cornea I microbial keratitis
1/31
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
32 Terms
what are the different types of microbial keratitis (3)
bacterial/fungal
viral
protozoal (Acanthamoeba Keratitis)
what is the aetiology of bacterial/fungal keratitis (4)
multiple bacteria/fungi that can cause it - common bacterial include:
Pseudomonas sp. (Gram -ve) - cause severe CL related infections
Staphylococcus sp. (Gram +ve)
Streptococcus sp. (Gram +ve)
gram + thicker cell walls which takes stain up better and gram - thinner walls - some treatments are more effective against gram+/gram -
common fungal:•Candida sp. (yeast-like)
•Fusarium sp. (filamentous)
•Aspergillus sp. (filamentous)
what are the predisposing/risk factors of bacterial/fungal keratitis (7)
•Ocular surface disease - dry eye, blepharitis, exposure keratopathy
•Lid margin infection - blepharitis, demodex, hordeolum
•Ocular trauma or surgery
•CL wear - esp. soft, extended wear lenses (poor hand/case hygiene)
•Immune compromise - weak
•Topical steroids - dampen inflammatory response
•Neurotrophic keratopathy (2° to HSV or diabetes) - reduced corneal sensation
what are the symptoms of bacterial/fungal keratitis (7)
•Usually unilateral
•Pain - moderate to severe and usually acute onset, rapid progression
•Redness
•Discharge
•Photophobia - sensitivity to light
•Blurred vision
•Awareness of white spot on cornea
what are the signs of bacterial/fungal keratitis (6)
•Lid oedema - swelling
•Epiphora - watery eyes
•Discharge (mucopurulent or purulent)
•Conjunctival hyperaemia - redness
•Corneal lesion - usually single (central or mid-peripheral) / excavation of epithelium (ulcer) - epithelium is missing / stromal infiltration/ stromal oedema (folds in Descemet membrane)
