Thoracis drains
1/39
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
40 Terms
What is a Thoracic Drain?
A chest drain is a tube that is temporarily placed into the plural space, within the chest cavity, to allow drainage of air or effusion. They are also known as a chest tube or a thoracostomy tube
Indications for a Thoracic Drain?
1 - Following surgery
2 - Management of plural effusion where repeated thoracentesis is required
3 - Management of pneumothorax
Indications for a thoracic drain - Following surgery
Remove air that has accumulated during a thoracotomy
To allow re-expansion of the lungs
To monitor for blood or continuous air production (indicating leaking)
They can also be used as a trouble to deliver treatment - whether that be lavage fluids for a prothorax or administration of local anaesthetic following thoracic surgery
Indications for thoracic drain - Management of pleural effusion where repeated thoracentesis is required
Prothorax
Chylothorax
Haemothorax
Hydrothorax
Neoplastic effusion

Trochar thoracic drain
This uses a trochar ‘stylet’ to aid the tubes entry into the pleural space. They can be more traumatic to place but have a larger diameter therefore rarely obstruct
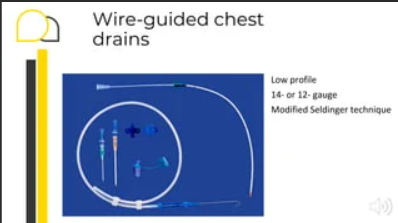
Small bore wire-guided thoracic drain
This type of drain can be placed using a ‘Selinger’ technique. It is smaller in diameter therefore is considered less traumatic to place and well tolerated however, they can obstruct more easily
Types of Thoracic Drain - Most drains are made of silicone or PVC and are either a ..
Trochar thoracic drain
Small bore wire-guided
In any case, the chest tube of choice should have the following properties ..
Be flexible and not collapse
Be able to be sterilised
Internal diameter should be 1/2 - 2/3rds of the width of an intercostal space
The length of the tube should allow it to sit at the ventral aspect of the 2nd / 3rd rib
