Cognitive and Eating Disorder
1/76
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
77 Terms
Reasoning
Judgment
Attention
Perception
Comprehension
Memory
Cogntive Abilities
Delirium
Disturbances of consciousness
Short period of time and fluctuating
Older acutely ill clients
Easily distracted and disoriented
Sensory Disturbances
Risk factors of delirium
Physical illness: surgery, disease, fatigue
Older age
Cognitive impairment: dementia
Febrile illness/drug-related: children
Hyperactive delirium symptoms
Hallucination/illness
Easily irritated
Delusions
Confusion/disorientation
Language difficulty
Disorganized thoughts
Misinterpretation
Hypoactive delirium symptoms
Fear/anxiety
Gloomy
Sluggish
Withdrawn
Silence
Apathy
Etiology (Videbeck) of delirium
Physiologic or metabolic
Infection
Drug-related
Nursing Consideration
It is very important to know the cause of delirium for the team to identify the appropriate treatment plan
Pathophysiology theories of delirium
Delirium
Drugs
Coritsol
Inflammatory conditions
Oxidative impairment
Neurotransmitters
Dopamine
GABA
Serotonin
Ach
Nursing consideration of delirium for psychopharma
It is very important to know the cause of delirium for the team to identify the appropriate treatment plan
Not indicated for hypoactive
Symptomatic for hyperactive
Haloperidol (Antipsychotic) for hallucination/illusion
Sedatives for calming effect
Acute confusion
Managing confusion will help patient manage personal daily activities, prevent from any forms of injury, manifest good social behaviors/interaction, and reduce psychotic episodes
Nursing Care Plan Assessment
History - drug-use, alcohol intake, and medications
Motor behavior - hyper or hypo
Mood and affect - observe fluctuations
Thought process - disorganized and fragmented
Sensorium and Intellectual Process - Disorientation, confusion, delusion, hallucination, illusion
Judgment and Insight - Impaired reasoning
Roles and Relationship - Role impairment
Self-concept - Feel bad about self
Physiologic and Self-care considerations - Sleep, eating, void, hygiene, leisure
Nursing Care Plan Goal
Free from Injury
Intact with reality
Normal Sleep-Wake Cycle
Maintain proper nutrition
Good hydration
Optimum level of functioning
Promote client safety
Priority focus of delirium nursing intervention
Therapeutic communication
Manage client’s confusion for delirium
Controlling environment (milieu management)
Intervention for environment in nursing
Routine
Promote sleep and priority
Dementia
A mental disorder that involves multiple cognitive deficits, initially, memory impairment, and later, the following cognitive disturbances (Videback)
Aphasia
Deterioration of language function
Agnosia
Inablitiy to recognize name of objects
Apraxia
Impaired motor function
Echolalia
involuntary repetition of words, phrases, or sounds spoken by others
Palilalia
a rare speech disorder characterized by the involuntary, self-repetition of words, phrases, or sentences just spoken
Disturbance in executive functioning
Inability to think abstractly
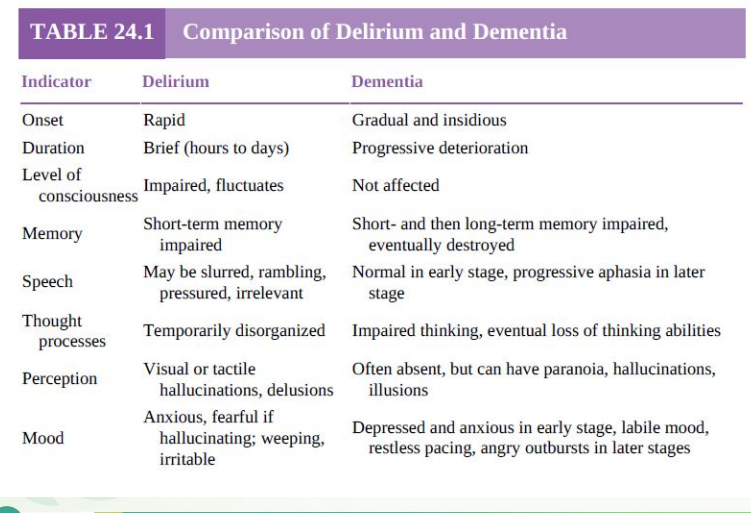
Comparison of Delirium and Dementia
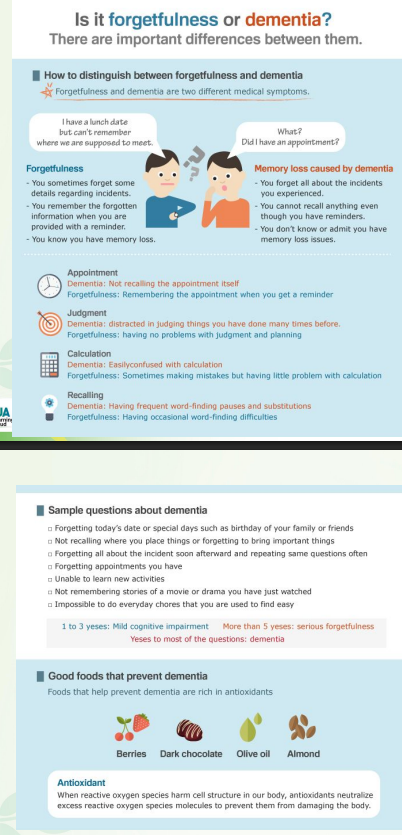
Comparison of forgetfulness or dementia
Dementia
