Neuro Lab Practical Final
1/93
Earn XP
Description and Tags
Covers vestibular, stroke, TBI, MS
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
94 Terms
What patient populations are tested in the Neuro practical?
1 scenario for Vestibular and 1 skill for Stroke, TBI or MS
What is vestibular functioning primarily related to?
The Vestibulo-Ocular Reflex (VOR)
It is a reflex that stabilizes vision during rapid head movements by producing eye movements in the opposite direction of the head motion, ensuring a steady, clear image. Essentially Its job is to keep your eyes fixed on a target while your head is moving.
What does the VOR help identify?
Vestibular imbalance
How does a patient with vestibular hypofunction present?
Main complaint: dizziness, difficulty in visually busy environments (grocery store), and difficulty when driving (In the car while environment is moving)
What MUST be done before ANY vestibular testing?
Clear the cervical spine!
Unsure if they expect us to clear the cervical spine or simply state that you would.
What are the examinations for vestibular hypofunctioning? (Just name them first)
Head thrust impulse test
Dynamic vision acuity (NOT ON PRATICAL ACCORDING TO ALVAREZ)
Head shaking nystagmus
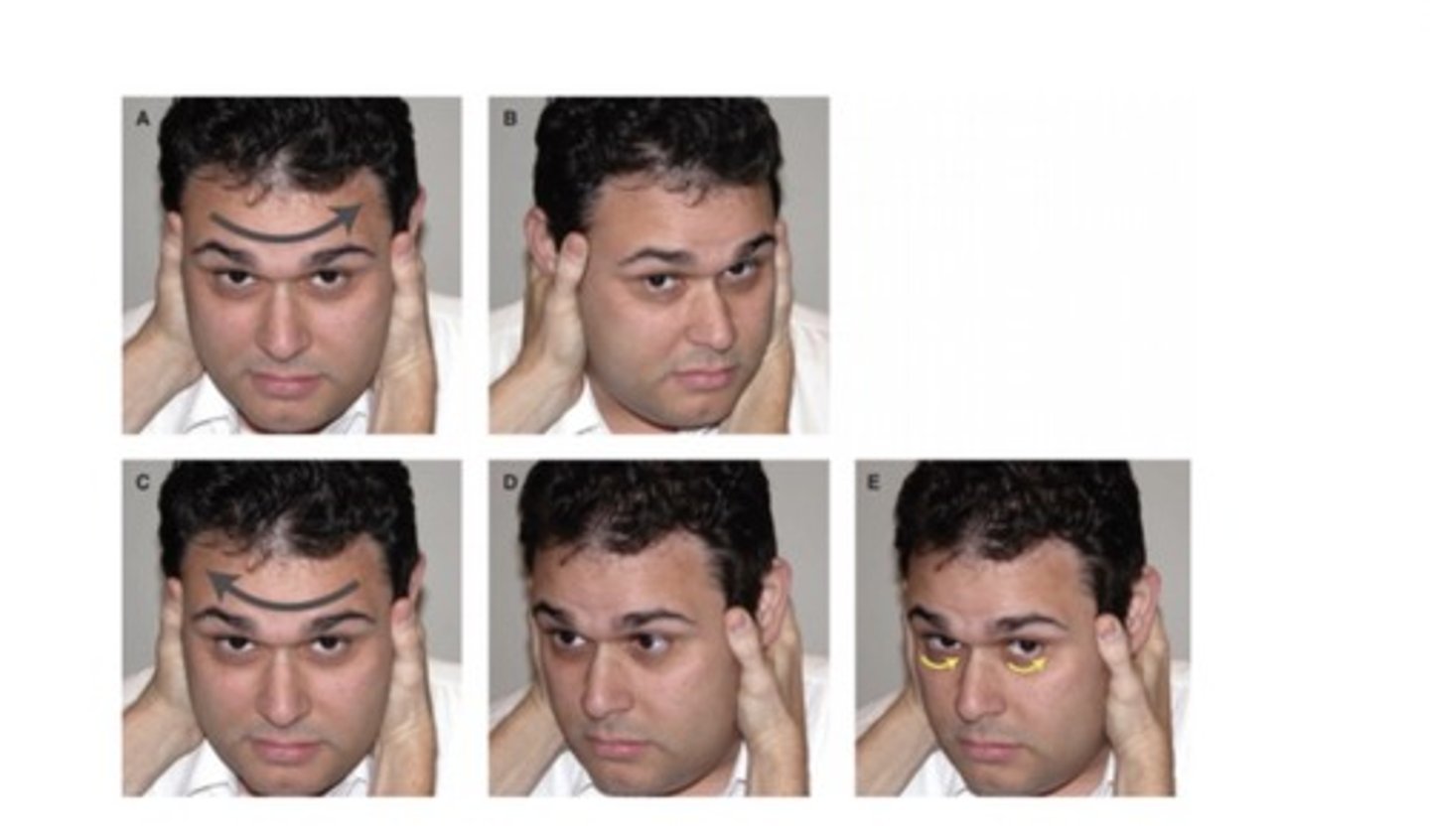
How do you perform the Head Thrust Test?
