EMCAP and Major Hemorrhage
1/105
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
106 Terms
What is MARCHE?
a trauma care algorithm that prioritizes life-threatening injuries in a specific order
What does the “M” in MARCHE stand for?
massive hemorrhage
What does the “A” in MARCHE stand for?
airway
What does the “R” in MARCHE stand for?
respiratory
What does the “C” in MARCHE stand for?
circulation
What does the “H” in MARCHE stand for?
head injury and/or hypothermia
What does the “E” in MARCHE stand for?
everything else
How do we assess for a massive hemorrhage?
TCCC and/or raking (front and back) of body
How do we assess a patient’s respiratory functioning?
respiratory rate (RR)
work of breathing (WOB)
lung auscultations
injury assessments (pneumo or hemothorax, flail chest)
SpO2
How do we assess a patient’s circulation?
pulses
blood pressure
skin
level of alertness (LOA)
BITFT algorithm
bones & bleeds
IV access
TXA (tranexamic acid)
fluids
tourniquet reassessment
How do we assess a patient for hypothermia?
How can we assess for moderate to severe brain injury?
What does MPHATD in the everything else category stand for?
M — monitoring vitals
P — pain medications
H — head to toe
A — address all wounds
T — tactical evacuation prep (if not already done)
D — documentation (SBAT)
What are pulse sites?
areas where you can compress an artery against a bone
List the different types of pulses you can obtain from a patient.
temporal
carotid
apical
brachial
radial
femoral
popliteal
posterior tibial
dorsalis pedis
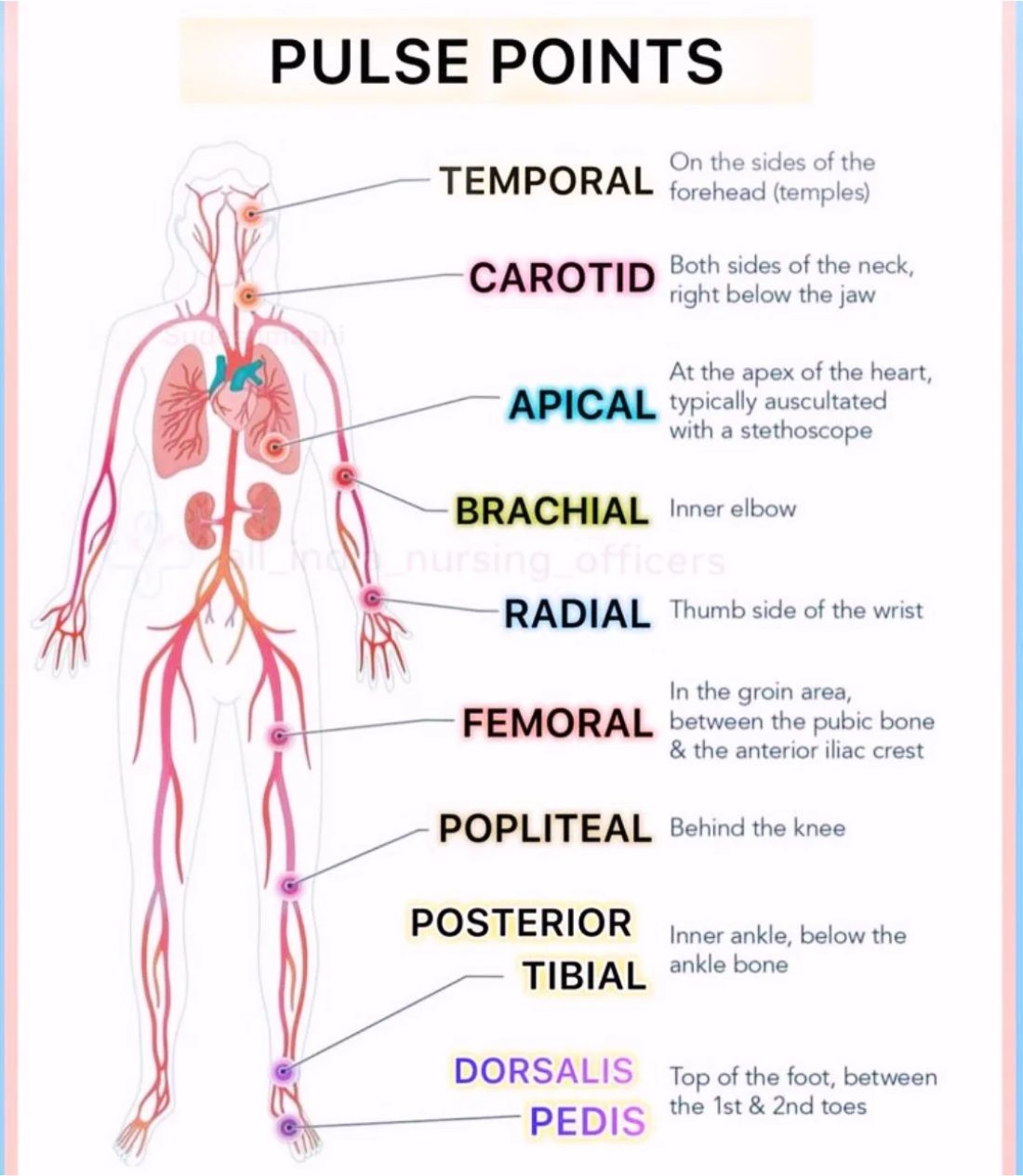
Where is the temporal pulse point?
