T1DM and emergent DM
1/94
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
95 Terms
What is Gluconeogenesis?
Produces glucose using amino acids, lactate, and glycerol for immediate energy needs in times of low insulin (fasting, overnight)
When is gluconeogenesis more active?
short-term fasting
What is Ketogenesis?
produce ketones and ketoacids using fatty acidsas an alternative energy course when glucose is low for extended periods
When is Ketogenesis more active?
long-term fasting and starvation,
What is the primary cause of Type 1 Diabetes Mellitus (T1DM)?
Autoimmune destruction of insulin-producing beta cells in the pancreas leading to insulin deficiency, hyperglycemia, and need for exogenous insulin
What is the most common type of T1DM?
Immune-Mediated Type 1A
What is Immune-Mediated Type 1A?
β cell autoimmunity with genetic predisposition (HLA-DR, HLA-DQ) and autobodies present. More common in Kids/Young Adults, Scandinavian and European patients
What is Idiopathic Type 1B?
More rare form of T1DM without autoantibodies or genetic component. Has milder insulin deficiency. More common in African or Asian descent
What occurs in Stage 1 of Type 1 Diabetes?
Autoimmune β-cell destruction begins; ≥2 pancreatic autoantibodies present with normal glucose tolerance
What characterizes Stage 2 of Type 1 Diabetes?
Progressive β-cell loss and dysglycemia with abnormal glucose tolerance
What occurs in Stage 3 of Type 1 Diabetes?
Significant β-cell destruction causing insulin deficiency and overt hyperglycemia (symptomatic!)
What are the symptoms of Stage 4 Type 1 Diabetes?
Long-standing established T1DM with variable glycemic control and potential chronic complications.
What is the primary pathophysiology of Type 1 Diabetes?
1) Autoimmune destruction of pancreatic beta cells
2) Pancreatic alpha cells continue to secrete glucagon
3) Muscle, adipose, and hepatic cells can respond to insulin, but insulin is ABSENT
What are the classic signs and symptoms of hyperglycemia in children with T1DM?
Hyperglycemia and ketonemia leading to polyuria, polydipsia, polyphagia, and weight loss +/- polyphagia and blurred vision
At what glucose concentration does polyuria occur?
