Lecture 22 - Leukaemia and its treatment
1/34
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
35 Terms
What is Acute Lymphoblastic Leukaemia?
Clonal expansion of lymphoid progenitors
B-cell, pre-B cell and T-cell
Most commonly the cause of death is from malignancy
What are the symptoms of ALL?
Generalised weakness and fatigue
Anaemia
Excessive bruising/bleeding
Unexplained/Rare infections and fever
Enlarged lymph nodes
What chromosomal abnormalities are seen in ALL?
Numerical
Hyperdiploidy
Hypodiploidy
Structural
Chromosomal translocations
T(12;21)
T(9;22)
Translocations involving mixed lymphoid leukaemia (MLL) gene
What is Hyperdiploidy?
More chromosomes
What is hypodiploidy?
Less chromosomes
How often is T(12;21) seen in ALL?
25% of cases
How often is T(9;22) seen in ALL?
3% of cases
Which age group are translocations involving mixed lymphoid leukaemia (MLL) gene seen?
Mostly seen in infants
Why do chromosomal translocations result in ALL development?
Leads to fusion proteins
Gene fusion results in chimeric A-B fusion genes being translated into fusion proteins
These fusion proteins are related to normal gene function
E.g. ABL in BCR/ABL
What is Core binding factor protein A-2?
Core binding factor protein A-2 (CBFA-2)(RUNX1) is a heterodimeric transcription factor made of RUNX1 and CBFB
Plays a role in regulating blood cell development
Either activates or represses its target genes by recruiting p300 or HDAC respectively
CBFA-2/RUNX1 activates its target genes by recruiting…
p300
CBFA-2/RUNX1 represses its target genes by recruiting…
HDAC
What is EVT6 RUNX1 protein?
Fusion gene which recruits HDAC complex
Allows formation of a very stable repressor complex
Represses RUNX1 target genes
How does the MLL gene play a role in ALL?
Encodes a DNA binding protein which methylates histones
Positively regulates gene expression, including HOX genes
However, fusion genes of MLL lose intrinsic methyltransferase activity but gain the ability to form complexes to bind targets as well as recruiting the methyltransferase DOT1L
This represses differentiation of lymphocytes while overexpressing HOX genes driving proliferation
What is the methyltransferase which fusion MLL proteins can recruit to hypermethylate histones?
The methyltransferase DOT1L
How is sex a prognostic factor of ALL at diagnosis?
Males generally perform worse
How is age a prognostic factor of ALL at diagnosis?
>10 years old have worse prognosis
How is while blood cell count a prognostic factor of ALL at diagnosis?
High white blood cell count generally indicates a poor prognosis
How is where the cancer spreads a prognostic factor of ALL at diagnosis?
Cancer spread to brain/spinal cord
Associated with worse prognosis
In ALL patients, Philadelphia chromosome and hypodiploidy are associated with _____ prognosis.
In ALL patients, Philadelphia chromosome and hypodiploidy are associated with worse prognosis.
In ALL patients, T(12;21) and Hyperdiploidy are associated with _____ prognosis.
In ALL patients, T(12;21) and Hyperdiploidy are associated with better prognosis.
>25% leukaemic blasts at day 8-15 of treatment is associated with______?
>25% leukemic blasts at day 8-15 is associated with a higher risk of relapse.
What is minimal residual disease?
Refers to the small number of cancer cells that remain in a patient's body during or after treatment
Often a good indicator of relapse risk
How does minimal residual disease relate to patient prognosis?
Presence of minimal residual disease is closely related to the risk of relapse
Risk of relapse rises steeply with the amount of minimal residual disease
Also independent of other prognostic factors
What is somatic rearrangement which occurs during lymphocyte development?
T-cell receptor and immunoglobulin loci undergo somatic rearrangement to allow the recognition of millions of diverse antigens
Receptors have heavy and light chains with both constant and variable regions
These regions are rearranged to produce unique receptors
How can somatic rearrangements be used in minimal residual disease assessments?