temples (sides of forehead)

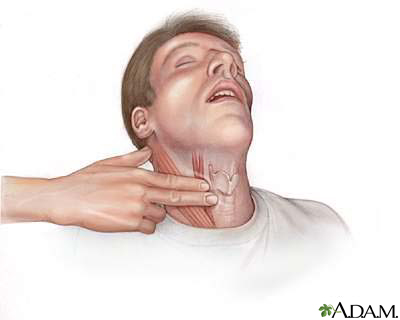
Where is the carotid pulse point?
both sides of the neck, right below the jaw
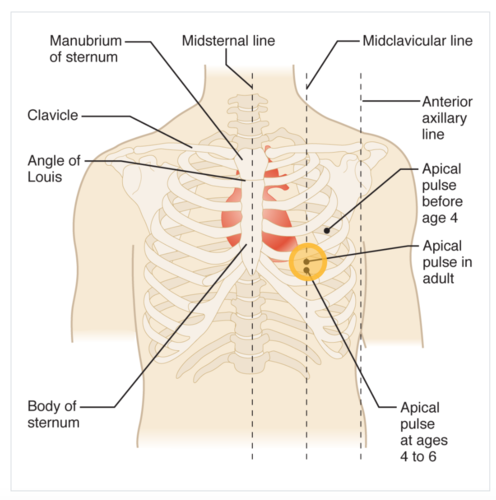
Where is the apical pulse point?
apex of the heart (L side of the chest at the 5th intercostal space at the midclavicular line; bottom of the heart)
Where is the brachial pulse point?
inner elbow

Where is the radial pulse point?
thumb side of the wrist

Where is the femoral pulse point?
groin area between the pubic bone and the anterior iliac crest

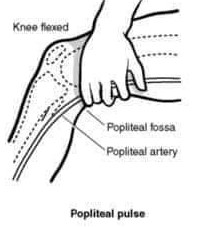
Where is the popliteal pulse point
behind the knee
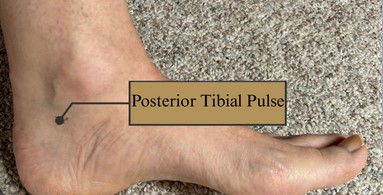
Where is the posterior tibial pulse point?
inner ankle, below the ankle bone
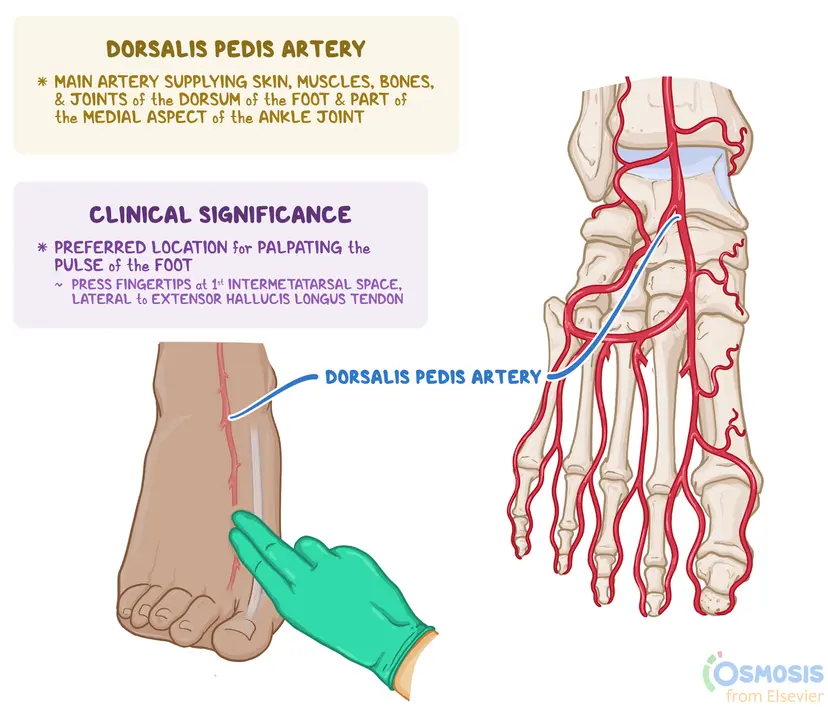
Where is the dorsalis pedis pulse point?