Have at least 3 Sid holes and an end hole (all of which need to be within the chest cavity). Additional holes can be made but must be <1/3rd of the tube diameter to avoid kinking
Placement of a thoracic drain can either be classed as ..
Open - placed during thoracic surgery
Closed - Placed ‘blind’ i.e. not via thoracotomy
Placement technique - Equipment
Clippers
Equipment for surgical prep
Sterile gloves
Local anaesthetic
Surgical kit - scalpel, scalpel holder, scissors, needle holder
Suitable thoracic drain
Gate clap / C-clamp
Suture material
Sterile dressing - e.g. primapore
Material for a chest bandage or mesh dressing
Patient preparation - Anaesthesia
Chest drain placement is painful therefore anaesthesia is recommended in these animal as it also allows rapid control of their airway with and ET tube and allows IPPV if necessary.
However, in high risk patients where they are not deemed stable enough to undergo general anesthetic, a combination of sedation and local anaesthetic can be used
Patient preparation - Positioning
The patient is placed into lateral recumbency
Which side of the chest tube is placed is determined by evaluating the thoracic radiographs or by which side was most productive on thoracocentesis
In the majority of patient, one thoracic drain is sufficient as the mediastinum is permeable to fluid and air
However, especially in the cases of thick purulent fluid (i.e. pyothorax) then bilateral thoracic drains may be placed
Measuring the Thoracic Drain
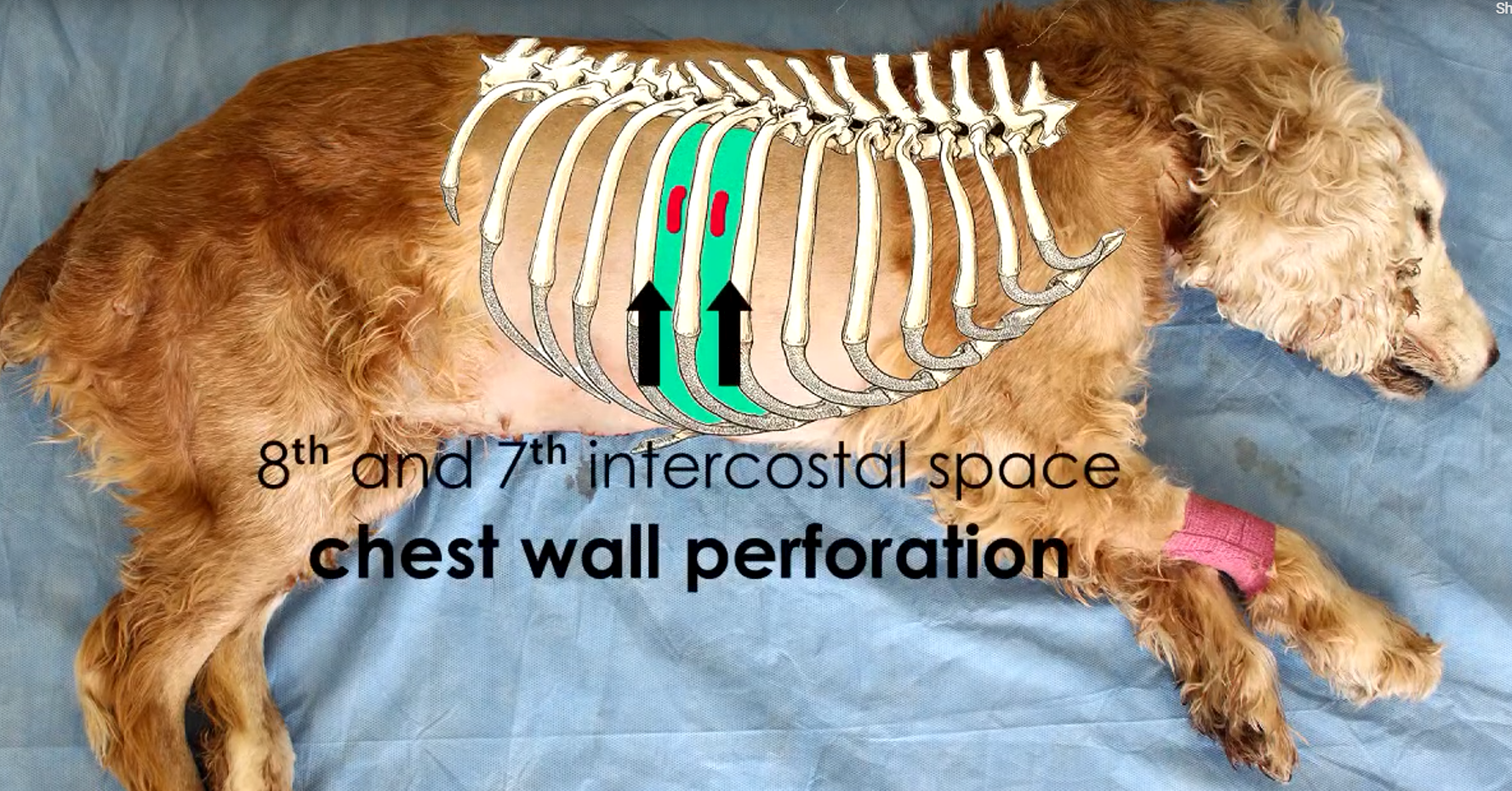
Prior to placement, the tube should be measured from the point of entry at around the 10th intercostal space, ventrocranially the 2nd/3rd intercostal space.
The tube as to remain sterile (so we cannot make a mark on it as we would for feeding tubes) so a mental note of the number on the drain is made
At this stage, additional holes can be made in the tube if required
While the patient is under anesthetic, why is it important to tap the chest before placing a Trochar thoracic tube?
