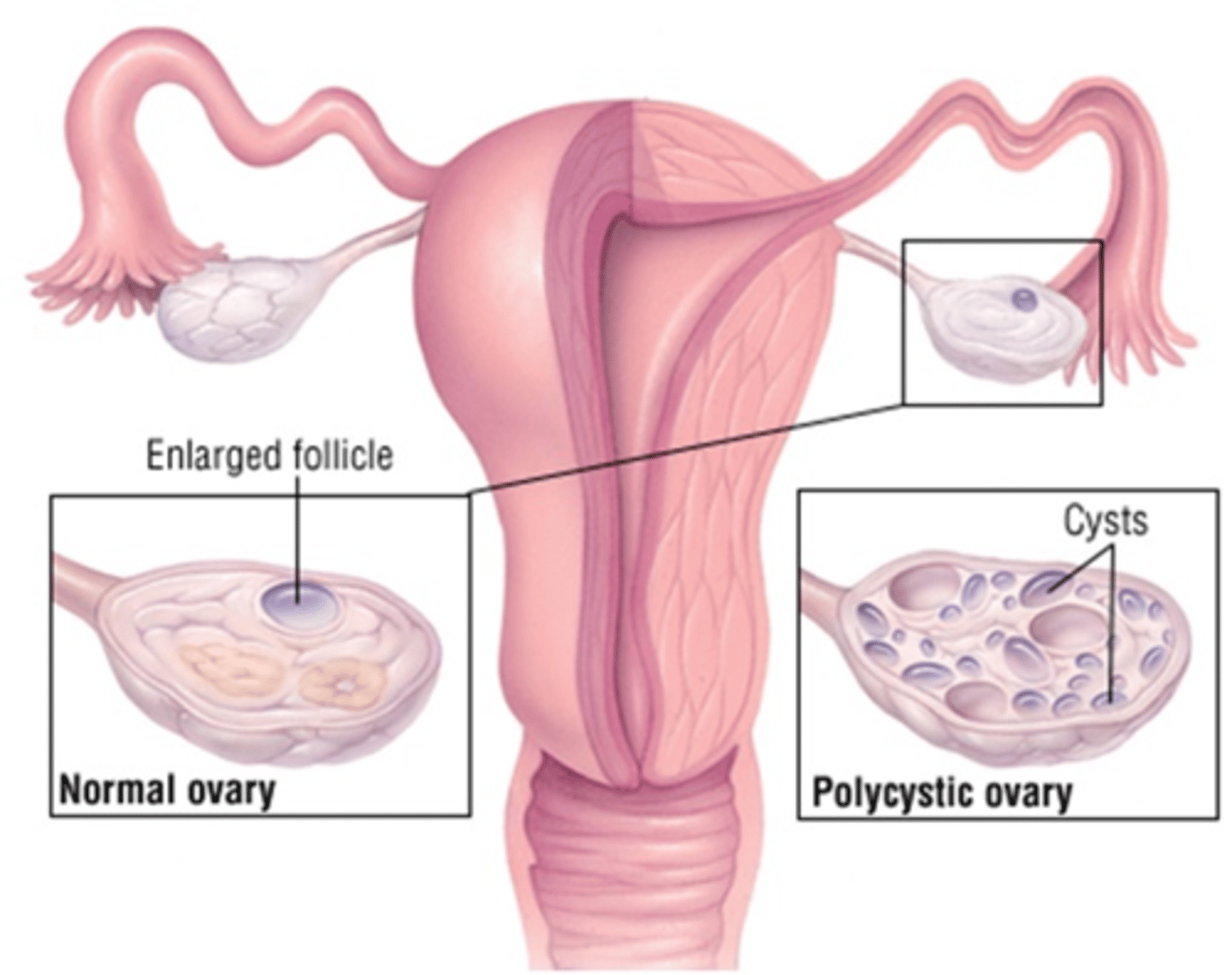
Assessment findings for polycystic ovarian syndrome (PCOS)
-amenorrhea & oligomenorrhea
-fluid-filled cysts in the ovarian follicles
-overproduction and inefficient use of insulin
-high testosterone levels
-weight gain
-excessive growth of body hair
-acne
-thinning hair or baldness
-abnormal lipid levels
-hypertension
-difficulty becoming pregnant
Diagnostics for polycystic ovarian syndrome (PCOS)
-palpate for enlarged ovaries
-vaginal ultrasonography
-blood tests to measure hormone levels
Treatment for polycystic ovarian syndrome (PCOS)
-oral contraceptives to offset excess of testosterone and to regulate menstrual cycle
-for those who want to conceive: oral hypoglycemic agent (meformin) and progestin-containing medications
-lipid-lowering agents
-antihypertensives
Menorrhagia
excessive bleeding at time of normal menstruation
Determined by one of these:
-menstrual flow that lasts more than 7 days
-requires the use of an additional 2 pads per day
-extends 3 or more days longer than usual
Causes of menorrhagia
-endocrine disorder
-coagulation disorder
-systemic disorders
Treatment of menorrhagia
-NSAIDs (reduce prostaglandins that exist in endometrial tissue where they exert a stimulating effect on the uterus)
-progestins
-hormonal contraceptives with combos of estrogen and progestin (transform the proliferative endometrium into a secretory endometrium that stimulates a pregnant state)
-dilation and curettage (D&C) for symptomatic relief
-endometrial ablation (via photodynamic therapy or uterine balloon therapy)
Endometrial ablation
-detachment of the lining of the uterus
-done by photodynamic therapy or uterine balloon therapy
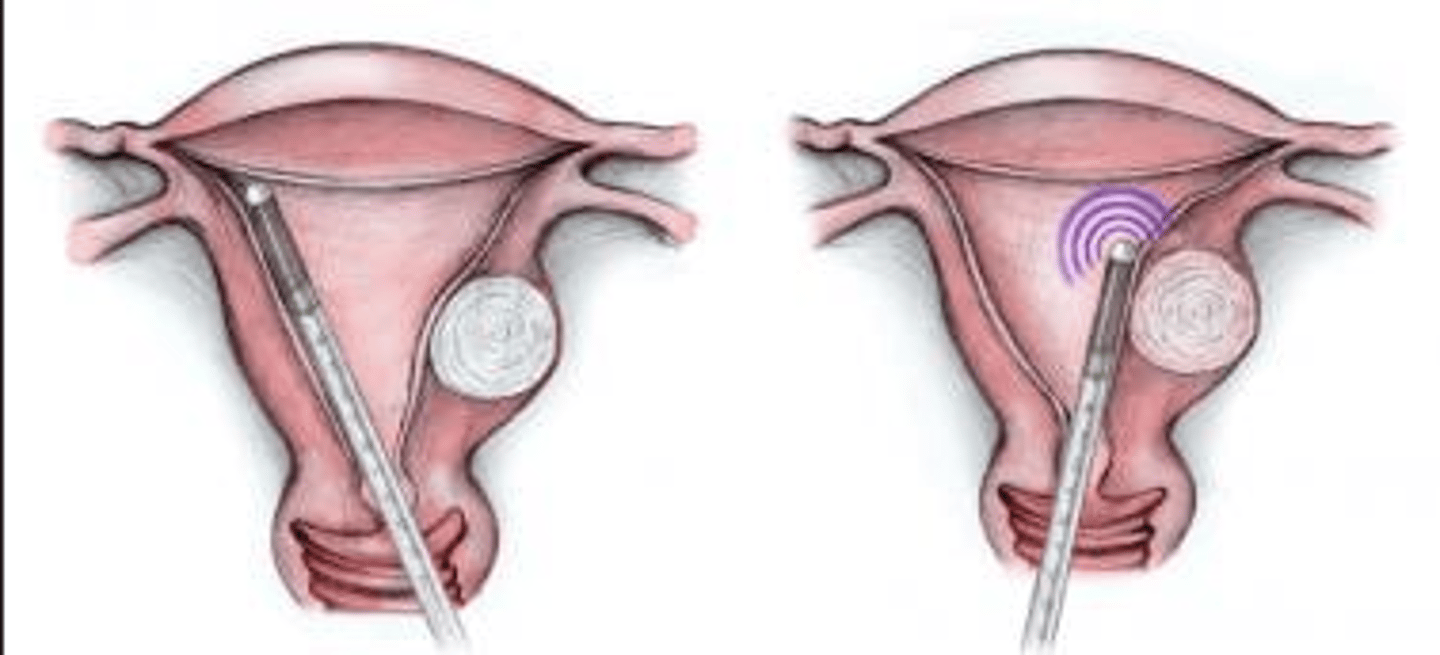
Endometrial ablation: Photodynamic therapy
-a light-sensitive substance is applied to endometrial tissue
-a laser probe is then inserted through the cervix
-the absorption of laser light by the tissue causes the endometrium to slough
-in contrast to being removed with a surgical curette
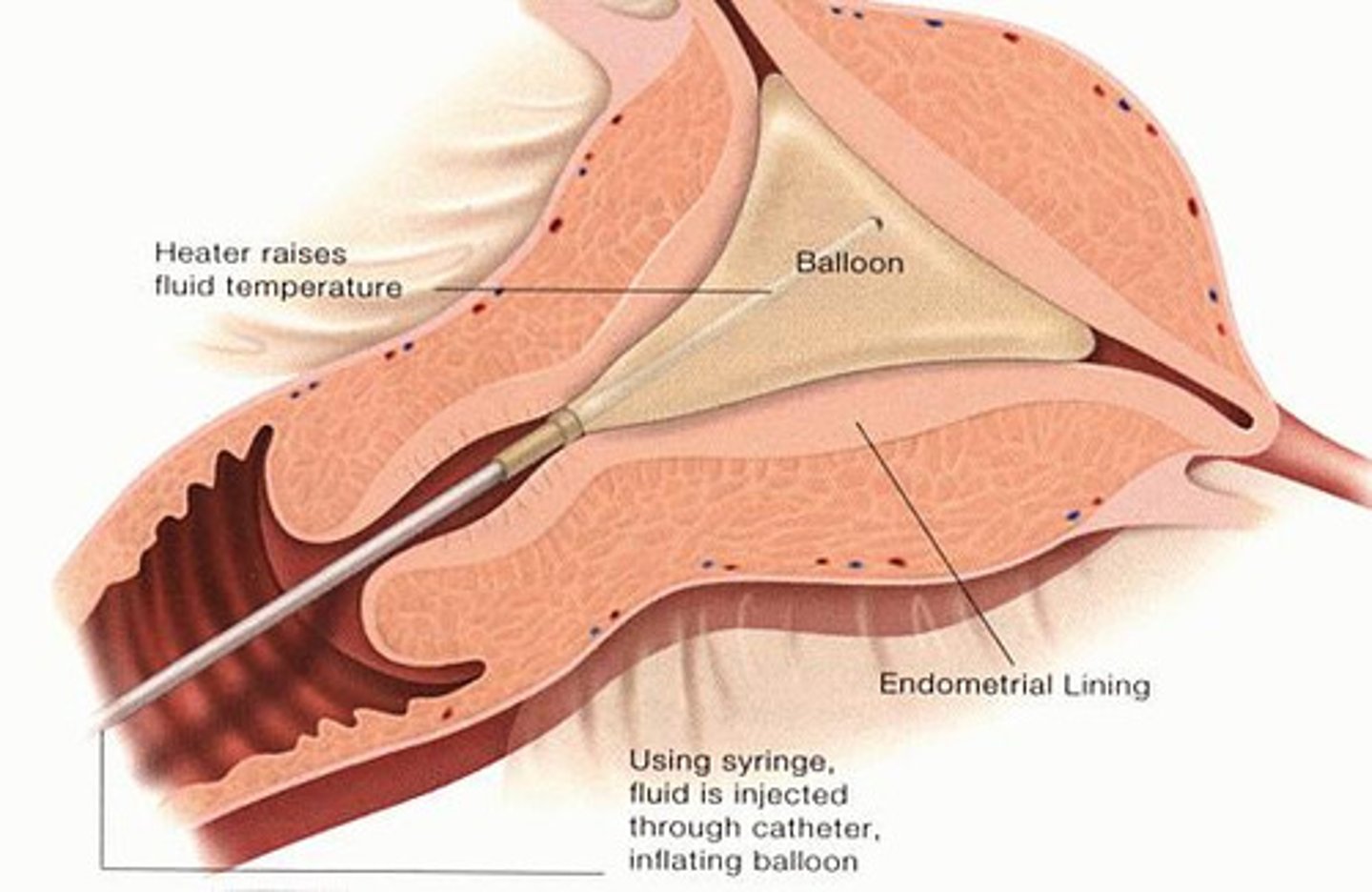
Endometrial ablation: Uterine balloon therapy
-a balloon is inserted into the uterus
-balloon is filled with an isotonic saline solution
-the solution is heated to 87 degrees for 8 minutes
Metrorrhagia
-vaginal bleeding at a time other than menstruation
-amount of blood is not important, just that it is occurring
Causes of metrorrhagia
-erratic stimulation of or response to pituitary or ovarian hormones (especially in adolescent girls and perimenopausal women)
-uterine malignancies
-cervical irritation
-breakthrough bleeding that occurs with hormone replacement therapy (HRT) or low-dose hormonal contraceptives
-intermenstrual or postcoital bleeding needs to be evaluated promptly