According to Alzheimer’s Disease Association of the Philippines (ADAP) As one gets older, it is normal to be a little bit forgetful. If forgetting becomes more frequent, affecting routine daily activities and decision-making, and often accompanied by changes in personality or behavior, it’s _____
Memory
Language
Judgment
Reason
Signs and symptoms of dementia (ADAP)
Affects social and occupational functioning:
activities of daily living
behavior
cognition
Dementia - early stage
Become forgetful, especially things that just happened (hallmark beginning)
Some difficulty with communication
Difficulty in keeping things and handling personal finances
Mood and behavior:
less active and motivated and lose interest in activities and hobbies
may react unusually angrily or aggressively on occasion
Dementia - Mild Stage
Become very forgetful, especially of recent events and names of unfamiliar people (Progressive Memory loss)
Can still comprehending time, date, place and events with some difficulties
Need help with personal care (i.e. toileting, dressing)
Unable to prepare food, cook, clean or shop (Complex tasks)
Unable to live alone safely without considerable support
Dementia - Late Stage
Unaware of time and place
May not understand what is happening around them
Unable to recognize relatives, and friends
Unable to eat and walk without assistance
Increasing need for assisted self-care
May have bladder and bowel incontinence
Behaviour changes (e.g. wandering, repeated questioning, calling out, clinging, disturbed sleeping, hallucinations)
Inappropriate behaviour (e.g. disinhibition, aggression)
Reversible types of dementia
Caused by tumors, hypothyroidism, drugs or psychiatric related
Irreversible types of dementia
Examples are alzheimer’s disease, vascular dementia, parkinson’s disease
Parkinosn’s
Trigerred by the individual’s existing medical condition of parkinson’s
slowly progressive neurologic condition characterized by tremor, rigidity, bradykinesia, and postural instability.
Creuzfeldt-Jakob
Rare form of dementia caused by the abnormality of prion, a protein found in the brain, which is toxic to brain cells
Hunington’s disease
Progressive brain disorder caused by a single defective gene on chromosome 4, affecting the central are of the brain
Fronototemporal
Also known as Pick’s disease. Relatively rare form which affect the brain where language and behavior are controlled
Normal-pressure hydrocephalus
When excess cerebrospinal fluid (CSF) accumulates in the brain’s ventricles affecting its tissue. Can be reversed or controlled
Wernicke-Korsakoff Syndrome
Chronic memory disorder caused by severe deficiency of thiamine (vitamine B1). Commonly linked with alcohol misuse
Mixed
A combination of two or more types of dementia in an individual. Most common is Alzheimer’s disease with vascular dementia
Alzheimer’s disease
The most prevalent type of dementia. Approximately 50-70%
Vascular or dementia
The second most common type of dementia is caused by multiple strokes due to interrupted blood flow to the brain. Approximately 20-30%
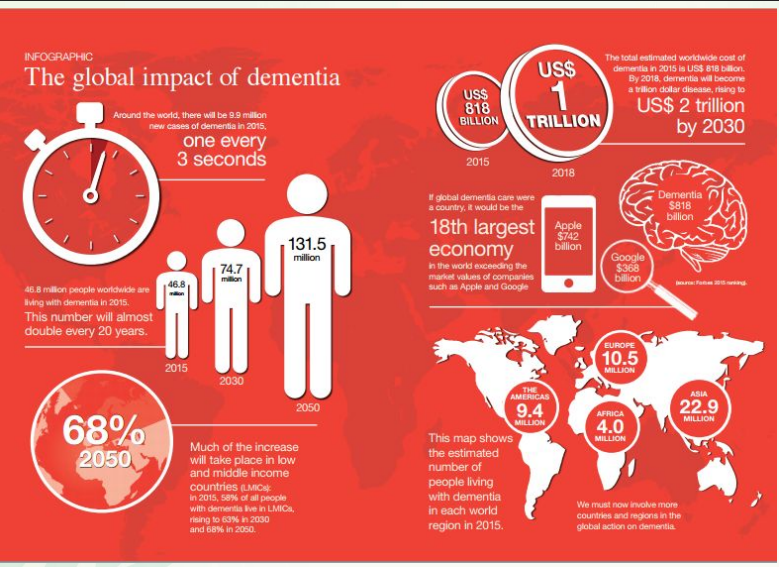
Global impact of dementia
The world’s older population currently comprises nearly 900 million people. Most live in what are currently relatively poor countries
Nursing consideration of dementia
Proper identification of the underlying condition is vital for the treatment plan.