180 mg/dL
What diagnostic criteria indicates diabetes based on fasting plasma glucose?
≥126 mg/dL.
How do you distinguish Type 1 from Type 2 diabetes?
Pancreatic autoantibody testing and C-peptide
What is the c-peptide ratio in a patient producing their own insulin?
1:1 ratio; therefor, in T1DM C-peptide will be low
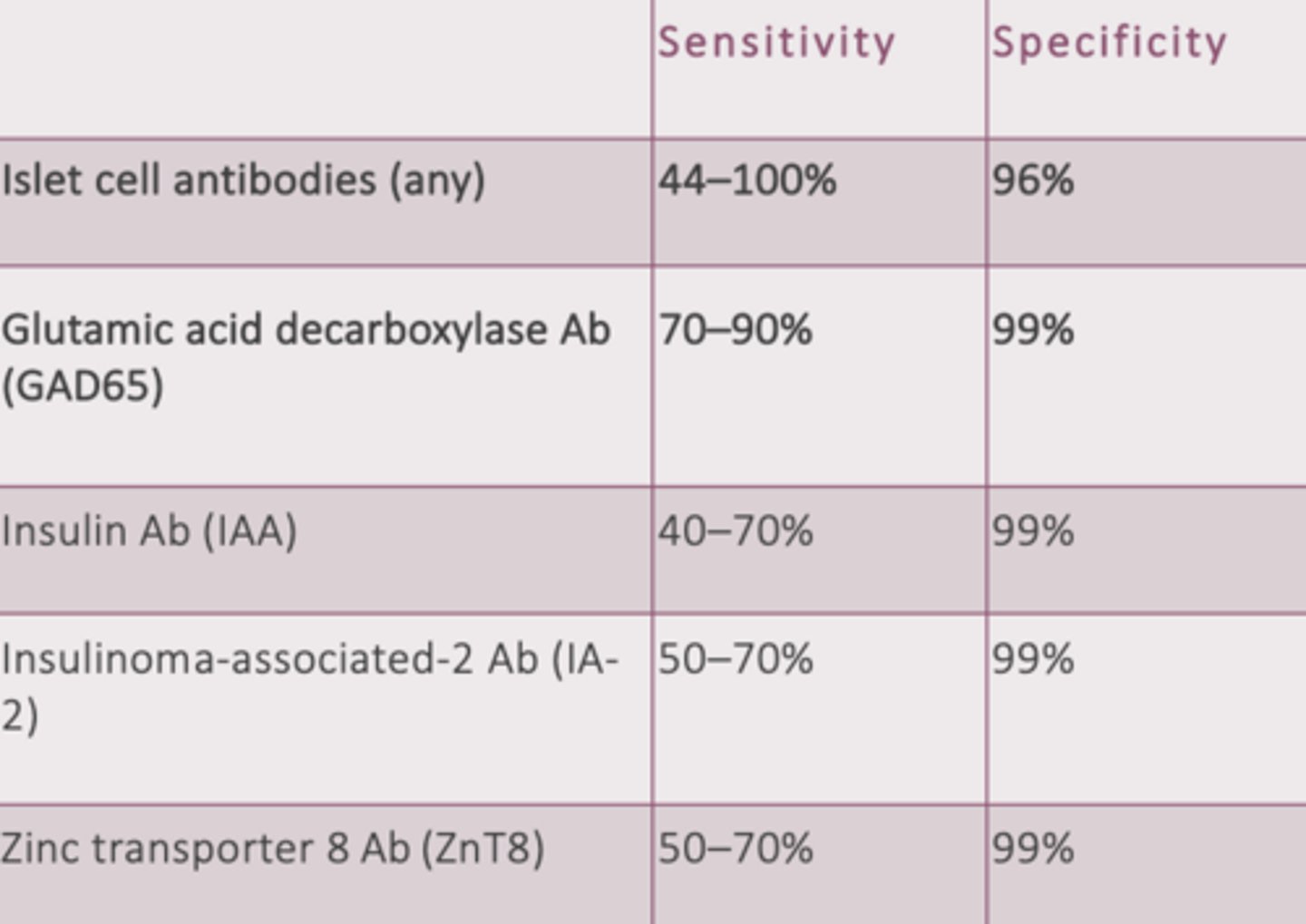
What autoantibodies are tested to distinguish Type 1 from Type 2 Diabetes?
GAD65 (MC), IA2, IAA (Ab targeting insulin), and ZnT8.
What are the characteristics of monogenic diabetes?
Caused by a single gene mutation in non-obese individuals with no autoantibodies present often presenting at a young age
What are the typical manifestations of monogenic diabetes?
1. Maturity onset diabetes of young (MODY); Develops ~25 years
2. Neonatal diabetes mellitus; first 6 months of life
What constitutes a "balanced diet" reccomended for T1DM?
complex carbohydrates balanced with protein, fat, and fiber
What is the recommended duration of aerobic activity for T1DM patients?
At least 30 minutes most days of the week (≥ 150 minutes/week).
What is the A1c goal for T1DM patients?
< 7.0%
How often should glucose be monitored in T1DM?
6-10 times per day preferably achieved with continuous glucose monitoring
What are the glucometer goals for T1DM patients?
80 to 130 mg/dL before meals, bedtime, overnight
What does "Time in Range" mean in continuous glucose monitoring?
the amount of time a patient's glucose is within the target range of 70 to 180 mg/dL; reasonable target for children is at least 70% of the day (17hrs/day)
What is the key understanding to the pharmacological management of T1DM?
It must be treated with insulin; no oral medication is effective
How often is basal insulin administered?
Daily or twice daily intermediate or long-acting insulin given via a continuous pump or subcutaneously
How often is prandial insulin administered?
Administer rapid-acting insulin during mealtimes with the dose determined by pre-meal glucose level and anticipated size of meal
What screening should be completed for complications of T1DM and how often should they be completed?
- Blood pressure (every visit!!)