Treatment for metrorrhagia
treat the underlying cause
Menopause
-cessation of the menstrual cycle
-a natural physiologic process that happens between 45-55 years of age
Peri-menopause
-the time during which ovarian activity gradually ceases
-vasomotor disturbances such as hot flashes accompanied by sweating, sleep disturbance, and irritability or depression, vaginal dryness, diminished libido, dyspareunia (discomfort during intercourse)
Post-menopause
begins 1 year after menstruation ceases
Surgical menopause
menopause induced by the removal of the ovaries
Physiology of menopause
-when the ovarian function diminishes
-levels of estrogen and progesterone are reduced
-ovulation gradually ceases
-menstruation becomes irregular until it stops
-natural reproductive capacity ends
-as the levels of estrogen and progesterone drop, the hypothalamus attempts to raise them by releasing GnRH which stimulates the anterior pituitary gland to release FSH and LH
-this surge of hypothalamic-pituitary stimulation is thought to be responsible for alterations in temp regulation, sleep disturbances, and disequilibrium in mood
Assessment findings for menopause
-estrogen deficiency causes thinning of vaginal walls, breast and uterine atrophy, and loss of bone density
-increased risk of heart disease and stroke as estrogen decreases
-depression related to social or pscyhological implications of menopause
-changing menstrual patterns (irregular periods, scanty or sometimes unusually copious menstrual flow)
-hot flashes
-dyspareunia (discomfort during sex)
-sleep disturbances
-irritability
-vaginal dryness
-diminished libido
-weight gain
Medical management of menopause
-hormone replacement therapy
-antidepressants and minor tranquilizers
-ointments for vaginal dryness
-bisphosphonates to reduce potential for osteoporosis
-bioidentical hormones
Hormone replacement therapy (HRT)
-estrogen with or without progestin
-causes increased risk of breast cancer, heart disease, blood clots, stroke, gallbladder disease, and dementia
-prescribed in lowest appropriate dose for the shortest time necessary
-estrogen in small doses can help prevent osteoporosis and relieve menopausal symptoms
Bisphosphonates
-aldendronate (Fosamax)
-inhibits bone resorption
-used to prevent osteoporosis
-take with water and sit up 30 minutes after
Bioidentical hormones
-prescription substances made from soy and yams
-indistinguishable and similarly effective as those from naturally occurring estrogen and progesterone
-diets rich in phytoestrogens, such as isoflavones in soy products and lignans in flaxseed, may reduce menopausal symptoms, especially hot flashes
Nursing management for menopause