To evacuate it of any accumulated air that may occur as a result of being put on pressurised gas
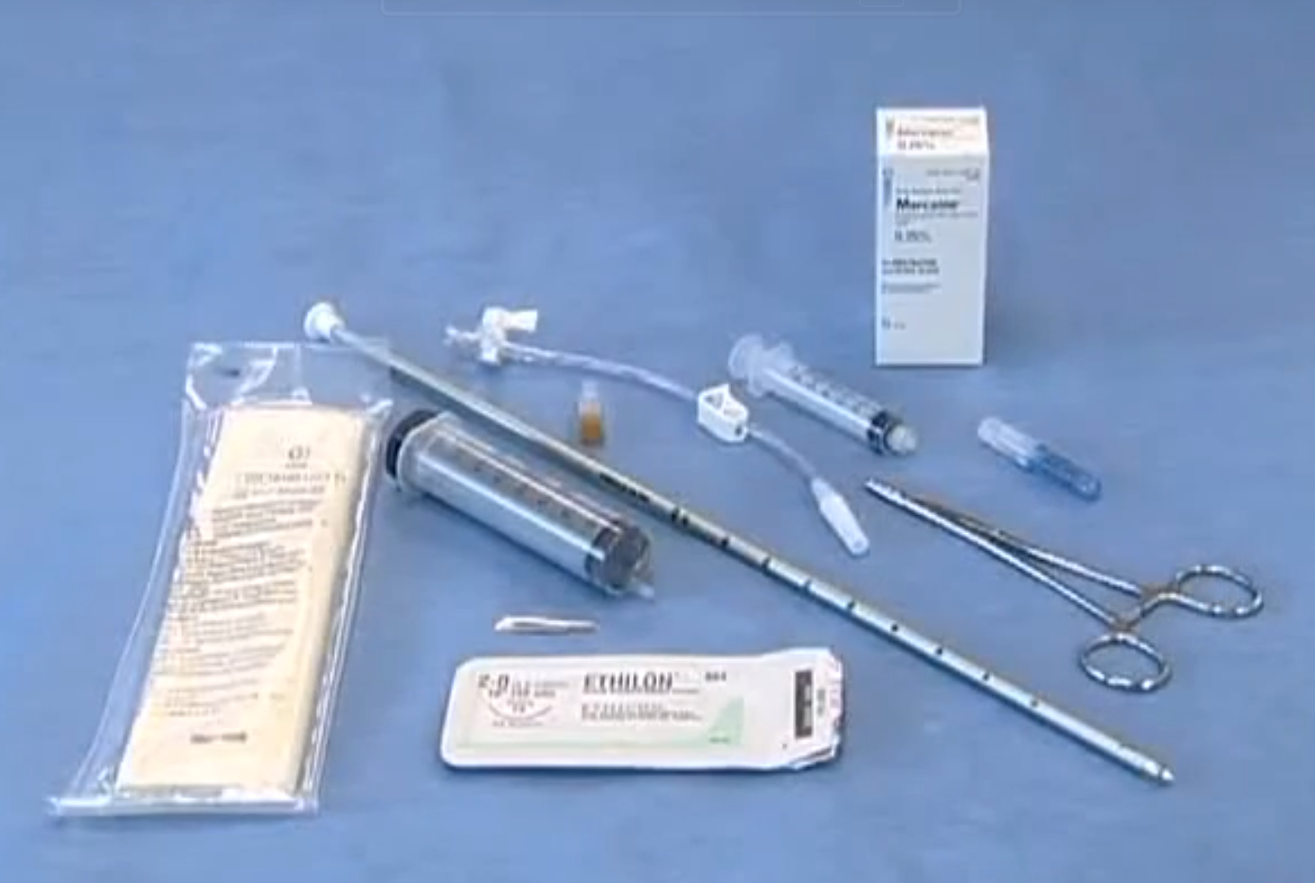
In order to place a Trochar chest tube, you will need ..
→ Sterile gloves
→ A sterile chest tube
→ A chest tube adaptor with a clamp
→ A syringe to aspirate any fluid or air which may have accumulated within the chest cavity
→ Suture material in order to secure the tube to the chest wall
→ A syringe to administer local anaesthetic
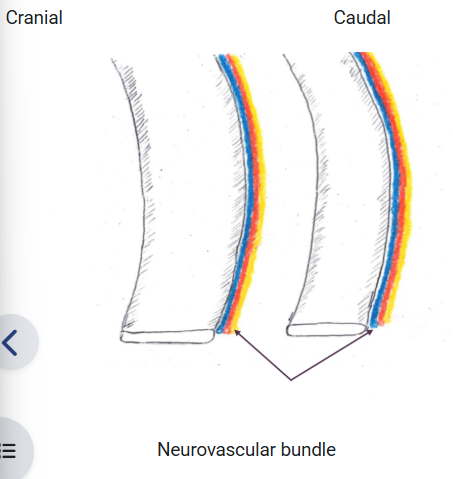
When placing a thoracic drain, it must be remembered to insert the drain ..