Total assistance
Dementia is a progressive deterioration of cognitive and physical abilities until death. Later stages of Dementia require ___
Cholinesterase inhibitors
Donepezil (Aricept)
Rivastigine (Exelon)
Memantine (Namenda)
Medications for dementia
Dementia Nursing care plan assessment
History - interview family members
Motor behavior - inability to sustain meaningful conversation
Unusual behaviors (dec. motor and uninhibited)
Mood and affect
Anxiety and Labile mood
Emotional Outburst
Wandering at night
Loss of personal control
Apathetic
Through process
impaired abstract and logical thinking
Delusions and persecutions
Sensorium and Intellectual Process
Confabulation
Impaired attention span
Confusion
Hallucinations
Judgment and Insight - Underestimating risks of disease
Roles and relationship - Affected work performance
Families being caregivers
Impaired House and Family responsibilities
Physiologic and self-care considerations - sleep, eating, void, hygiene, leisure
Dementia Nursing care plan goal
Free from Injury
Rest-Activity Balance
Maintain proper nutrition
Good hydration
Regular Voiding
Independent Functioning
Respected and Supported
Community involvement
Promote client safety
Promoting adequate sleep and proper nutrition, hygiene and activity
Eating, bathing, dressing, transferring, toileting, walking or moving around
Intervention for dementia
Providing emotional support
Promoting interaction and involvement
Establishing trust
Person with dementia may have cognitive impairments which will limit your communications
Make an effort to communicate with both the person and the carers
Make sure the person can see and hear properly (e.g. spectacles may no longer be of the right prescription, or a hearing aid may not be working properly
Speak clearly, slowly and with eye contact
Pay attention to body language - people whose language is impaired often communicate through non-verbal means
Provide the carer and family with opportunities to express their worries and concerns about the person’s illness
Listen carefully to the concerns of the carer and family members
Highlight the positive aspects of the family – Congratulate the family for taking such good care of the person if appropriate
Be flexible in your approach with the carer and family. The family may come to you with needs you did not expect.
Reminiscence therapy
With the family
Remote memory of the patient
Use of photo album or music or movies
Conversations and active listening
Caregiver burden
The hidden patient
Emotionally and physically exhausting
Round the clock care
Stressful
Role Strain
Unappreciated
Most of the caregivers are immediate family members
Caregiver burden management
Having a stress –free caregiver will tolerate the burden of assisting Dementia patient, in turn, will make the patient sustain optimum state of well being and slowing down the deterioration of cognition.
Include in decision making
Constant education about dementia
Stress management
Communication and endorsement
Ethical consideration
Maintain dignity
Emotional support
End of life care
Anorexia Nervosa
14 to 18 years old
Starts with denial and anxiety
Unable to identify or to explain their emotions about life events
Noticeable changes in mood
Social isolation
Restricting
Binge eating and purging
Subtypes of anorexia nervosa
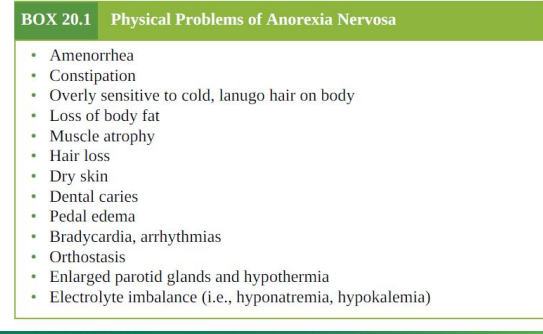
Medical complications of anorexia nervosa
Clients with the lowest body weights and longest durations of illness tended to relapse and have the poorest outcomes
Medical complications related to weight loss
Musculoskeletal - Loss of muscle mass
Metabolic – Hypothyroidism, hypoglycemia, and dec. insulin sensitivity
Cardiac - Bradycardia, hypotension, cardiac arrhythmias
Gastrointestinal - Delayed gastric emptying, bloating, constipation, abdominal pain, gas, and diarrhea
Reproductive - Amenorrhea and low levels of luteinizing and follicle-stimulating hormones
Dermatologic - Dry, cracking skin due to dehydration, edema, and acrocyanosis (i.e., blue hands and feet)
Hematologic - Leukopenia, anemia, thrombocytopenia
Neuropsychiatric - Abnormal taste sensation, apathetic depression and sleep disturbances
Medical complications related to purging and laxatives
Metabolic - hypokalemia, hypochloremic alkalosis, hypomagnesemia, and elevated blood urea nitrogen
Gastrointestinal - Esophageal and gastric erosion or rupture, dysfunctional bowel, and superior mesenteric artery syndrome
Dental - Erosion of dental enamel (perimyolysis)
Neuropsychiatric – Seizures, mild neuropathies, fatigue, and weakness
Severe fluid, electrolyte, and metabolic imbalances
Cardiovascular complications
Severe weight loss and its consequences
Risk for Suicide
Major life- threatening complications that indicate the need for hospital admission include:
Weight restoration
Nutritional rehabilitation
Rehydration
Correction of electrolyte imbalances
Severely malnourished clients may require total parenteral nutrition, tube feedings, or hyperalimentation (IV nutrition) to receive adequate nutritional intake
Medical management focuses on:
Amitriptyline (Elavil)
Cyproheptadine (Periactin)
Medications for weight gain
Olanzapine (Zyprexa)
Medications for bizarre body image distortion (psychosis)
Fluoxetine (Prozac)
Medications for relapse prevention
Psychotherapy for anorexia nervosa
Family therapy
Individual therapy
Targets coping skills, self-esteem, self-acceptance, interpersonal relationships, assertiveness, can improve overall functioning and life satisfaction.