-collects relevant menstrual, reproductive, sexual, and psychosocial history
-prepare and support during diagnostics
-health teaching topics such as normal developmental changes, coping strategies, health promotion techniques, methods to achieve symptomatic relief, and treatment-related information
-recommends regular gynecological and breast exams
-patient teaching
Patient teaching for menopause
-use bland skin creams or lotions to reduce skin dryness
-use a water-based lubricant prior to intercourse for vaginal lubrication
-plan an exercise program to prevent weight gain and loss of calcium from the bones
-increase calcium intake by eating calcium-rich foods or by taking a calcium supplement containing vitamin D
-discuss with the prescriber the benefits, risks, and alternatives for HRT
-discuss a schedule for routine gynecologic and breast exams
-contains the provider if breakthrough vaginal bleeding or other symptoms occur while taking hormonal replacement
-cultivate new interests and hobbies or resume those that have been abandoned because of other responsibilities
Infectious and Inflammatory Disorders
-vaginitis
-cervicitis
-pelvic inflammatory disease (PID)
-toxic shock syndrome (TSS)
Vaginitis
inflammation of the vagina
Causes of vaginitis
-chemical or mechanical irritations
-feminine hygiene products
-allergic reactions
-age-related tissue changes (atrophic vaginitis with menopause)
-infections
-antibiotics or douching (eliminate the bacilli that promote an acidic vaginal environment)
Which 3 infections are most associated with vaginitis?
1. bacterium Gardnerella vaginalis
2. protozoan Trichomonas vaginalis
3. yeastlike fungus Candida albicans
Pathophysiology of vaginitis
-the vagina is typically self-protected by mucus-secreting cells and acidic environment, but the tissue can become disrupted
-protective mechanisms are altered
-decreased estrogen at menopause reduces the thick, moist consistency of vaginal tissue
-pregnant women, those with unregulated diabetes, and those who take hormonal contraceptives containing estrogen have an excess of glycogen in vaginal mucus which supports the growth of microorganisms
Assessment findings for vaginitis
-abnormal vaginal discharge
-characteristics of the discharge often are indicative of the infecting organism
-itching, burning, redness, swelling of surrounding tissues
Medical management of vaginitis
-antifungal, antiprotozoal, and antibiotics for the pathogen
-may need to treat sexual partner too
-atrophic vaginitis relieved with estrogen replacement administered as a topical cream
-for diabetics, regulating BG is an important part of treatment
Nursing management of vaginitis
-explain that a panty liner can be worn after vaginal insertion of medications to prevent staining of clothing or linens