top of the foot between the first and second toes
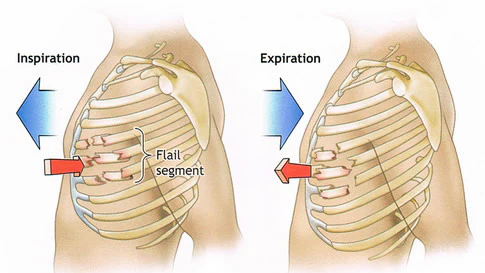
How is flail chest determined?
palpate for sternum stability
observe for paradoxical chest wall motion (flail chest segment)
observe for chest wall deformity
What are the different levels of respiratory distress?
mild
moderate
severe
(ventilatory) failure
What are the different levels of oxygenation compromise?
mild
moderate
severe
(oxygenation) failure
What is EMCAP?
mnemonic for scene assessment (to ensure safety and gather pertinent information)
What does the “E” in EMCAP stand for?
environment
What does the “M” in EMCAP stand for?
mechanism of injury (MOI)
What does the “C” in EMCAP stand for?
casualty count
What does the “A” in EMCAP stand for?
allied agencies
What does the “P” in EMCAP stand for?
PPE
What are the six parts of a scene approach?
introduce self and get name and age of patient
obtain chief complaint
FREI
clinical findings
peripheral perfusion
work of breathing
brain perfusion
pulse(s)
determine sick or less sick (and start CPR if no pulse)
delegation to your partner
4 lead ECG
blood pressure
SpO2
respiratory rate (RR)
“notify me of any abnormal findings immediately”
note: ensure all other relevant vitals are gathered by end of primary (will depend on patient’s presentation)
What is the first part of a scene approach?
introduce yourself (name, profession)
obtain name and age of patient
What is the second part of a scene approach?
obtain chief complaint
What is the third part of a scene approach?
FREI screening
What is the fourth part of a scene approach?
clinical findings
peripheral perfusion
work of breathing
brain perfusion
pulse(s)
What is the fifth part of a scene approach?
determine sick or less sick (and start CPR if no pulse)
What is the sixth part of a scene approach?
delegation to your partner
4 lead ECG
blood pressure
SpO2
respiratory rate (RR)
“notify me of any abnormal findings immediately”
What vitals must be collected during your primary assessment?
HR
BP
RR
SpO2
ETCO2
pupils
temp
4 or 12 lead ECG
GCS
BGL
What are some common hazards present at scenes?
fire/smoke
air pollutants/chemicals
weather
water
vehicles
crimes/assailants/weapons
animals
bio-hazards
bystanders
Why does the MOI matter?
helps predict:
likely injury patterns
severity
required resources
extrication
ACP
trauma centres
What does MOI stand for?
mechanism of injury
What is translational energy?
injures caused by rapid, linear acceleration (or deceleration) forces
body moves along a straight line (translates) rather than rotating
hallmark of high-energy impact (MVCs, falls, etc.)
severe shearing, stretching, or tearing of tissues
high risk of spinal cord injuries (SMR)
high risk of aortic ruptures
TAI
What is a traumatic axonal injury (TAI)?
severe form of brain injury caused by shearing forces that damage nerve fibres
widespread white matter damage caused by rapid acceleration/deceleration
What is rotational energy?
falls or spins leading to twisting forces
What is crush/compression energy?
forces applied over time + area
What must you do regarding identifying hazards during your assessment?
also mention mitigation of the hazard(s), not enough to simply identify the hazard
Why is PPE not considered a mitigation for hazards?