CLEAR CERVICAL SPINE FIRST
Patient seated upright, hold their head and you flex their head flexed 15-20°, patient fixates on your nose. Now rapidly rotate head 10-20° to one side, return to center, repeat other side.
Important to not just start with the rapid turns, do a couple slower ones before then randomly throw in a thrust one direction, then repeat the process for the other side.
What are you testing in the Head Thrust Test?
Vestibulo-Ocular Reflex (VOR) → ability to maintain gaze with head movement
What is a positive Head Thrust Test?
Corrective saccade
What does a corrective saccade indicate?
VOR disruption → vestibular hypofunction
A positive Head Thrust correlates to which side?
The side the head was rotated toward
What does the Head Thrust Test help diagnose?
Peripheral vestibular system problem such as vestibular hypofunctioning
How do you perform the Dynamic Visual Acuity Test? (NOT ON PRATICAL ACCORDING TO ALAVAREZ, but i would still know how to do it/what it test for just in case they ask)
CLEAR CERVICAL SPINE FIRST
Patient sits 2-4 meters from ETDRS chart, and ask them to read the lowest possible letter on the eye chart (this test static acuity first).
After doing this, ask the patient to do it again but this time rotate head side-to-side. The rotations should be 30 degrees total and the frequency aka the speed of the movement is 2 hz or 2 cycles a second (this test dynamic acuity)
What are you comparing in DVA?
VOR, comparing static (baseline reading no rotations) vs dynamic visual acuity (with rotations)
What is a positive DVA test?
A change of ≥ 3 lines
What does a positive DVA indicate?
Peripheral vestibular system problem such as vestibular hypofunctioning
How do you perform the Head Shaking Nystagmus Test?
CLEAR CERVICAL SPINE FIRST
Patient seated, head flexed 30°, eyes closed. Once in this position, shake head 20 times (One cycle = 1 shake) or 20 seconds at 2 Hz.
Once done shaking, tell pt to open their eyes and observe for nystagmus (rapid eye beating)
NOTE: For nystagmus, you don’t want the pt to focus their eye sight directly on anything as that might mask the nystagmus. So DO NOT tell them to focus on your nose
What are you testing in Head Shaking Nystagmus?
Vestibulo-Ocular Reflex
What is a positive finding in Head Shaking Nystagmus?
More than 3 beats of nystagmus
In vestibular imbalance, where does the fast phase of nystagmus go?
Toward the UNINVOLVED side
You name it by the fast phase, no the slow drift. Nystagmus usually beats away from the damaged side. For example lets say you see the eyes slowly drift to their left, then quickly snap to their right, that is right beating nystagmus, meaning there is left peripheral vestibular hypofunctioning
What does the Head Shaking Nystagmus Test help diagnose?
Peripheral vestibular system problem such as vestibular hypofunctioning/vestibular imbalance
Lets say you perform these test on your patient and they are positive meaning they have vestibular hypofunctioning. What are the interventions/treatment you can have them do to correct this issue? (Just name them right now)
Gaze stability/adaptation X1
Gaze stability/adaptation X2
How do you perform X1 gaze stability exercises?
Patient seated, holds out card with target on it (typically an X mark), and tell the pt to keep their eyes on the target/X mark
Now have the pt perform head rotations side to side for 1-2 minutes, taking 1-2 minutes of rest between sets or until the symptoms subside
What is the duration and frequency of X1 exercises?