-tell patient to not douche before exam
-teach client how to insert vaginal medications
-encourage patient to take Lactobacillus acidophilus in capsules form or eating yogurt containing live cultures of lactobacilli to replenish normal vaginal microorganisms
-sitz baths to relieve itching, burning, and swelling of the vulva and perineum
-skin protectants containing zinc oxide promote healing
-teaching to prevent vaginal infections
Patient teaching for prevent vaginal infections
-bathe daily with particular attention to perineal hygiene
-wipe from front to back after bowel movements
-avoid feminine hygiene products and douching more than once per week
-wear cotton undergarments and change them daily
-refrain from wearing layers of clothing, such as underwear plus pantyhose plus slacks, which increases warmth and interferes with air circulation around the genital area
-change from a wet swimsuit as soon as possible
-wash hands and devices that are inserted into the vagina, such as medication applicators, douche tips, and diaphragms, and store them in clean containers
-change sanitary pads before they become saturated, substitute a sanitary pad for a tampon at night
-use a condom or avoid intercourse if either client or her sex partner has genitourinary symptoms
Cervicitis
inflammation of the cervix

Causes of cervicitis
-infectious microorganisms
-decreased estrogen levels during menopause
-trauma during gynecologic procedures
-inserting tampons or vaginal medication applicators
-streptococcal, staphylococcal, gonorrheal, and chlamydial infections
Consequences of cervicitis
-potential is greater during pregnancy and after childbirth when the microorganisms can enter cervical tissue through small lactations
-the infection can travel upward through uterine and tubal structures leading to pelvic inflammatory disease
-inflammation and subsequence formation of scar tissue increases the potential for ectopic pregnancy or difficulty conceiving
-chronic cervicitis decreases the amount and quality of cervical mucus and alters the pH, both of which are underlying causes of infertility
Assessment findings for cervicitis
-early cervicitis may be asymptomatic
-spots or bleeds intermenstrually
-may develop vaginal discharge
-dyspareunia (painful intercourse) or slight bleeding after sex
-severe cervicitis can cause sensation of weight in the pelvis
Diagnostics of cervicitis
-visual examination of the cervix
-cervical smears c&s
Medical management of cervicitis
-douching
-local or systemic antibiotics
-chronic cervicitis: electrocautery (heat-generating device) (frank bleeding requires cervical or vaginal packing or electric coagulation of the bleeding vessels)