it’s an article of defense (a buffer), not a means of mitigation
e.g., you don’t mitigate traffic hazards by wearing a helmet
What could be a hint to the severity of a call within the calls details, and how can this be applied in the EMCAP?
trauma triage guideline
spinal motion restriction standard
“call details mentioned rollover and ejection, so this patient is likely to meet my trauma bypass and spinal motion restriction (SMR)”
What are deceleration injuries?
rapid loss of velocity —> when the body stops suddenly, organs continue moving at the original velocity until they either:
1) hit something or,
2) tear away from whatever was holding/anchoring them
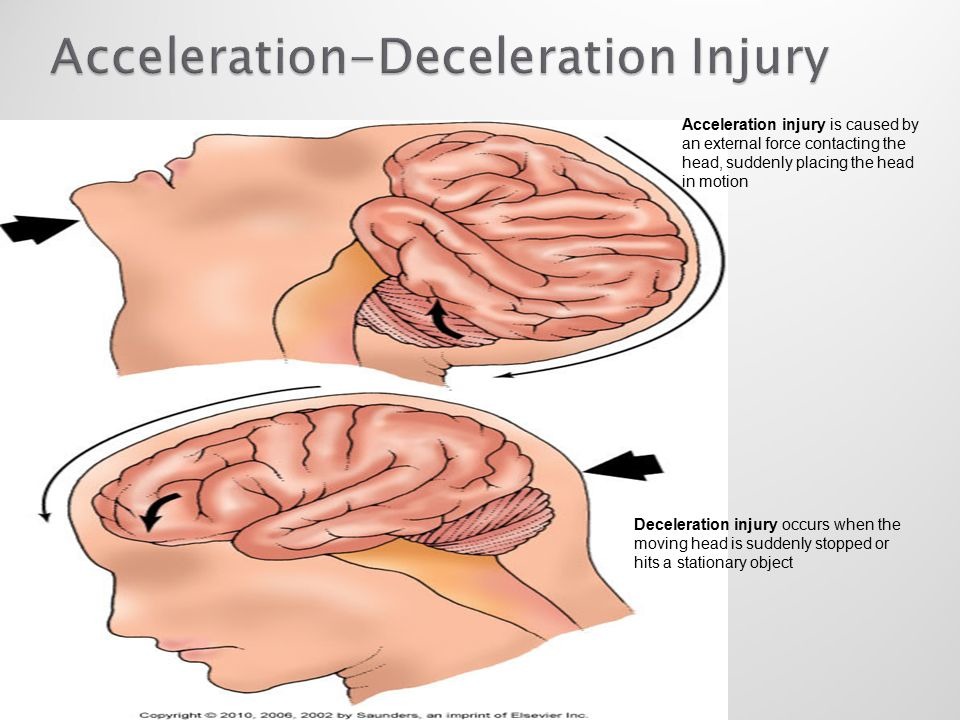
What are acceleration injuries?
What are contact precautions?
long sleeve gown
gloves
dedicate equipment to patient (or disinfect thoroughly before use with another)
What are droplet precautions?
long sleeve gown
gloves
dedicate equipment to patient (or disinfect thoroughly before use with another)
mask
eye protection
What are airbourne precautions?
droplet precautions + N95 mask
What illnesses require droplet precautions?
pertussis (whooping cough)
meningococcal disease
RSV
influenza
parainfluenza
GAS (skin, wound, invasive)
What illnesses require airbourne precautions?
tuberculosis
measles (rubeola)
chickenpox
shingles
What illnesses require contact precautions?
RSV
influenze
parainfluenza
GAS (skin, wound, invasive)
ESBL
MRSA
VRE
clostridium difficile (c-diff)
norovirus
What is a FREI screening?
dispatch gives you an initial screening
new (or worsening cough)
fever/shakes/chills over last 24 hours
headache, sore throat, muscle pain, abdominal pain, vomiting, or diarrhea
must confirm upon patient contact, and adjust PPE accordingly
What is CLAPS-D?
looking for:
C
contusions
contaminations
L
lacerations
A
abrasions
P
punctures
penetrations
protrusions
S
swelling
D
dried blood
diaphoresis
deformities
What is TICS-D?
feeling for:
T
tenderness
I
instability
C
crepitus
S
swelling
D
deformities
How do we collect clinical findings?
looking
listening
feeling
What are we looking for when assessing peripheral perfusion during our approach?
paleness
mottling
cyanosis
What are we looking for when assessing work of breathing during our approach?
relaxed breaths
laboured breaths
absent
sounds
What are we looking for when assessing brain perfusion during our approach?