Identify specific clonal rearrangement of the child’s leukaemic cells
Use PCR to specifically detect any residual leukemic clone
Sensitivity -0.01 to 0.001%
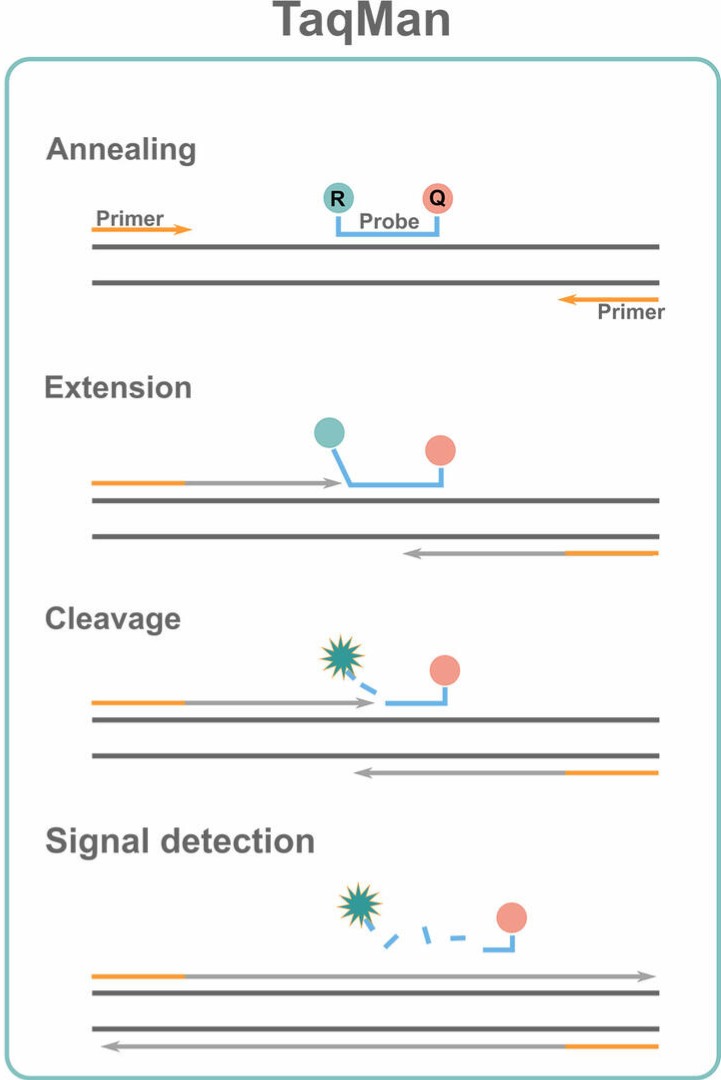
What is Taqman Hydrolysis Probes?
Probe is conjugated with a quencher fluorochrome which absorbs the fluorescence of the reporter
On amplification of the target, the 5’ exonuclease activity of Taq polymerase hydrolyses the probe causing separation of reporter and quencher
This generates a fluorescent signal
Each consecutive cycle causes exponential reporter fluorescence
This can then be measured using a computer
What are the therapeutic approaches to treating ALL?
Chemotherapy
Combination of many different therapies
Radiation therapy
Painful in bony areas and high disease burden
Bone marrow transplant
Requires whole body radiation
Intensive combined chemo and radio therapy
Surgery
Novel agents
Early during ALL treatment, what was the treatment given?
Early on therapy was not given
As drugs started to be given, more children were surviving
What are the key clinical challenges of treating ALL in children?
Toxicity issues
Overtreatment of some cancers
How can treatment be tailored to each patient?
Use of prognostic markers to tailor treatment
Poor prognostic patient groups receive more intensive therapy to improve chances of survival
Good prognostic patient groups may be considered for less intensive protocols
Reduce toxicity without reducing survival rates
The study which attempted tailored treatment based on prognostic markers found what?
Treatment reduction was possible
Patients on intermediate treatment who responded well could be given less treatment with no difference in survival or relapse
Treatment intensification also aided patients
Showed increasing treatment appeared to help patients who responded poorly to initial treatment
HOWEVER, overall survival was not significant due to the increased toxicity
Imatinib is a targeted therapy which targets what? What type of cancer can it be used to treat?
Targets the BCR-ABL fusion protein and competitively inhibits it
Can therefore only be used on Philadelphia chromosome-positive CML/ALL as the BCR-ABL fusion protein is present
Continuous imatinib exposure in Ph+ ALL patients resulted in what?
Continuous imatanib exposure improved outcome 80% event free survival when compared to historical controls (35%)
There were no significant toxicities associated with adding imatinib to intensive chemotherapy
What are the current critical challenges in ALL treatment?
Further increase survival rates
Achieve a cure with minimal toxicity