-severe chronic cervicitis: conization (removal of the diseased portion of the cervical mucosa)
Electrocautery
use of an instrument heated by electric current (cautery) to coagulate bleeding areas by burning the tissue (e.g., to sear a blood vessel)

Nursing management of cervicitis
-schedules treatment procedures 5-8 days after the end of the menstrual period to reduce potential for bleeding
-explains that momentary cramping sensation may be felt during the electrocautery procedure
-explains post-electrocautery instructions
Post-electocautery instructions for the client
-rest more than usual for 1-2 days
-avoid straining or heavy lifting
-rest in bed and report if slight bleeding does occur
-frank bleeding requires a return visit to the primary care provider
-expect a grayish-green, malodorous discharge for about 3 weeks after cautery
-anticipate slight bleeding about the 11th day
-return for a follow-up visit to the primary care provider in 2-4 weeks
-abstain from sexual relations until tissues are healed
-expect that healing may take 6-8 weeks
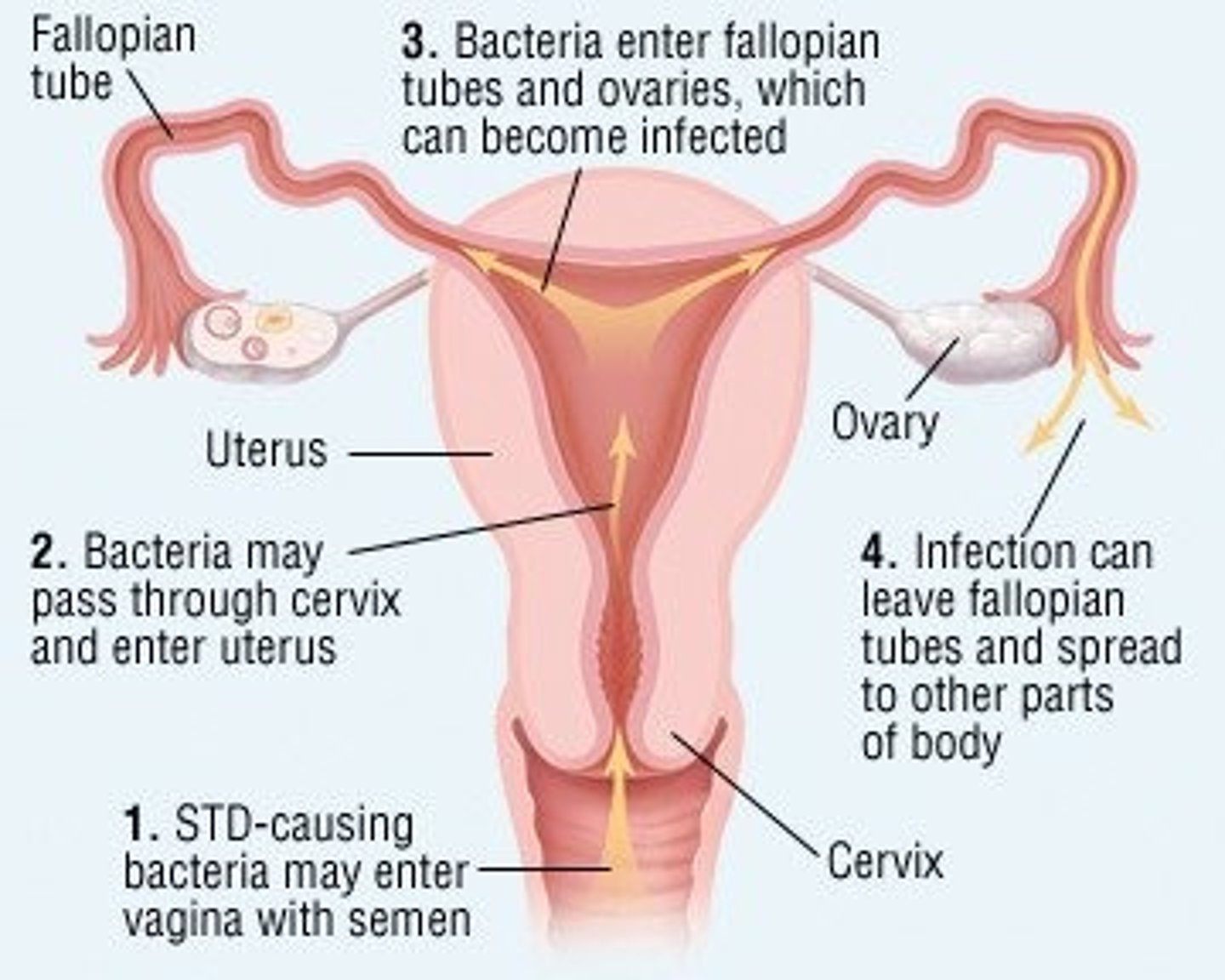
Pelvic Inflammatory Disease (PID)
an infection of the pelvic organs other than the uterus, including the ovaries, fallopian tubes, pelvic vascular system, and pelvic supporting structures
Pathophysiology and etiology of PID
-microorganisms enter pelvic structures through the cervix from the vagina
-the causes usually is bacterial with gonoccoi and Chlamydia trachomatis being the most common pathogens
-infection travels up the uterus to the fallopian tubes and ovaries and can result in a pelvic abscess
-can cause peritonitis as pus from the infected tubes leaks into the abdomen
Assessment findings for PID
-infectious malodorous discharge
-backache
-severe or aching abdominal and pelvic pain
-bearing-down feeling
-fever
-dyspareunia
-nausea/vomiting
-pain during pelvic exam
-severe may cause urinary symptoms
Diagnostics for PID
-gynecologic exam
-c&s test of vaginal discharge is obtained
-US, MRI, or CT may disclose pelvic abscess
Medical management of PID
-hospitalization with complete bed rest is often necessary
-parenteral or oral antibiotics
-IV fluids are ordered if the client is dehydrated
-antipyretics if fever
-ruptured pelvic abscess requires emergency surgery
Toxic Shock Syndrome (TSS)
-a type of septic shock
-life-threatening systemic reaction to the toxin produced by several kinds of bacteria
Microorganisms that cause TSS
-Staphylococcus aureus
-Streptococcus pyogenes
-Clostridium sordellii
Pathophysiology and etiology of TSS
-associated with the use of superabsorbent tampons that are not changed frequently and internal contraceptive devices that are left in place longer than necessary