-Anterior chamber activity (flare, cells, hypopyon (visible layer of WBC (pus)))
what is the optometric management of bacterial/fungal keratitis (2)
•Same day referral to eye clinic - as it is a sight threatening condition
•Advise patients - STOP contact lens wear and take contact lenses and case to clinic for culture - identify what microbe is involved and what treatment would be most effective against this
explain the secondary care (1) for bacterial (4) and fungal keratitis (1)
corneal scrape & culture - small sample taken to investigate what microbes are involved and to determine what antibiotics would be effective
for bacterial infections:
antibiotics - (monotherapy/dual therapy, and systemic) e.g., levofloxacin, moxifloxacin, gentamicin hourly or ½ hourly
hospital admission - severe infections and/or compliance issues
cycloplegia - dilates iris and reduces ciliary spasm which is painful - reduces pain
topical steroids, once the infection is controlled
for fungal infections:
combined topical and oral therapy e.g. natamycin 5%, econazole 1%, oral voriconazole - longer course of treatment but rare
what is the aetiology of viral keratitis (3)
•Herpes simplex virus - HSV - very common - latent - leading cause of corneal blindness in the UK
•Herpes Zoster virus - HZO - affects 20-30% - previously chicken pox -
•Adenovirus - ADV
what are the predisposing factors of viral keratitis and specifically for HSV, HZO and ADV (5)
•Poor general health, immunodeficiency
•Steroids, immunosuppressants
•HSV: Previous ocular HSV - blepharonconjunctivits, keratitis, iridocyclitis, acute retinal necrosis
•HZO: Peak incidence 50-70 years old
•Adenovirus: Exposure to infection (highly infectious), upper respiratory tract infection
what are the symptoms of viral keratitis (6)
•Redness
•Watery
•Mild - moderate burning