- Lipids (q1-3 years)
- Retinopathy (q1-2 years)
- Neuropathy (annually)
- Nephropathy (annually)
When should screening being in T1DM diagnosis?
Retinopathy: 5 years after diagnosis or puberty for child diagnosis
Nephropathy: 5 years after diagnosis or ≥11/puberty in children
Neuropathy: 5 years after diagnosis
When should screening for PAD begin?
Age ≥65 years or diabetes duration ≥10 years, any end-organ damage, microvascular disease, or evidence of foot complications
What is the blood pressure goal of T1DM?
<130/80 achieved with ACEI or ARB
What are the LDL-C goals of T1DM?
Primary: <100 mg/dL
Secondary: <70 mg/dL
When is statin therapy reccomended in T1DM patients?
≥ 40 years old or younger with risk factors
What is the CAC goal for T1DM patients?
≥ 100
What is the Lipoprotein goal for T1DM patients?
> 50 mg/dL
How should an elevated UACR (>30 mg/g) be condired?
2 of 3 samples over a 6-month period
What is the treatment for diabetic neuropathy?
gabapentin, SNRIs, TCAs, or sodium channel blockers
What is the risk factor and presentation of Diabetic Gastroparesis?
longstanding DM (>10 years) resulting in nausea, vomiting, bloating, early satiety, upper abdominal discomfort, and constipation
How is Diabetic Gastroparesis diagnosed?
Upper endoscopy and nuclear gastric scintigraphy
What medication can be used for Diabetic Gastroparesis?
Metoclopramide (avoid GLP-1 as they slow gastric emptying)
What autoimmune comorbidities are associated with Type 1 Diabetes?
Thyroid disease, celiac disease, pernicious anemia, Addison's disease.
How often should screening for autoimmune comorbidities occur?
TSH: at least once, repeat as needed
Celiac: at least once; for children at diagnoses, 2 years then 5 years
Vitamin B12: at least once or neuropathy
Vitamin D: at least once
ALT/AST: at least once
Addison disease: unexplained hypoglycemia, electrolyte disturbance
What is the most common acute complication of T1DM?
Hypoglycemia
What glucose level indicated Level 1 Hypoglycemia?
<70 mg/dL
What glucose level indicated Level 2 Hypoglycemia?
<54 mg/dL
What is the "15-15" Rule of Level 1 and 2 Hypoglycemia?
1. Symptoms of hypoglycemia
2. Check blood sugar
3. Consume 15 grams of glucose (tablets preferred or Juice)
4. Recheck blood glucose in 15 minutes
5. If still 70 mg/dL, repeat 15 g glucose
What glucose level indicated Level 3 Hypoglycemia?
Any glucose level with altered mental/physical status requiring assistance of another person
What is the management of Level 3 Hypoglycemia?
1) Glucagon via SC, IM, or intranasally
2) IV dextrose (D50)
3) After acute symptoms resolve, 20 g of long-acting carbohydrate
What are the risk factors of hypoglycemia?
Longer diabetes duration, history of prior severe hypoglycemia, and Impaired awareness of hypoglycemia (IAH)
What are the autonomic symptoms of hypoglycemia?
palpitations, tachycardia, tremor, sweating, pallor, irritability, hunger, paresthesias
What are the CNS symptoms of hypoglycemia?
Headache, confusion, visual changes, weakness, LOC, seizure, dizziness
What is Impaired Awareness of Hypoglycemia (IAH)?
Dangerous condition where patients stop experiencing the warning signs (symptoms) of hypoglycemia
What are the causes of Impaired Awareness of Hypoglycemia (IAH)?
Recurrent hypoglycemia episodes, Sleep disturbance, Psychological stress, and Alcohol
What are the possible symptoms of Impaired Awareness of Hypoglycemia (IAH)?
Confusion, seizures, and coma
What is the Dawn Phenomenon?