-virulent bacteria reproduce suddenly and abundantly in the body and remain unchecked by normal physiologic defense mechanisms
-bacteria produce chemicals that cause blood vessels to dilate, which keeps the major portion of the blood volume in the periphery, reduces cardiac output, and causes severe hypotension (shock)
-toxin also inhibits the ability of affected cells to use oxygen
Assessment findings for TSS
-sudden onset
-high fever
-chills
-tenderness or pain in muscles
-nausea/vomiting
-diarrhea
-hypotension
-hyperemia (increased redness and congestion) of vaginal mucous membranes
-disorientation
-headaches
-skin is warm despite client being in shock
-rash on the palms of the hands or body a few hours after infection later results in shedding of the superficial layer of skin (desquamation)
-pulse is rapid and thready
Diagnostics for TSS
-c&s of blood, urine, vagina, or other sites
-BUN, creatinine, and bilirubin levels increase (kidney values increase)
-AST and ALT increase (liver values increase)
-platelet count may decrease
Medical management of TSS
-circulation is supported with IV fluids
-IV antibiotics (oxacillin, nafcillin, methicillin)
-potent adrenergic drugs are given to counteract peripheral vasodilation and maintain renal perfusion (dopamine, dobutamine)
-oxygen therapy to promote aerobic metabolism at cellular level
Nursing management of TSS
-assess vital signs
-administer abx
-applies pressure to venipuncture or injection sites to control bleeding and oozing if platelet count is low
-measure I&O
-notify provider of output of less than 500 mL/day
-teach preventive measures such as using perineal pads rather than tampons or change tampons more often; patients using a diaphragm, vaginal sponge, or cervical camp for birth control should remove the device within 24 hours after use; emphasizes hand hygiene and keeping vaginal devices clean
Structural Abnormalities
-endometriosis
-vaginal fistulas
-pelvic organ prolapse
-uterine displacement
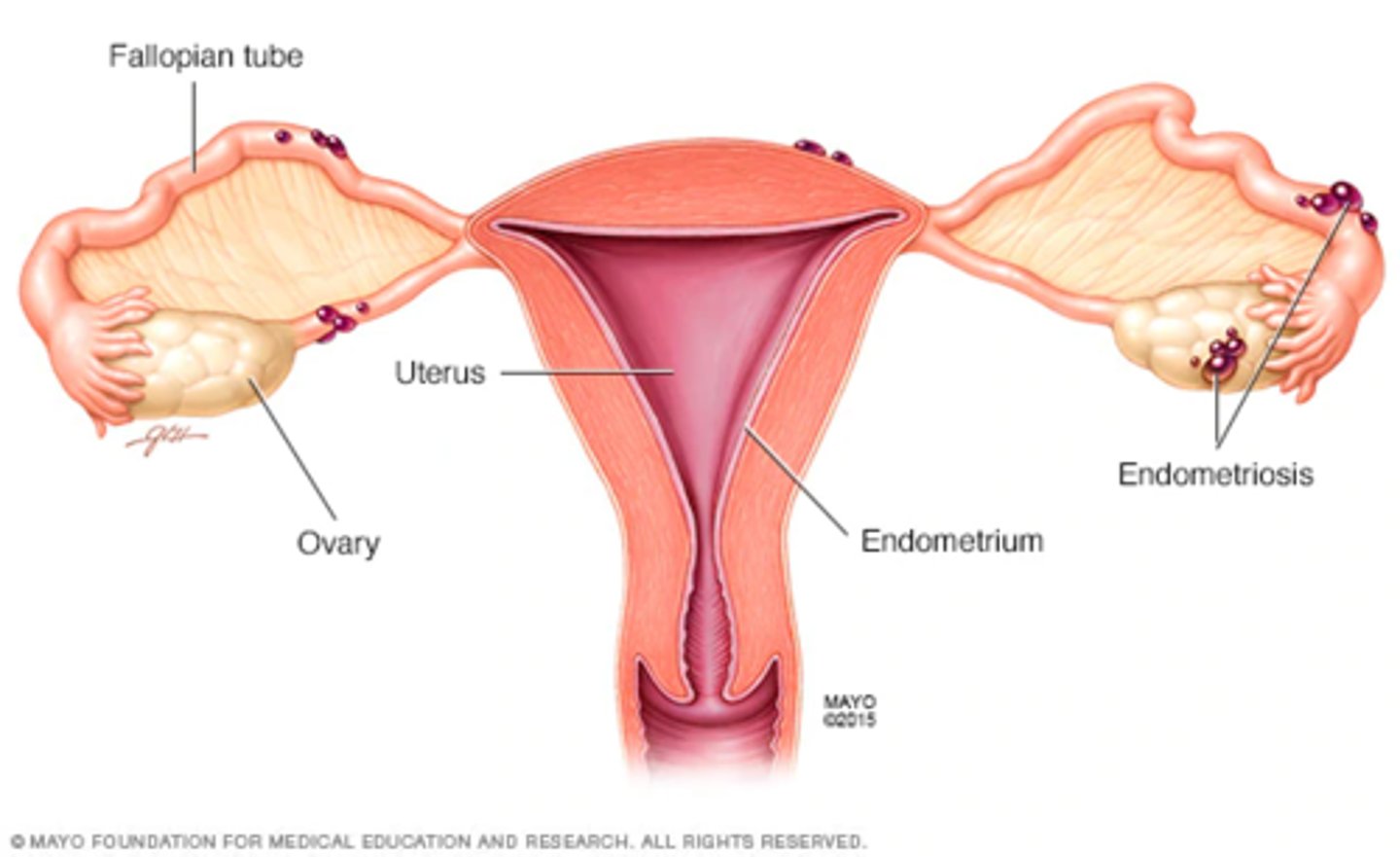
Endometriosis
-a condition in which tissue with a cellular structure and function resembling that of the endometrium is found outside the uterus
-atypical locations include ovaries, pelvic cavity, abdominal cavity
Causes of endometriosis
-not clearly understood
-may result from remnants of embryonic tissue that remain in the abdominal cavity
-could be from retrograde menstruation in which the fallopian tubes expel fragments of endometrial tissue that eventually become implanted outside the uterus
Pathophysiology of endometriosis
-ectopic tissue responds to stimulation by estrogen and maybe progesterone
-tissue bleeds when the endometrium of the uterus is shed, but there is no outlet for the extrauterine bleeding