1-2 minutes per set, 3x/day, total: 3-5 min/session
How do you progress X1 exercises?
Increase head speed (while target remains clear), walk while doing the exercises, or use a busy background
What is the goal of X1 exercises?
1-2 minutes per set, 3x/day, total: 3-5 min/session
Adaptation is when you stop right before symptoms are provoked, habituation is purposely having the pt’s symptoms provokes in order for their “threshold” to increase.
Think of it like a threshold, adaptation works right underneath the threshold and habituation works past the threshold.
How do you perform X2 exercises?
Patient seated, holds out card with target on it (typically an X mark), and tell the pt to keep their eyes on the target/X mark
Now have the pt perform head rotations side to side AND have them move the card the opposite way of the direction of rotation. Perform for 1-2 minutes, taking 1-2 minutes of rest between sets or until the symptoms subside
What is the duration and frequency of X2 exercises?
1-2 minutes per set, 3x/day, total: 3-5 min/session
How do you progress X1 exercises?
Increase head speed (while target remains clear), walk while doing the exercises, or use a busy background
What is the goal of X2 exercises?
Adaptation (stopping before dizziness) to stimulus
What does BPPV stand for?
Benign Paroxysmal Positional Vertigo
Paroxysmal (sudden onset of symptoms)
positional (head position provokes stimulus)
What type of disorder is BPPV? What does it cause?
Peripheral vestibular disorder
Causes acute onset of vertigo and nystagmus
What causes BPPV?
Otoconia crystal displacement (canal or cupula)
Cupula is more severe
What is the MOST common sign of BPPV?
Vertigo ("room spinning")
What triggers BPPV symptoms?
Head movements, neck movements, or overall positional changes. Common triggers are:
Rolling in bed, looking up/down, supine to sit and vise versa, and leaning forward.
What is the duration of BPPV symptoms?
Seconds to minutes
What is the main complaint in BPPV?
"The room is spinning"
What does the Dix-Hallpike test diagnose?
Posterior & anterior canal BPPV
How do you perform Dix-Hallpike?
Start long sitting, head turned 45° toward affected side, quickly bring patient back, head in 30° extension, hold 60 sec.
What is a positive Dix-Hallpike?
Torsional + beating nystagmus
What does upbeating nystagmus indicate?
Posterior canal BPPV
What does downbeating nystagmus indicate?
Anterior canal BPPV
What does nystagmus < 60 sec indicate?
Canalithiasis (free-floating crystals)
What does nystagmus > 60 sec indicate?
Cupulolithiasis (crystals stuck)
How do you perform the Supine Roll Test?
Patient supine, head in 20° flexion, quickly rotate head 90° to one side, hold up to 1 minute or until symptoms stop, return to neutral, repeat on other side.
What are the positive findings and interpretation of the Supine Roll Test?
Positive: Horizontal nystagmus; Interpretation: < 60 sec → Canalithiasis, > 60 sec → Cupulolithiasis, Direction: Geotropic → toward ground, Ageotropic → toward sky.
What is the Epley Maneuver used for and how does it start?
Used for: Posterior canal BPPV (canalithiasis); Start: Dix-Hallpike toward affected side, hold until vertigo + nystagmus stop.
What is the full sequence of the Epley Maneuver after the starting position?
Rotate head to unaffected side → hold, roll patient onto side (head 45° toward ground) → hold ~1 min, bring patient to sitting → maintain position until symptoms resolve.
What is the Semont maneuver used for and what is the setup?
Used for: Posterior canal cupulolithiasis; Setup: Patient seated, head turned 45° to UNAFFECTED side.
What is the movement sequence of the Semont maneuver?
Quickly move to affected side-lying → hold 1-2 min, rapidly move to opposite side-lying (face toward mat) → hold 1-2 min, return to sitting.
What is the Lempert (BBQ Roll) maneuver used for and what is the starting position?
Used for: Horizontal canal BPPV; Start: Supine, head turned toward affected side (90°).
What is the full rolling sequence of the Lempert maneuver?
Affected side → hold, neutral → hold, unaffected side → hold, prone (neck flexed 20°) → hold, continue until sitting.