Normal glucose until rise in serum glucose levels between 2am and 8am
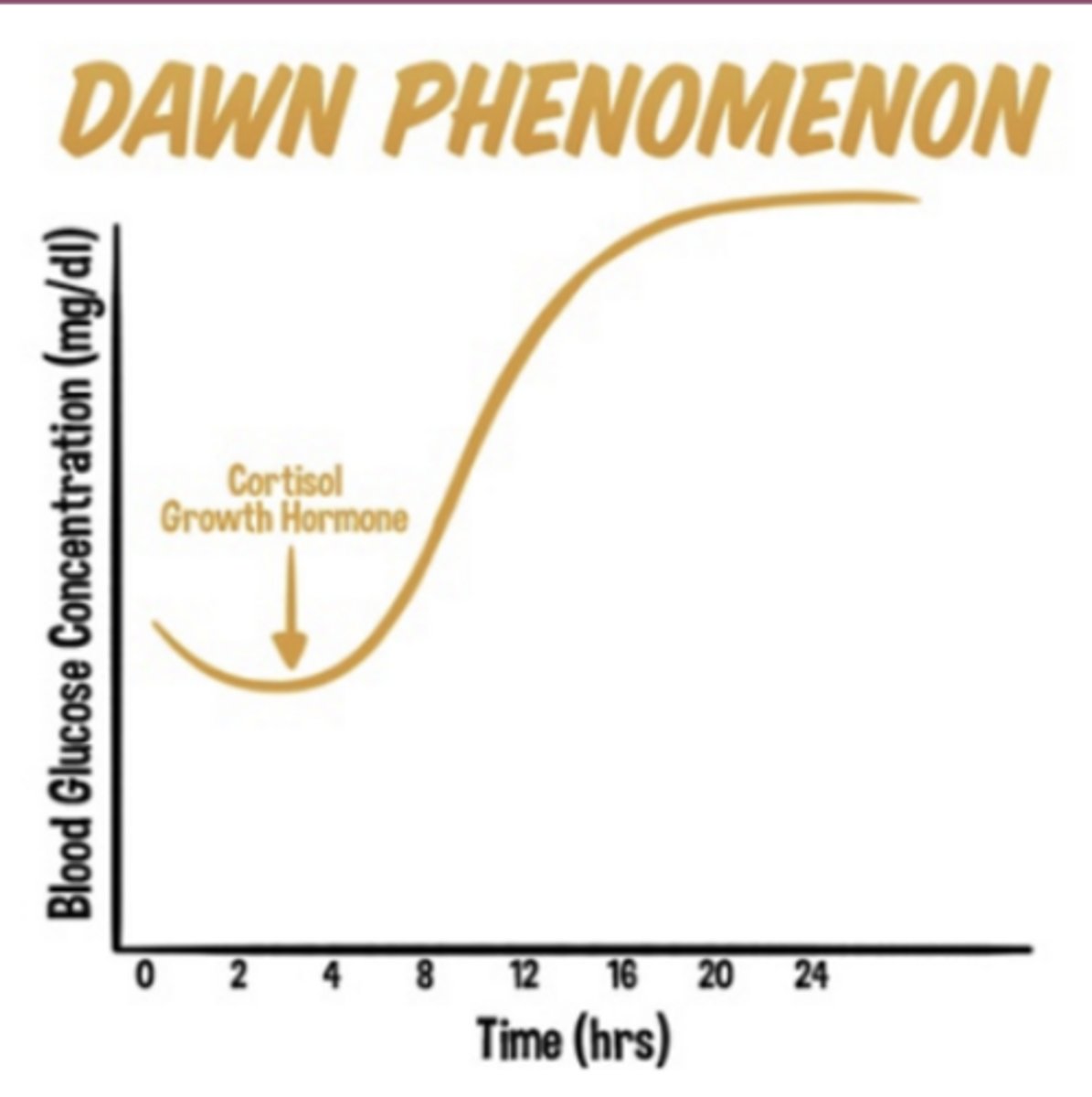
What management is recommended for the Dawn Phenomenon?
Increase overnight insulin delivery, avoid carbohydrates late at night, use insulin pump in the morning
What is the Somogyi Effect?