-trapped blood causes pain and ultimately adhesions in the peritoneal cavity
-if fallopian tubes are affected, they may become occluded and result in infertility
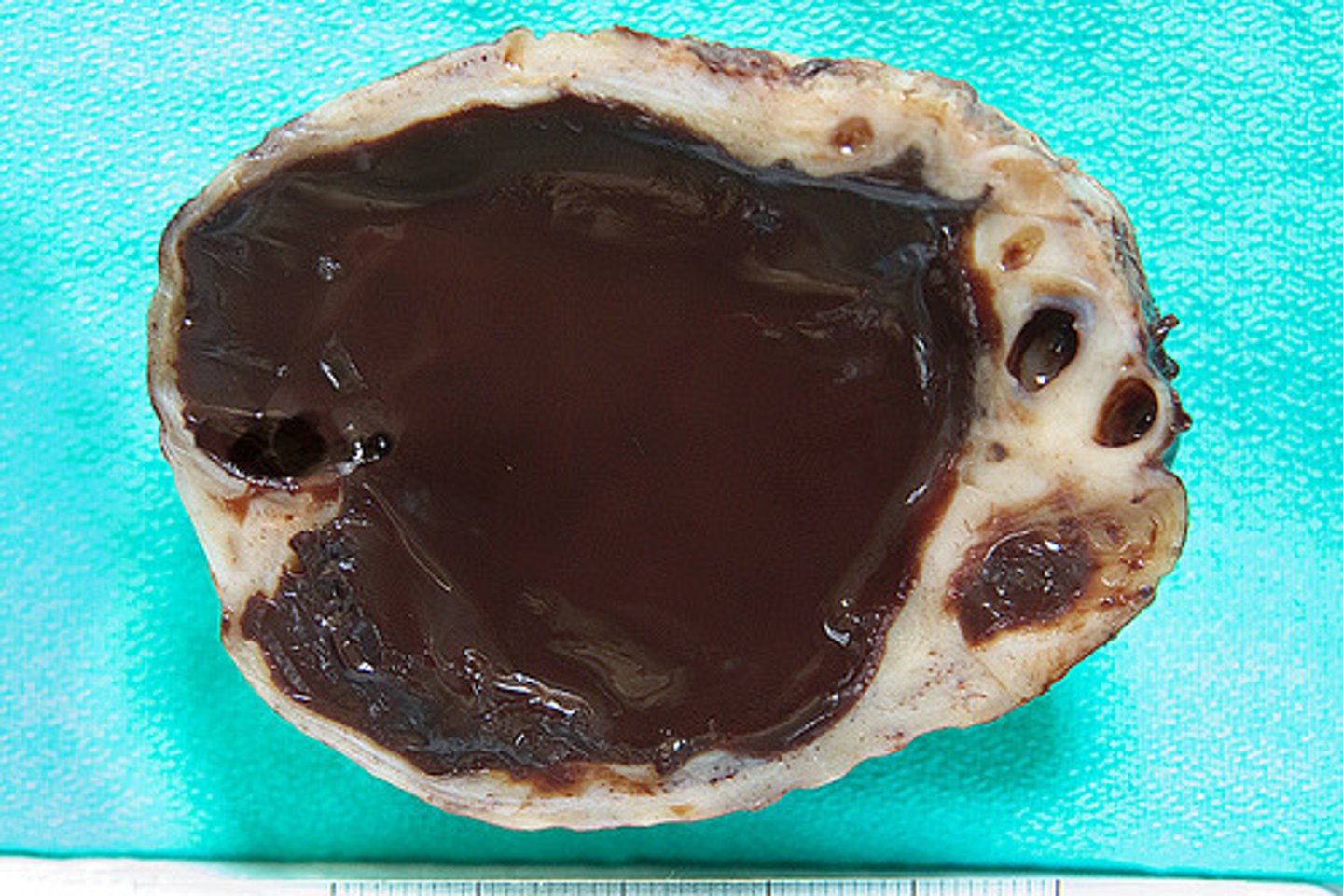
-if endometrial tissue is enclosed in an ovary, a "chocolate cyst" (collects dark blood) develops
-occasionally the cyst ruptures spilling old blood and endometrial cells into the pelvic or abdominal cavity
-condition is naturally relieved when endometrial tissue atrophies after menopause or regresses during pregnancy
Chocolate cyst
endometriosis in ovary
Assessment findings for endometriosis
-severe dysmenorrhea
-copious menstrual bleeding
-dyspareunia
-pain on defecation
-rupture of a chocolate cyst results in severe abdominal pain that can mimic other abdominal pathologies (appendicitis, bowel obstruction)
Dyspareunia
painful sexual intercourse
Diagnostics for endometriosis
-pelvic exam shows fixed, tender areas in the lower pelvis and restricted mobility of the uterus from adhesions
-laparoscopy confirms diagnosis
Medical management of endometriosis
-natural or surgical menopause
-to preserve the potential for having children, many women are managed medically as long as possible
-estrogen-progestin contraceptives are administered to keep the client in a non-bleeding phase of her menstrual cycle for about 9 months (norethindrone, danazol)
-goal is to control the ectopic tissue so that the client is symptom-free for several years
-surgery to remove cysts and much of the ectopic tissue as possible
-laparoscopy is used to remove small areas of endometrial tissue as well as relieve adhesions
-endometriosis that is widespread through the pelvic organs may necessitate a panhysterectomy
-elagolix (a GnRH receptor antagonist to suppress estogren)
Panhysterectomy
removal of the uterus, both fallopian tubes, and ovaries
Nursing management for endometriosis
-reinforce or clarify explanations of treatment options and the consequences of each option
-emphasize that the condition does not require an immediate decision and void giving advice or influencing the client's opinions
-suggest that the client include her significant other in the discussion of options
-offer the option of seeking a second medical opinion
-suggest the client list the pros and cons compatible with her values and goals
-help with pain management
-encourage regular gynecologic evaluations
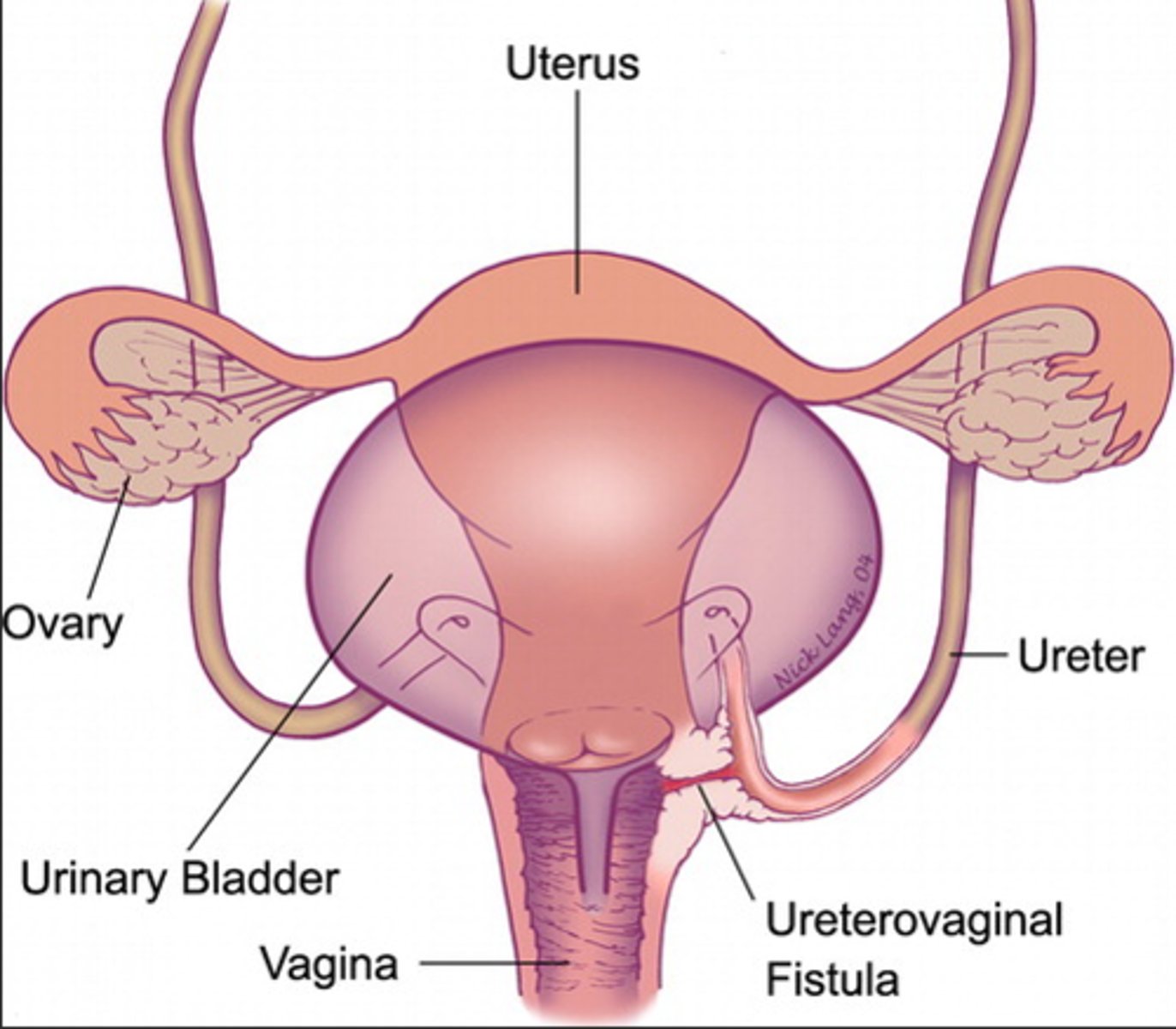
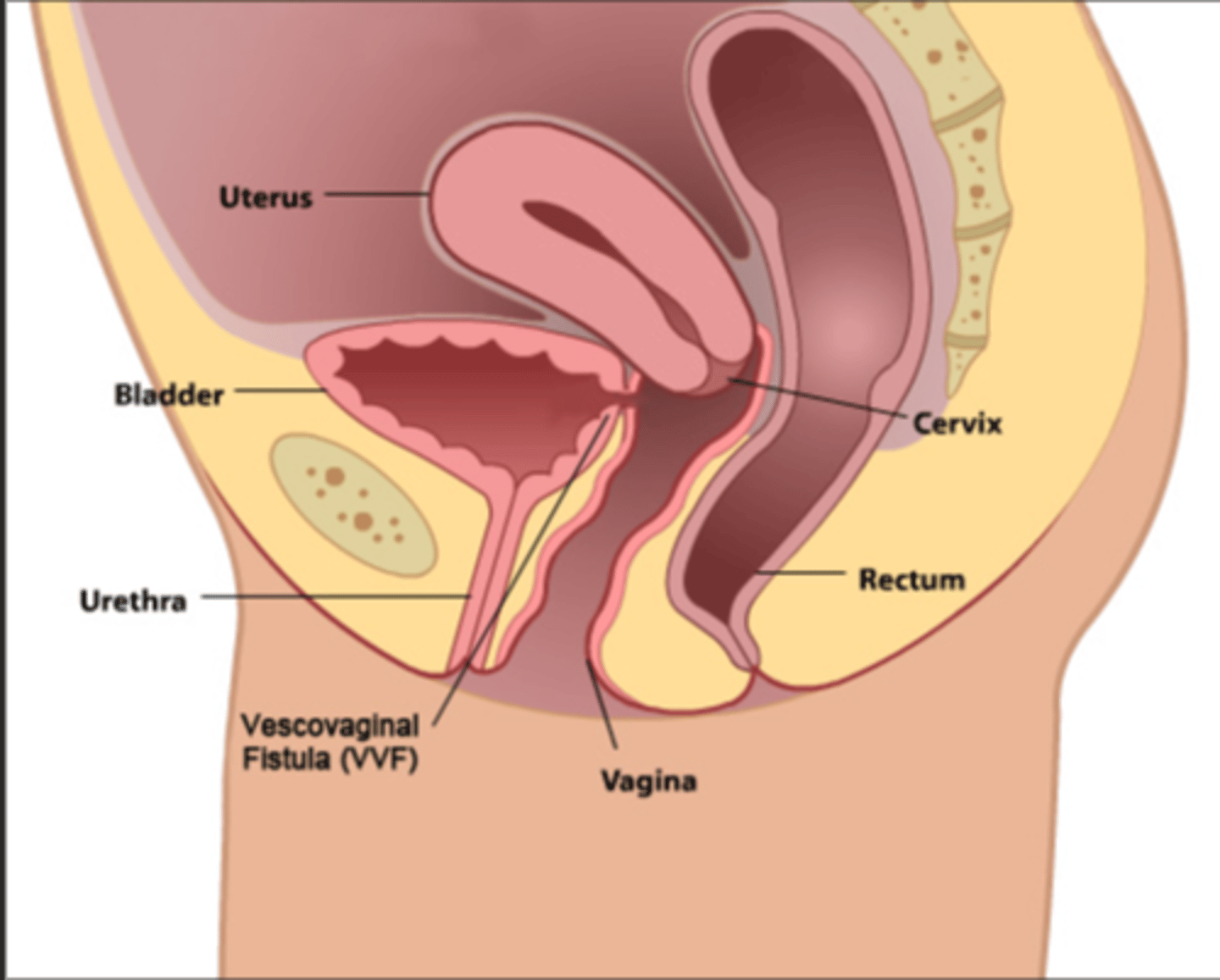
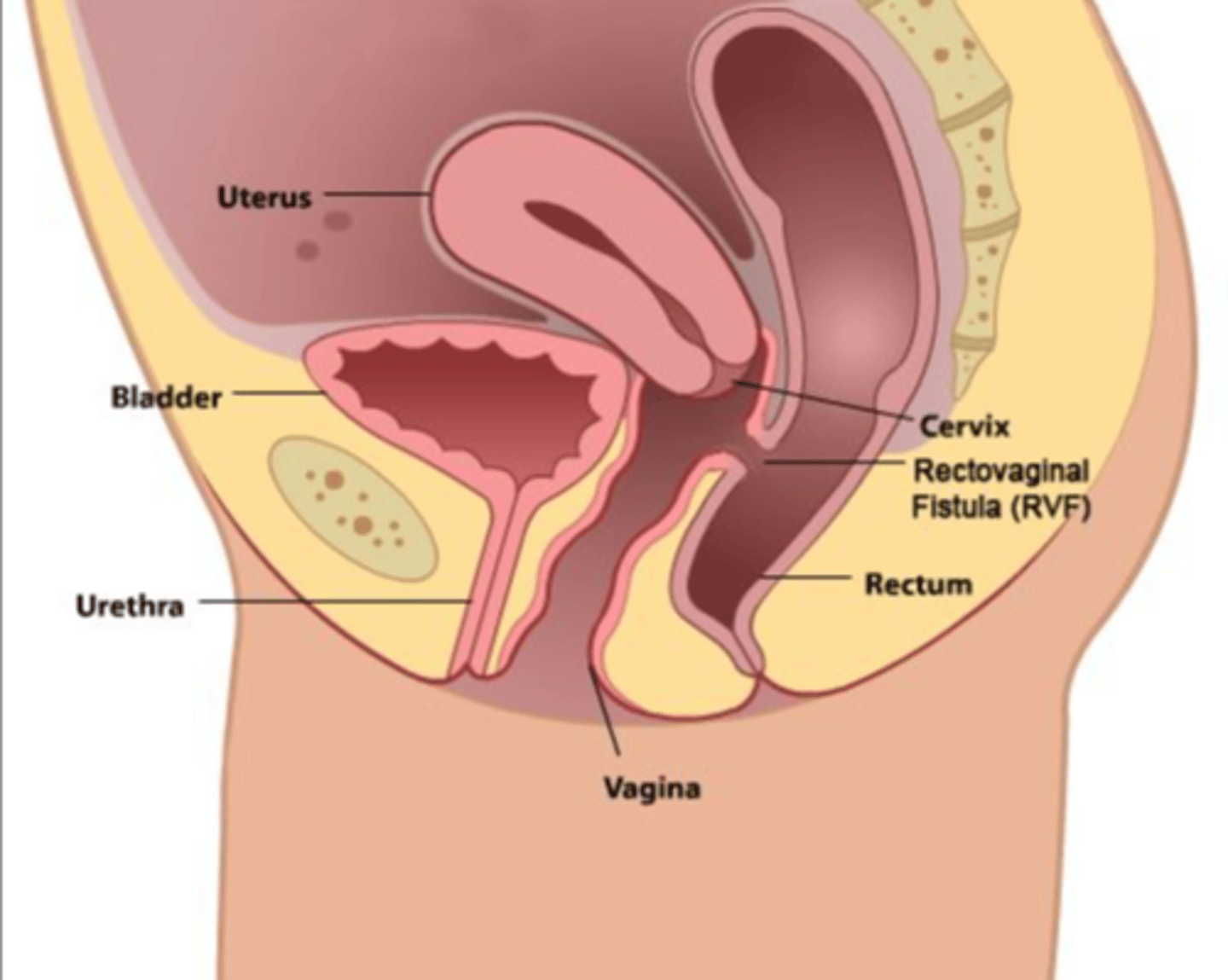
Vaginal fistula
an unnatural opening between a structure and the vagina
Ureterovaginal fistula
a fistula between the lower ureter and vagina
Vesicovaginal fistula
a fistula between the bladder and vagina
Rectovaginal fistula
