Cancer Pain Management
1/31
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
32 Terms
incidence
65-85% pts with advanced cancer experience pain
generates great deal of anxiety → treatment is impactful!
influenced & potentially enhanced by existential sources: cultural, spiritual, psychosocial pain
pure opioids, non-opioids (NSAIDs/APAP) & adjuvants
National Comprehensive Cancer Network (NCCN) adult cancer pain guidelines
survival linked to symptom control & pain management, which contributes to broad quality of life improvement
pain management - essential part of oncologic management → prolong survival
analgesic options
pure opioids & methadone
adjuvants
• neuropathic agents: antiepileptic drug (AED), TCA, SNRI
• musculoskeletal agents: cyclobenzaprine
• topical: NSAID, lidocaine
• miscellaneous: ketamine
non-opioids: NSAIDs, APAP
7 pure opioids
morphine
oxycodone
hydromorphone
fentanyl
oxymorphone
hydrocodone
methadone
opioid review
dosing frequency for long-acting morphine, oxycodone, oxymorphone: q8hr & q12hr - NEVER for breakthrough pain
dosing frequency for IR opioids: q3-4hr PRN or q1hr PRN
ALL have issues with accumulation during renal failure, esp. morphine (metabolites accumulation can cause problem)
methadone (Dolophine®)
MOA: NMDA antagonist, mu (but less), 5HT, inhibits reuptake of serotonin & NE
*help prevent neurotoxicity & opioid tolerance
different conversion protocols
for opioid-tolerant pts → indicated for moderate-to-severe pain
metabolism: CYP3A4, 2B6, 2C19 & highly protein bound
• 80-90%
• unpredictable pharmacokinetics
t½ = 8-59 hrs
dosing frequency (pain): q6, 8, 12, 24hr ATC (addiction dose)
5-7 days for steady state → titration every 5-7 days (long-acting)
ADE: sedation, arrhythmia, sweating, constipation
methadone: 6 items to know
role in somatic & neuropathic pain
role in rapidly escalating opioid doses
option for neurotoxicity management - unwanted SE of opioids
less sedation & constipation vs. opioids
NO renal concerns but issues with hepatic dysfunction → be cautious
experience required
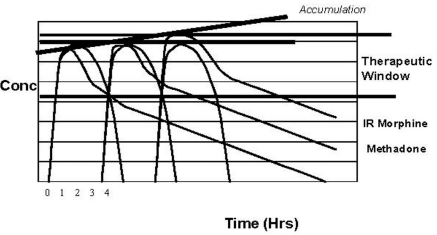
methadone elimination curve
therapeutic window = good pain coverage
IR morphine - peaks & goes down
methadone - 2 phases of elimination
• rate depends on liver fxn
• variable t½
methadone: IV formulations
only long acting IV opioid product available
• NOT 1:1 conversion, generally 2:1
may dose SQ/IV q8h OR q12h
• SQ - possible local irritation
continuous infusion typically NOT necessary
• greater risk of QT interval prolongation due to preservative (chlorobutanol) → to avoid switch to preservative-free
methadone cardiac concerns: consensus recommendations
assess for arrhythmias, structural heart disease & h/o syncope
inappropriate use
• congenital/acquired QT prolongation: structural heart disease (arrhythmias, syncope)
➢ QT = 450-500ms → risk vs. benefit & increase monitoring
• electrolyte imbalances (K, Mg, Ca): hypokalemia, hypomagnesemia, hypocalcemia → have to correct 1st unless have chronic issue
• liver failure: accumulation
monitoring standard
• educate pts regarding arrhythmia risk
• obtain pretreatment ECG for ALL pts - follow up in 30 days, then annually
additional ECG monitoring indicated for
• >100mg/d, syncope reported &/or seizures
• PRN individual circumstances
methadone: drug interactions
many drugs can cause QT prolongation → screen!
*cigarette smoking
when in doubt, look it up!
cancer pain assessment
assess etiology, pathophysiology (metastatic spread), cancer pain syndromes & pt goals for comfort/functionality/safety
*treatment-related, know where it comes from
cancer pain assessment: cancer pain syndromes
inflammation &/or nerve compression
neuropathic pain
bone pain
mucositis - worst!