Nocturnal hypoglycemia followed by rebound hyperglycemia in the morning
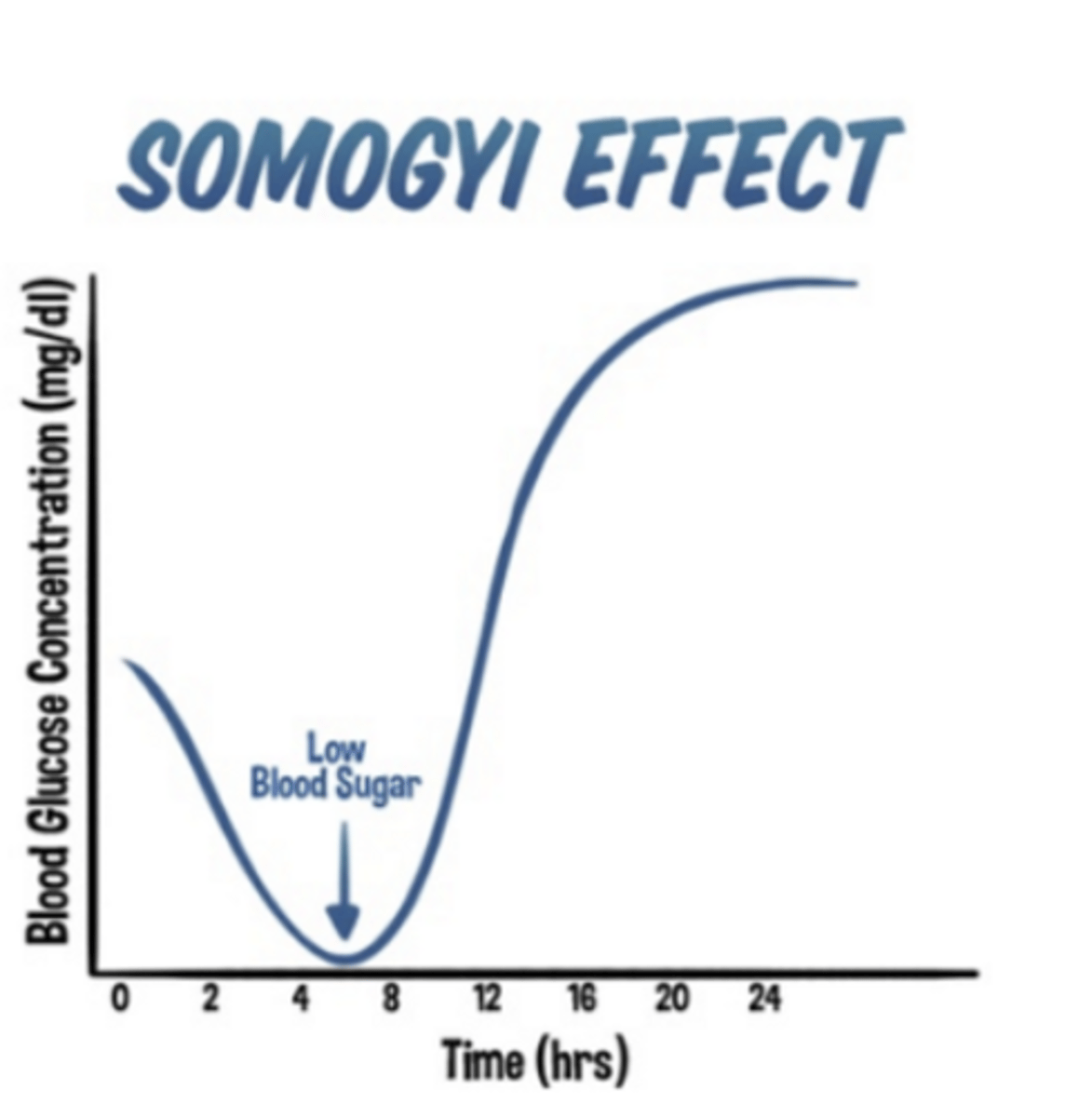
What management is recommended for the Somogyi Effect?
Decrease nighttime NPH dose or move it earlier and have a bedtime snack
What is Diabetic Ketoacidosis (DKA)?
a life-threatening condition resulting from severe insulin deficiency and increasing levels of counterregulatory hormones.
What are the metabolic pathway of DKA?
gluconeogenesis & glycogenolysis → ketogenesis → metabolic acidosis → glycosuria → osmotic water loss → potassium depletion
What is the triad of DKA?