•Variable levels of pain
•Photophobia
+/- Blurred vision
what are the signs of viral keratitis (4)
•Conjunctival hyperaemia - redness
•Epiphora/watery discharge
•Keratitis
•Ulcer
what is the optometric management of viral keratitis (1)
Sight-threatening (due to corneal involvement) - same day/emergency referral
what are the specific symptoms of Herpes Simplex Keratitis (3)
variable severity
Usually unilateral
Irritation - pain (NB: ↓corneal sensation)
what are the specific early (1) and late (2) signs of Herpes Simplex Keratitis
most commonly affects the epithelium
early signs:
coarse punctate (large, irregular dot like lesions) or stellate pattern (lesions are star shaped)
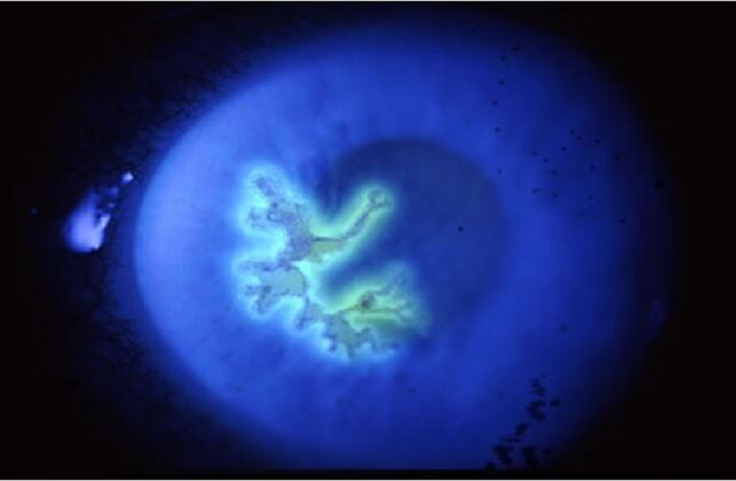
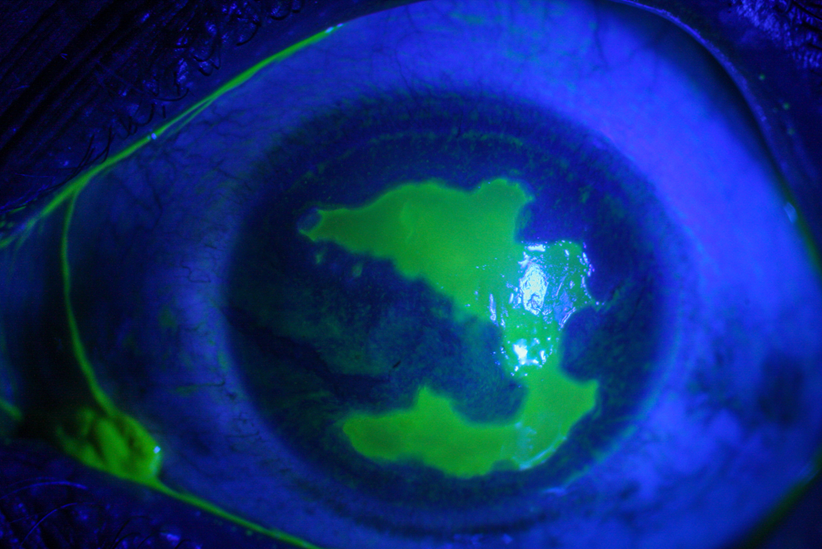
late signs:
Dendrite - characteristic branching pattern, stromal infiltrates
Geographic ulcer can follow (topical corticosteroids) - reduced corneal sensitivity - recurring - heals 1-2 weeks with scarring
what is the specific optometric management of herpes simplex keratitis (3)
•Stromal involvement - same day referral
•No stromal involvement - urgent referral (within one week) to ophthalmologist
•Dilate to exclude viral retinitis (same day referral)
what is the management by an ophthalmologist for Herpes Simplex Keratitis (3)
•Swab or biopsy - confirm the cause, guide appropriate treatment - for severe, uncertain and treatment resistant cases
•Antivirals - topical/systemic (Aciclovir 5 x daily for a week)
•Topical steroid AFTER initial treatment
what are the specific ocular symptoms of herpes zoster ophthalmicus (6)
•Discomfort
•Watery/sticky discharge
•Redness
•Pain
•Photophobia
+/- blurring

what are the general signs (systemic) of herpes zoster ophthalmicus (3)
•Pain and altered sensation of one side of forehead