immunotherapy-related polyarthralgia
lesion related pain
severe refractory pain in imminently dying pts
cancer pain syndrome: inflammation/nerve compression
etiology
• inflammation: tumor (ball of inflammation)/mets (spread from original tumor) location (direct effect on tissue)
• nerve compression (NC): bone mets in spinal cord, tumor invasion, treatment-induced osteoporosis
➢ common sites: back, neck, leg (sciatic), pelvis
*pancreatic cancer - celiac plexus, prostate cancer - bone
treatment (acute): dexamethasone (burst therapy then possible maintenance therapy)
maintenance (chronic)
• NC: consider antidepressant, anticonvulsant (Lyrica), topical agent, methadone or interventional strategies (nerve block)
cancer pain syndrome: bone pain
caused by either primary tumor or metastatic spread
local: palliative radiation, nerve block (celiac, hypogastric, intercostal plexus block), percutaneous ablation, NSAID (bleeding risk)/COX-2/APAP, assess for pathologic fractures
• pathologic fracture (non-healable)/weakness → consult orthopedics for stabilization
diffuse (systemic approach): bisphosphonate trial, steroids (caution w/ chemo/immunotherapy), NSAID/COX-2/APAP, hormone therapy, chemotherapy, radioisotopes
cancer pain syndrome: bone pain - bisphosphonates (IV)
inhibit resorption & delay skeletal events in pts w/ osteolytic bone metastasis
decreases pathologic fractures, spinal compression & hypercalcemia
4 agents
• zoledronic acid (Zometa) - most common
• pamidronate (Aredia)
• denosumab (Xgeva)
• ibandronate (Boniva) - off label
cancer pain syndrome: bone pain - bisphosphonates (IV): zoledronic acid (Zometa)
4 mg q3-4 wks, infuse 15-30 mins; most common
APAP prior may decrease acute rxn
• within 3 days in 44% of pts (max 14 days)
• pretreat with APAP before & 72 hrs post
renal adjustment CrCl <60 mL/min
cancer pain syndrome: bone pain - bisphosphonates (IV): pamidronate (Aredia)
90 mg over 2-4 hrs q3-4 weeks
renal adjustments (longer infusions may decrease renal toxicity)
cancer pain syndrome: bone pain - bisphosphonates (IV): osteonecrosis of jaw
non-healing extraction of socket or exposed jaw bone
more common in multiple myeloma & breast cancer
counseling: dental exams, good oral hygiene w/ nice soft toothbrush, gargle with salt water & report oral mucosal changes ASAP
cancer pain syndrome: bone pain - systemic radionuclide therapy
strontium (Metastron) IV infusion
• can provide relief up to 3-6 months
*can experience increased pain 36-72 hr post infusion
considered when
• multiple, remote bone lesions
• life expectancy >6 months
• unable to tolerate systemic pharmacotherapy OR refractory disease pain
*palliative care?
caution in immunosuppressed
cancer pain assessment: oncologic emergencies
bone fracture
neuroaxial metastases w/ threatened injury
infection
acute abdomen
thrombotic emergency
cancer pain assessment: pain not related cancer pain syndromes or oncologic emergencies
opioid naïve
opioid tolerant
pain assessment tools
before, during, after therapy changes or ends
• change in pain must be investigated
*any new pain, movement or worsening
PQRST evaluation
• palliative/precipitating factors
• quality
• region of body
• subjective description
• temporal/time frame
brief pain inventory (BPI) - assess pain & overall impact on quality of life in chronic painful diseases/conditions
opioid naïve* pts: general principles
*<60 OME/day for at least 1 week
medication selection based on
• pain physiology
• comorbid conditions
• drug interactions
• cost
anticipate/treat analgesic SE - constipation
provide psychosocial support
provide family/caregiver education
optimize integrative interventions
analgesic regimen: NSAIDs/APAP, opioid, adjuvant analgesic
opioid naïve* pts: score & medications
severe/pain crisis → acute, severe pain crisis consider IPU or hospice consult to achieve pt-specific goals for comfort & function
*do NOT treat at home → inpatient
moderate/severe
• adding NSAIDs/APAP + adjuvants with IR opioids PRN
• morphine IR 5 mg PO (solution; higher absorption), 7.5 mg (tablet) or equivalent
• titrate IR opioids q3-4h PRN or q1hr PRN
• IF multiple doses needed consistently, consider converting to scheduled long-acting regimen
mild
• consider adding NSAIDs or APAP
• adjuvants = muscle relaxants, neuropathic agents, topical
opioid naïve* pts: severe/pain crisis score
consider inpatient unit (IPU) or hospice consult to achieve patient-specific goals for comfort & function
*do NOT treat at home → inpatient
opioid naïve* pts: moderate/severe score
adding NSAIDs/APAP + adjuvants with IR opioids PRN
morphine IR 5 mg PO (solution; higher absorption), 7.5 mg (tablet) or equivalent
titrate IR opioids q3-4h PRN or q1hr PRN
IF multiple doses needed consistently, consider converting to scheduled long-acting regimen
PO peak 60 min → MS IR 5-15 mg
• pain unchanged/increased → increase dose 50-100%
• pain ↓ but inadequate → repeat same dose
• pain improved & adequate → continue PRN, follow up in 24 hrs
opioid naïve* pts: mild score
consider adding NSAIDs or APAP
adjuvants = muscle relaxants, neuropathic agents, topical
opioid tolerant* pts: general principles
*≥60 OME/day for at least 1 week
medication selection based on
• pain physiology
• comorbid conditions
• drug interactions
• cost
continue treatment of SE - bowel movements
provide psychosocial support
provide patient & family education
optimize integrative interventions
analgesic regimen: NSAIDs/APAP, opioid, adjuvant analgesic
opioid tolerant* pts: mild pain
adding NSAID/APAP &/or adjuvant therapies, unless C/I
may consider opioid reduction (10-20%) IF
• rare use of PRN/breakthrough
• well-controlled pain/stable disease/acute event over
• unwanted/unmanageable ADE
• safety concerns - sedation d/t sepsis ~50-75%
• worsening pain with increasing dose, possible hyperalgesia/neurotoxicity
opioid tolerant* pts: moderate/severe pain
NSAIDs/APAP, adjuvants with IR opioids PRN
• titrate IR opioids, increase total daily dose (TDD) 30-100%
• IF multiple doses needed/day (consistently) → addition/increase dose of long acting opioid
PO peak 60 min → 10-20% of TDD
• pain unchanged/increased → increase dose 50-100%
• pain ↓ but inadequate → repeat same dose
• pain improved & adequate → continue PRN, follow up in 24 hrs
opioid tolerant* pts: acute, severe pain crisis
consider hospital or inpatient unit (IPU) hospice to achieve patient-specific goals for comfort & function