Hyperglycemia, ketonemia, and metabolic acidosis.
What is the most common precipitator of DKA?
Insulin omission or noncompliance
What are other causes of DKA?
UTI, Pneumonia Inflammation (pancreatitis, cholecystitis), Infarction, Intoxication, and Medications (SLGT-2, steroids, and antipsychotics)
What are common symptoms of DKA?
polyuria, polydipsia, weight loss, fatigue, dyspnea, vomiting, abdominal pain, and polyphagia.
What are the signs of DKA?
Dehydration, Kussmaul respirations, ketonemia (fruity breath) and altered mental status.
What is the diagnostic criterion for DKA?
Glucose >250 mg/dL, anion gap, metabolic acidosis (pH <7.3 & Bicarb <18) and elevated Serum β-hydroxybutyrate (βOHB) or urine ketones
What is the anion gap in DKA?
>10 mEq/L.
What are the four pillars of DKA management?
Fluid resuscitation, insulin therapy, electrolyte replacement, and treatment of the precipitating cause.
What is the initial fluid resuscitation protocol for DKA?
1 L of 0.9% saline in the first hour, then 250-500 mL/hour based on volume status. Add dextrose when glucose reaches 250mg
What should be monitored before starting insulin therapy in DKA?
Potassium levels.
What should be done if K+ is <3.3 ?
Hold insulin and give 20–30 mEq K⁺/hr
What should be done if K+ is 3.3-5.3 ?
Add 20-30 mEq K⁺ to each liter of IV fluid
What should be done if K+ is >5.3 ?
Do not give K⁺; recheck every 2 hours
When is Bicarb considered to be given?
when pH < 6.9
What is the recommended insulin therapy for DKA?
IV regular insulin at 0.1 unit/kg/hr started immediately once potassium levels are normal
What is Euglycemic DKA?
DKA presenting with plasma glucose 200 mg/d in the presence of ketosis and metabolic acidosis
What can precipitate Euglycemic DKA?
SGLT-2 Inh (promotes glycosuria), reduced food intake, liver failure, and alcohol use
What is the anion gap metabolic acidosis in Euglycemic DKA?
pH <7.3 and bicarb <18
What are the symptoms of Euglycemic DKA?
Nausea, vomiting, malaise, and sometimes abdominal pain (similar to classic DKA)
What is the management of Euglycemic DKA?
Same protocol as classic DKA with IV fluids with dextrose (D5 or D10)
What is Hyperosmolar Hyperglycemic State (HHS)?
A serious, acute, and life-threatening hyperglycemic emergency occurring most often in in middle-aged and older adults with Type 2 diabetes
What is the defining clinical feature of HHS?
Profound hyperglycemia ( >600) without significant ketosis
What are the common precipitating factors for HHS?
Infection (MC), new-onset diabetes, nonadherence, acute illness, medication (corticosteroids, diuretics), and decreased water access
What is the clinical presentation of HHS?
Profound dehydration (8-12L deficit) and prominent neurologic manifestations with an insidious onset over days to weeks
What are the 3 cardinal biochemical features of HHS?
1. Severe hyperglycemia
2. Hyperosmolality
3. Absence of significant ketoacidosis
What is the initial lab workup for HHS?
Point-of-care glucose, CBC, CMP, serum osmolarity, ABG, serum ketones, CK, and A1c
What is the critical diagnostic value for effective serum osmolality in HHS?
≥ 320 mOsm/kg.
What is the standard sodium correction ratio?
1.6 mEq/L to measured Na⁺ for every 100 mg/dL glucose above 100 mg/dL (Katz formula)
What is the general step-wise managment of HHS?
1) Fluid Resuscitation
2) Insulin
3) Electrolytes
4) Thromboprophylaxis
What is the recommended fluid replacement for HHS?
1-1.5L NS over the first hour, with approximately 9L over 48 hours.
When should insulin be started in HHS?
Start after initial fluids once potassium is >3.3 (same as DKA)
What are common complications of HHS?
Thromboembolism, rhabdomyolysis, cerebral edema, and seizures.