Individual therapy
For clients contraindicated to family therapy
For older clients
For clients with individual issues
Bulimia Nervosa
Late adolescence (18 yo) or early adulthood
Begins during or after a diet regimen
People who eat restrictively, which leads to purging and binging
Storing foods and goes to food stores
Bulimia Nervosa Outcomes
Clients with a comorbid personality disorder tend to have poorer outcomes than those without
Hospital admission is indicated if binging and purging behaviors are out of control and the client’s medical status is compromised
The death rate from bulimia is estimated at 3% or less.
Cognitive-behavioral therapy
Food focus on interrupting the cycle of dieting, binging, and purging
Altering dysfunctional thoughts and beliefs about food, weight, body image, and overall selfconcept
Desipramine (Norpramin)
Imipramine (Tofranil)
Amitriptyline (Elavil)
Nortriptyline (Pamelor)
Phenelzine (Nardil)
Fluoxetine (Prozac)
Psychopharmacology for bulimia nervosa
Binge-purge type vs bulimia
Nursing care plan assessment bulmia nervosa
History - According to Family Members
Anorexia - shift in mood
Bulimia - impulsive behavior
Appearance
Anorexia – Low weight
Bulimia – Normal weight
Motor Behavior
Anorexia - slow, lethargic, and fatigued turns away, avoiding discussing the problem
Bulimia - appears normal and willing
Mood and Affect
Avoiding “bad” or fattening foods gives them a sense of power and control over their bodies
Eating, binging, or purging leads to anxiety, depression, and feeling out of control.
Most of the time, for Anorexia: Serious; Bulimia: Cheerful
Suicide are common to those with history of sexual abuse
Thought Process
Preoccupied with their attempts to avoid eating or eating “bad” or “wrong” foods
Delusional Body image disturbance
Paranoid ideas for those who are suggesting them to eat
Sensorium and Intellectual Processes - Only with complications of malnutrition: confusion, slowed mental processes, difficulty with focus and attention
Judgment and Insight
For Anorexia, they do not believe they have a problem
For Bulimia, they recognize the problem; ashamed of their binging / purging
Self-concept
Low self esteem, helpless, powerless, and ineffective
See themselves badly if not able to follow food restrictions
Doesn’t see any other achievements in life, but only achievements whenever they have controlled food
Roles and Relationships - Eating disorder interferes with roles relationships
Physiologic and Self-Care Considerations
Relates directly to the severity of self-starvation and purging
Exercises excessively
Sleep disturbances
Dental and oral cavity problems
Nursing care plan goal bulmia nervosa
Physiologic outcomes
Treat malnutrition
Treat medical complications
Psychological outcomes
Nutritional Eating patterns
Eliminate compensatory behaviors
Coping mechanism about food
Verbalize feelings of guilt, anger, anxiety, and food control
Accept Body image
Nutritional rehabilitation for anorexia
Gradual increases in calories
Avoid food rituals
Purging supervision (1-2 hrs after meals)
Nutritional rehabilitation for bulimia
outpatient
Eat with Family and Friends
Eat a planned Menu
Emotions and coping
Recognize emotions towards eating as anxiety / guilt
Self-monitoring - increase client’s awareness of their eating patterns
Body Image
Emphasize on health
Focus on other strengths aside from food control
Client and family education
Nutritional education and prevention of complications
Distraction Delaying Techniques – for binging / purging
Emotional support, love, and attention and concern about client’s health