A - alert (*4)
V - verbal (*3)
P - painful (*2)
U - unresponsive (*1)
How are the AVPU brain perfusion check and the GCS related?
AVPU (alert, verbal, pain, unresponsive) = eye section of GCS assessment
What is the purpose of a primary exam?
to find
life
limb
function
threats and indicate the appropriate interventions
What is a bradycardic heart rate?
<50 bpm
What is a tachycardic heart rate?
>100 bpm
How is heart rate calculated?
counting how many beats are felt over 1 minute
# of beats in 10 seconds x 6
# of beats in 15 seconds x 4
What are we assessing when taking heart rate?
rate
rhythm
strength
How is respiratory rate calculated?
counting how many respirations are seen over 1 minute
# of respirations in 10 seconds x 6
# of respirations in 15 seconds x 4
What is the RR range for bradypnea?
<10 breaths per min
What is the RR range for tachypnea?
>28 breaths per min
What are we assessing when taking respiratory rate?
rate
effort
depth
pattern
What is systolic blood pressure?
top number
pressure in arteries when heart contracts
reflects cardiac output
reflects force of contraction
What is diastolic blood pressure?
bottom number
pressure in the arteries when the heart relaxes
reflects vascular tone (systemic vascular resistance)
What can a decrease in systolic blood pressure indicate?
hypovolemia
pump problems
What can a decrease in diastolic blood pressure indicate?
sepsis
loss of vascular tone (spinal shock)
severe vasodilation (anaphylaxis)
What is mean arterial pressure (MAP)?
MAP = DBP + ⅓(SBP-DBP)
low readings indicate potential organ failure
target MAP for organs is >65 mmHg
What is a fistula?
surgically created connections between an artery and a vein → provides access to the blood stream for hemodialysis
Why should blood pressure not be taken on the same side of the body as a patient’s masectomy?
lymphnodes are surgically removed during masectomies → taking blood pressure on that side can cause lymphedema since there are no lymph nodes to help with drainage
What is PERRLA?
Pupils Equal, Round, and Reactive to Light and Accommodation
What causes hemorrhagic shock?
rapid blood loss (internal and/or external) leading to inadequate perfusion of tissues and organs
blood volume drops → less oxygen delivery → tissues starve → organ failure → death
In regards to energy transfer, what do we see happen to air-filled tissue (lungs, bowel) during trauma?
tear easily
In regards to energy transfer, what do we see happen to solid organs (liver, spleen) during trauma?
rupture when sheared or compressed
In regards to energy transfer, what do we see happen to bone during trauma?
handles compression well but fails under bending and twisting
In regards to energy transfer, what do we see happen to vascular structures (arteries, veins) during trauma?
fail under sudden stretch
What do high-speed collisions do to the body?
car stops → body keeps moving → body eventually stops → organs keep moving → organs slam into cavity walls → multiple impacts → many layers of damage (complex systemic trauma)
What are compression injuries?
when force is applied directly to tissue, crushing it between two surfaces (e.g., chest vs. steering wheel, abdomen vs. lap belt, head vs. windshield)
In regards to MOI, what 4 questions should be asked?
what energy was involved?
how did the body decelerate?
what was compressed?
what can be anticipated to occur next given this information?
“What energy was involved” concerns which factors of MOI?
velocity
height
mass
surface
“How did the body decelerate” concerns which factors of MOI?
instant stop
gradual
multiple impacts
What are some things that could be anticipated to happen in a patient from only knowing the MOI?
stabbing → internal hemorrhage
high-speed collision → organ rupture
fall from greater than 2m → spinal injury
electrocuted → enter and exit spots of electrical current
How should amputated/avulsed parts be handled?
preserve all amputated tissue
if contaminated → gently rinse with saline
wrap/cover exposed end with moist, sterile dressing
place in suitable water-tight container/plastic bag + immerse in cold water
When should a wound be packed?
When should a tourniquet be used to stop a deadly bleed?
What should be done if a deadly wound is located in a hollow space of the skull, chest, or abdomen?
What are common errors seen with tourniquet use?
not tight enough
placed over clothes/objects
placed too low
stopping when patient screams
not re-assessing for re-bleeding
forgetting to document the time