What is the purpose of Brandt-Daroff exercises?
Used for chronic BPPV (canalithiasis), works via habituation.
What is the goal of AFO/ACE wrapping at the ankle?
Dorsiflexion + eversion, improve swing phase clearance.
How do you apply ACE wrap for foot drop?
Start at met heads, wrap lateral → medial, go up leg, anchor behind knee, wrap back down and secure.
What is the goal of theraband wrapping at the hip/knee?
Promote knee flexion + DF in swing, provide flexor moment.
How do you apply theraband for knee flexion?
Band under forefoot, cross in X pattern at knee, attach to gait belt.
What is the purpose of the ACE wrap lab station and the appropriate patient type?
Purpose: DF + knee flexion; Appropriate for: Foot drop, Stroke, TBI, Weakness.
What are other interventions for foot drop?
Theraband (propulsion), AFO, FES, ACE wrap.
What are the weakness patterns in neuro patients?
TBI → bilateral, Stroke → hemiparesis, MS → generalized weakness.
Where do you stand during gait training?
Unilateral → weak side, Bilateral → behind patient.
What is the purpose of gait training?
Drive the afferent nervous system, promote weight bearing for recovery.
Where should a cane be placed during gait training?
Strong side, therapist pulls patient toward weak side.
What is the most important concept for sit-to-stand in neuro patients?
Nose over toes.
How do you facilitate sit-to-stand and stand-to-sit?
Sit → stand: assist knee extension; Stand → sit: web space at groin for hip hinge, hand on back for forward cue.
What is the full setup for sit-to-stand training?
Strong side near support, weak side with therapist, therapist assists knee and trunk alignment.
What are the key goals during transfer training?
Prevent buckling, avoid excessive turning, maintain control.
What is Transfer Option 1 — setup and movement?
Transfer toward strong side, block weak knee, stand-step or pivot to chair.
How do you return a patient to bed?
Transfer toward weak side with proper blocking.
How do you control descent into sitting?
Web space at groin for hip flexion, hand on back for forward cue.
What is Transfer Option 2 — strategy?
Therapist on weak side, pull patient toward weak side, promote weight bearing.
What if a patient avoids weak side?
Place step under strong leg.
What is Transfer Option 3 — bilateral weakness?
Stand in front, block knees, assist stepping and turning.
What is the primary purpose of gait training?
Drive afferent nervous system to promote recovery.
What is included in balance training?
Progressive balance challenges.
What is the exercise progression for TBI patients?
Supine → sidelying, sidelying → sitting, edge of bed exercises, sit to stand, standing weight shifting.
How should balance training be performed in MS?
Vary surfaces, directions, and perturbations.
What are the stretching guidelines for MS patients?
30-60 sec holds, 2-3 times per muscle group.
What is the strengthening program for MS patients?
Bridging, sit-to-stands, UE and LE strengthening, resistance bands.
What are functional activities for MS patients?
TUG-style activities.
How do you train rolling in a hemiparetic patient?
Roll toward strong side, strong arm pushes, strong leg assists, bring weak arm across.
What must be included in a PT goal?
Time frame, level of assistance, measurable objective, functional.
What HR range is high intensity gait training?
70-85% max HR.
How do you calculate HR max?
208 − (0.7 × age).
What is the purpose of HIGT?
Promote neuroplasticity, increase BDNF. (Brain derived Neurotrophic factor)
What is the correct dosage principle for HIGT?
High repetitions are most important. Do a set of 10 then increase difficulty
What is the frequency/time for HIGT?
Inpatient 4-5x/week, 30-60 min, 400-2000 steps; Outpatient every session.
What is the intensity for HIGT?
70-85% max HR, RPE 15-18, beta blockers reduce HR by 10 bpm.
What type of HIGT is used?
Task-specific gait training.
What are the heart rate safety parameters?
60-120 resting, stop if >85% max HR.
What are the blood pressure limits?
Stop >180/110 rest or >250/115 exercise, monitor <90/60, stop if SBP increase with ischemia.
What is the oxygen saturation cutoff?
Stop if <92%.
What are the blood glucose limits?
Stop <70 or >250, monitor 70-250.
When is HIGT appropriate?
Patient can bear weight, has goal to walk, no arrhythmias or intolerance.