•Vesicular rash affecting forehead/upper eyelid follows
•General malaise (unwell feeling), headache, fever

what are the ocular signs of herpes zoster ophthalmicus (7)
•Mucopurulent conjunctivitis (common - vesicles on lid margin)
•Keratitis - punctate epithelial → disciform (round/oval shaped) pseudodendrites
•Reduced corneal sensation
•Endothelial changes and keratic precipitates (inflammatory deposits on the corneal endothelium)
•Others: Uveitis, 20 glaucoma, episcleritis, scleritis, posterior segment involvement
•Complications can occur months or years after the acute phase
•Variable scope and severity

what are the skin related signs of herpes zoster ophthalmicus (3)
•Unilateral, painful, vesicular rash on forehead and upper eyelid
•Crusts in 2-3 weeks
•Hutchinson’s sign - lesion at tip of nose - indicates three times the usual risk of ocular complications - but these may also occur in one in three patients without the sign
what is the optometric management of Herpes zoster ophthalmicus (5)
•Urgent referral - systemic anti-viral treatment (< 72hrs) / if corneal involvement, anterior uveitis or elevated IOP
•Rest and general supportive measure (reassurance, support at home, good diet, plenty of fluids)
•Risk of infecting others with chickenpox - avoid elderly, pregnant women, people not previously exposed to VSV, immunodeficient px
•Topical lubricants (symptomatic relief)
•Systemic pain relief (paracetamol, ibuprofen)
what are the secondary care options for Herpes Zoster Ophthalmicus (4)
•Systemic antivirals (aciclovir)
•Topical anti-viral
•Topical steroids
•Treatment of complications
what are the specific signs of adenovirus (2)
•Punctate epithelial keratitis - sub-epithelial opacities over time
•Follicular conjunctivitis (upper & lower eyelids)