At the cranial border of the rib as neurovascular bundle runs at the caudal border of the ribs
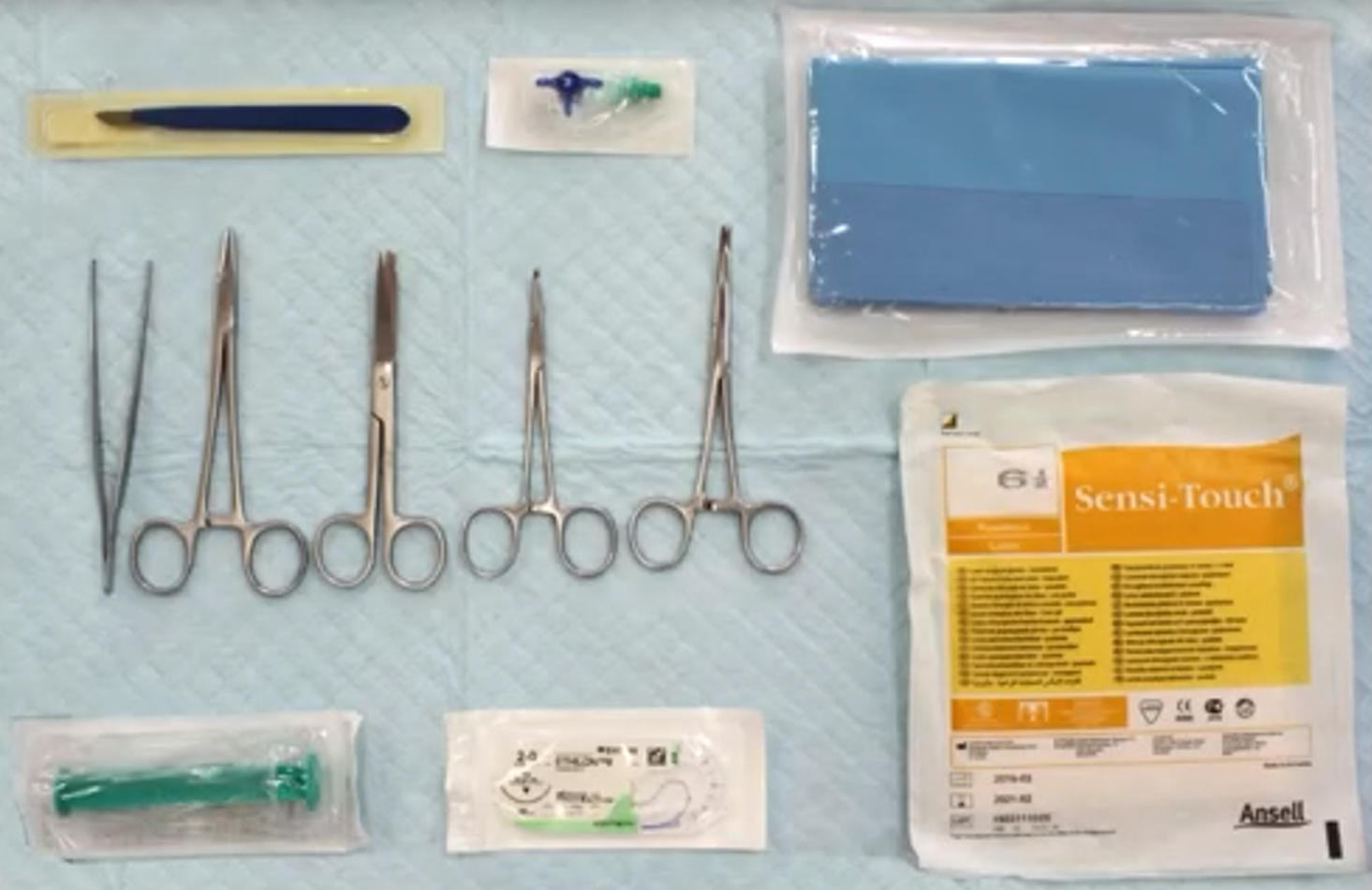
In order to place a chest tube using the seldinger technique, the equipment needed is ..
→ Scalpel
→ Forceps
→ Needle holder
→ Scissors
→ Curved forceps
→ 3-way tap
→ Sterile drape
→ Sterile gloves
→ Syringe
→ Suture material
Patient preparation when using the Seldinger Technique
Clip fur from last rib to shoulder
Prepare skin surgically
Checking the placement
Thoracic radiographs are taken to ensure correct placement of the thoracic tube
The tip should sit around the 2nd intercostal space
Dressing the drain
The thoracic drain will be secured in place using a purse string suture followed by a Chinese finger-trap suture (also know as a Roman Sandal suture)
It is then dressed to protect both the skin would and the drain itself
A sterile dressing (e.g. primapore) is placed around the entry site and then secured with with a body bandage, stockinette dressing or medical pet shirt to keep the drain close to the body - this protects the drain from getting dirty and getting damaged by the patient
The patient should wear a buster collar at all times
Drainage can be intermitter or continuous on the rate of fluid/air build up
→ Intermittent - Three way tap
→ Intermittent or continuous - Heimlich valves, Underwater seals
→ Continuous - Grenades, Suction
Intermittent Drainage
This is one of the most common techniques used for the drainage of thoracic drains in veterinary practice
Following a thoracotomy, drainage is usually carried out every hour for the first 4 hours and then reduced as necessary → this helps monitor for any post-op bleeding or air ‘leaks’.