a fistula between the rectum and vagina
Causes of vaginal fistulas
-cancer
-radiation treatment
-surgical or obstetric injury
-congenital anomaly
-complication of Crohn's disease
Complications of vaginal fistulas
-result in continuous drainage of urine or feces from the vagina
-often become infected
-vaginal wall and external genitalia become excoriated
-client may no void through the urethra because urine does not accumulate in the bladder
Assessment findings for vaginal fistulas
urine or stool leaks from vagina
Diagnostics for vaginal fistulas
-physical exam of vaginal wall
-sterile probe is inserted if the fistula is easily seen or a dye (methylene blue) is used to detect the exact location of the fistula
-vesicovaginal: colored dye instilled into bladder via urethral catheter
-ureterovaginal: dye given IV, IV pyelogram detects flow of radiopaque dye through lower GU tract
-rectovaginal: look for fecal drainage on the posterior vaginal wall
Medical management of vaginal fistulas
-surgery is performed after inflammation and edema have disappeared (may require months of treatment)
-sometimes the tissues are in such poor condition that surgical repair is not possible
-in the meantime, or if it cannot be repaired, symptomatic treatment to reduce the risk for infection and manage skin excoriation
Nursing management of vaginal fistulas
-before repair of rectovaginal fistula, administer neomycin, kanamycin, or any other prescribed abx to clean the bowel of microorganisms
-provide a light, low-residue diet to keep stool soft
-given an enema and a cleaning vaginal irrigation the morning of surgery
-insert an indwelling catheter to keep the bladder empty
Post-op nursing considerations for vaginal fistula repair
-serosanguineous vaginal drainage on perineal pad is normal
-no urine or feces from the vagina indicates healing of the repaired fistula
-prevent pelvic pressure and stress on the suture line by monitoring catheter drainage closely
-the pressure of a full bladder from an obstructed catheter may break down the surgical repair and cause the fistula to reappear
-prevent and relieve pressure on perineal structures
-warm perineal irrigations and heat lamp treatments are effective in promoting healing and lessening discomfort
-douches used during the post-op period remove drainage, keep the suture area clean, and lessen chances of infection
-about the 3rd of 4th post-op day, a rectal suppository or a stool softener may be ordered to prevent straining during a bowel movement
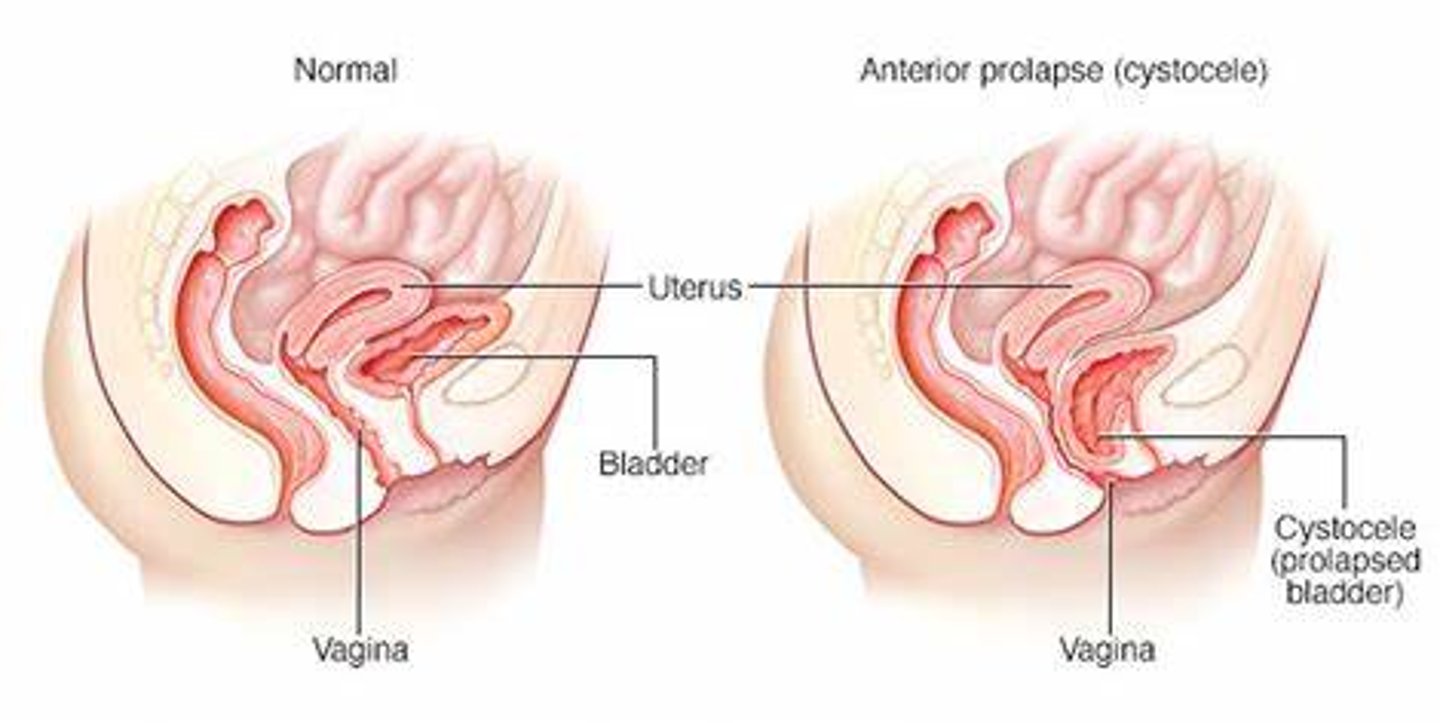
Pelvic Organ Prolapse
-prolapse is a structural protrusion
-can be cystocele, rectocele, enterocele, or uterovaginal prolapse
Cystocele
bulging of the bladder into the vagina