what is the management of adenovirus (5)
•Emergency referral if significant keratitis (pain and/or vision loss)
•Typically self-limiting
•advise on hygiene (i.e. don’t share towels)
•Antibiotics not effective
•Topical steroids controversial but may be given in some cases to reduce keratitis
what is the aetiology of Protozoal (Acanthamoeba) Keratitis (2)
•Acanthamoebae are ubiquitous free-living protozoans present in well water, drains, soil, dust and domestic tap water (tank)
rare but common in CL wearers
what are the predisposing/risk factors of Protozoal (Acanthamoeba) Keratitis (3)
•Soft contact lenses (extended wear)
•Poor contact lens hygiene - inadequate disinfection, use of non-sterile solutions, tap water rinsing of lenses and/or storage case, contamination of storage case with bacteria and fungi (± biofilm) which provide substrate for Acanthamoebae
•Contact with water - shower, swimming & using “hot tubs” especially with a corneal abrasion (scratch/loss of corneal epithelium) /if contact lenses in
what are the symptoms of Protozoal (Acanthamoeba) Keratitis (6)
•Pain (disproportionate to signs)
•Redness
•Watering
•Photophobia
•Loss of vision
•May be bilateral, may have a long history (misdiagnosis)

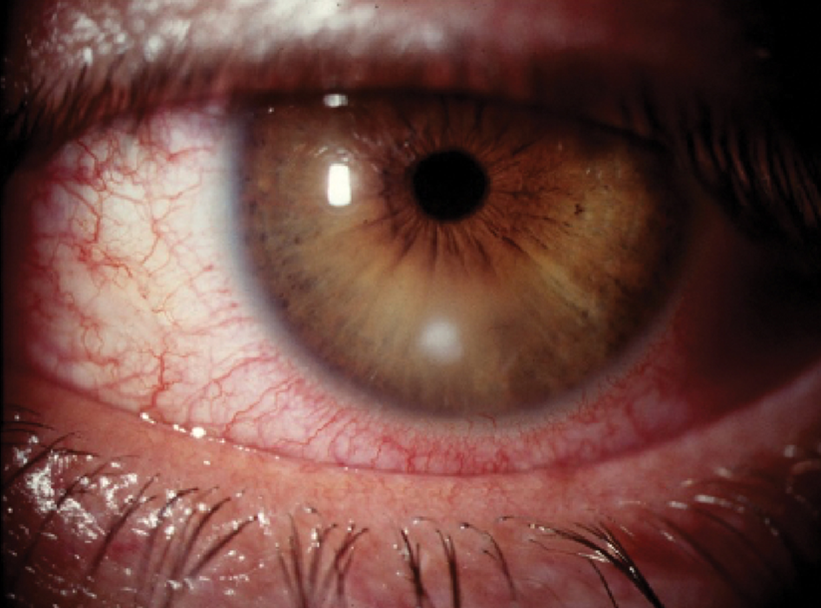
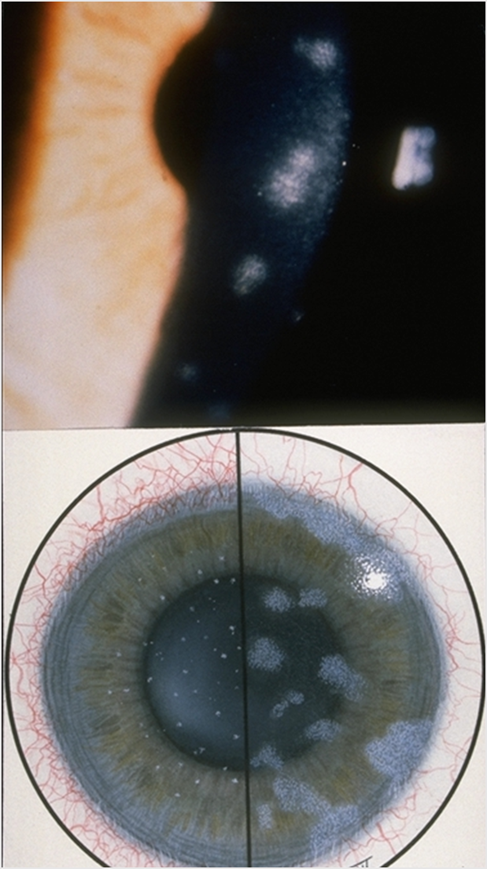
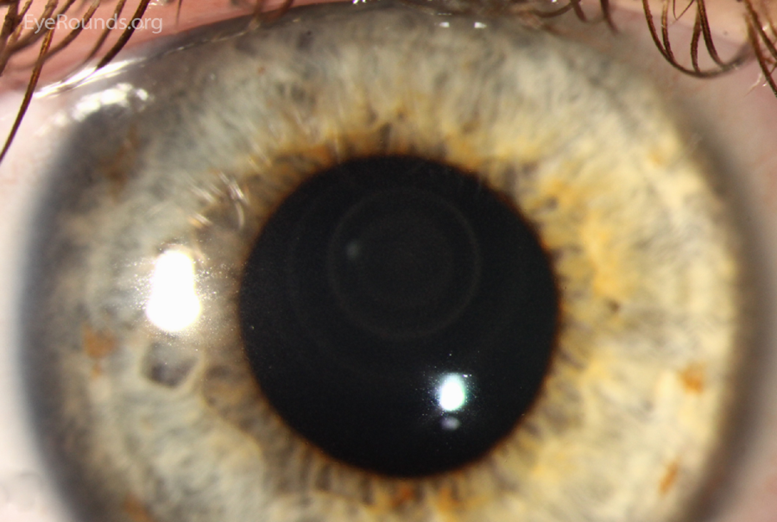
what are the early signs of Protozoal (Acanthamoeba) Keratitis (4)
•Epithelial/subepithelial infiltrates (localised collections of inflammatory cells in/under corneal epithelium)
•Pseudodendrites (corneal dendrite branch looking lesions)
•Radial keratoneuritis - inflammation of the corneal nerves that appear as radially oriented, linear, white opacities in the cornea - fine white lines radiating from the corneal center toward the periphery, following the path of corneal nerves
•Recurrent breakdown of corneal epithelium
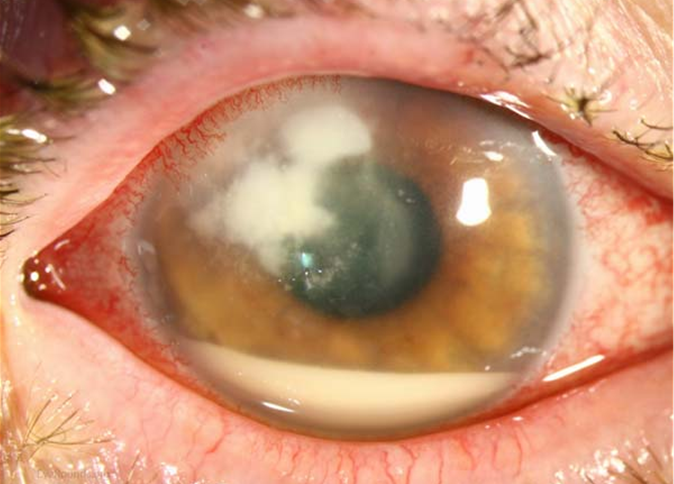
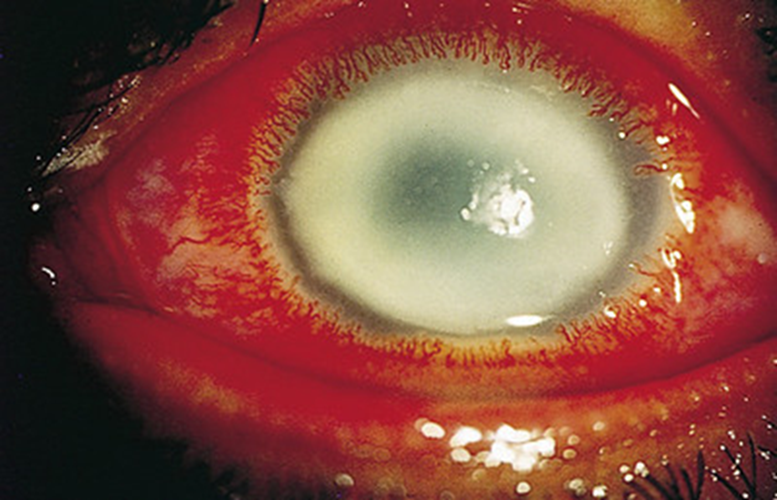
what are the later signs of Protozoal (Acanthamoeba) Keratitis (5)
•Deep corneal inflammation
•Central/paracentral ring-shaped infiltrate, disciform (round) infiltrate or abscess (localised collection of pus)
•Stromal thinning
•Anterior chamber activity - cells & flare, hypopyon, hyphema & 2° glaucoma
Scleritis (10% - poor prognosis)

what is the optometric management of Protozoal (Acanthamoeba) Keratitis (3)
•Stop all CL wear
•Refer as an emergency - same day to eye clinic
•Advise Px to take their contact lenses and case with them
what are the secondary care options of Protozoal (Acanthamoeba) Keratitis (3)
if unresponsive to antibiotics and steroids: Anti-oemebic drug - Dibromopropamidine, propramidine, neomycin + polyhexamethyl-biguanide (PHMB) - steroids later
Antibiotics for 2° infection
Lots of eye drops, longer term treatment (than for bacterial or viral keratitis)
case example of the evolution of Acanthamoeba Keratitis
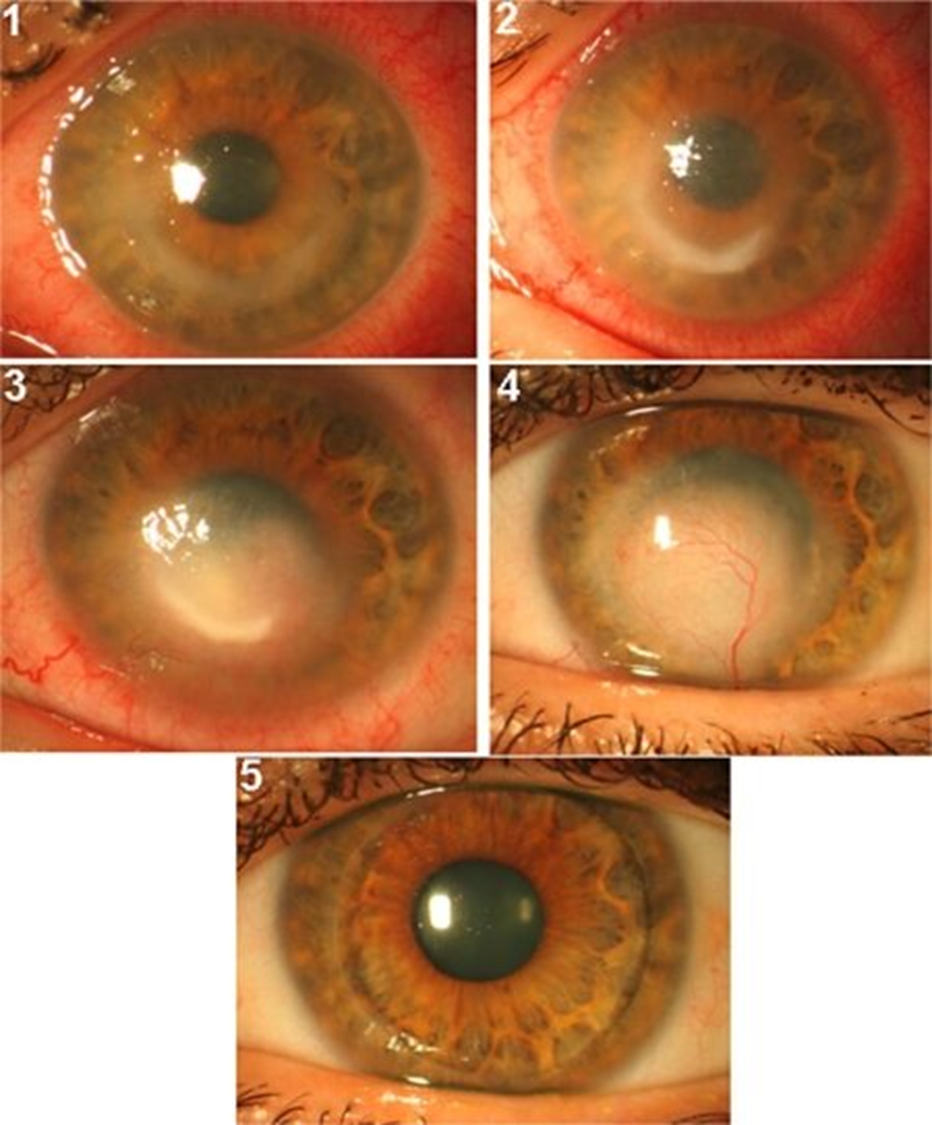
1: Cornea at the first visit - ring-shaped ulcer - typical sign
2: 3 months - no improvement on treatment - PHMB-desomedine every 1 hr.
3: Further 2 months - no signs of improvement after therapy switch to hexamidine and chlorhexidine every 1 h.
4: Further 4 months, the corneal ulcer finally receded, leaving a vascularized leucoma (white corneal opacity and scarring. Note that the conjunctival hyperaemia has also resolved.
5: Penetrating keratoplasty - corneal graft to remove scarring - with that blood vessel higher risk of treatment being rejected however would lead to vision loss so worth the risk for the patient