The frequency of drainage is determined by how fast the fluid/air accumulates and the patient’s condition
The most commonly seen technique is using a syringe and 3-way tap
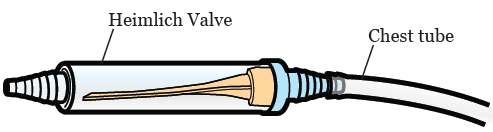
Intermittent OR continuous drainage - Heimlich valve
A portable device which consists of a clear plastic tube containing a rubber one-way flutter valve. It can be connected to the chest drain to allow intermittent drainage or left to function by itself and expel air/fluid during expiration
The plastic casing is quite brittle so can be prone to damage. The valves often become stuck ‘closed’ when draining thicker material, for this reason, they are mainly used for cases of pneumothorax
These devices do not allow measurement of the quantity of material aspirated so monitoring progression of the condition is difficult
Its use is reserved for large dogs/horses the valve does not allow adequate expulsion of air/fluid or animals <15kg
Intermittent OR continuous drainage - Underwater seal
This system uses a series of bottles/plastic compartments to allow drainage of the pleural space
They can be used for intermittent or continuous depending whether they are used with suction (3-bottle system) or without suction (2-bottle system)
These systems have been modernised and now come in a portable plastic form
Continuous drainage - Grenades
Can be attached to the thoracic drain to allow continuous drainage
It is compressed when attached then the negative pressure allows fluid to be drawn into the grenade
The fluid accumulates within the bulb therefore there is no need for a fluid trap
Suction can be applied to both the Heimlich valve the under seal to aid drainage
Most patients do not require this, however, when dealing with blood and tenacious fluid, it can be beneficial
A vacuum regulator should be used to ensure excessive pressure is not applied and therefore damaging the lungs
Nursing care
Veterinary nurses are heavily involved in the intermittent/continuous drainage of the thoracic drain
Nursing care - Dressing changes
Should be carried out 1-2 times daily
Aseptic technique should be used to do this as the opening has direct communication with the chest cavity so sterile gloves must be worn
The entry site of the drain should checked for any signs of infection (redness, inflammation, discharge)
The appropriate dressing should then be replaced (body bandage, stockinette or medical pet shirt)
Nursing care - Monitoring records
These patients require intensive monitoring and in the case of continuous drainage, this should be a dedicated nurse constantly monitoring the animals
This is because complication can happen more readily due to the increase in complicity of the equipment
Detailed record keeping is essential. Every time the drain is checked and drainage is carried out, the following should be record on the patients hospitalisation sheet ..
Time
Initials
Amount drained (try to include current rate of ml/kg/hr)
Colour/consistency is required
Comments - did the patient tolerate it? Any changes with the dressing?
When monitoring the patient, the following should have particular attention paid to:
Respiration → Changes in the rate, effort and patterns should be noted. This can indicate pin, hyperventilation (mainly due to effusion/air build up) or pyrexia
Cardiac → Pulse rare and quantity can give us an idea of pain and circulatory status
Mucous membranes → Cyanotic mucous membranes can indicate low oxygen saturation and pale mucous membranes may signify a bleed
Oxygen saturation → This can be measured using pulse oximetry. You should aim for >95% in these patient. If the SP02 is between 90-95% then oxygen supplementation should be given. <90% SP02 indicates a critical level of oxygen saturation
Temperature → Pyrexia can indicate infection, pain etc ..
Pain score → Having a chest drain in-situ, as well as the underlying pathology, can be painful so ensuring the patient is comfortable is vital
Nursing care - Pain relief
The patient will often require a combination of an opioid (buprenorphine/methadone) and a non-steroidal anti-inflammatory (e.g meloxicam)
Local anaesthetic may also be administered via the thoracic drain, especially after a thoracotomy
Nursing care - Positioning
Ideally these patients should be maintained in sterile recumbency, if possible, to optimise lung capacity
However, if the patents has a sternotomy (incision made through the sternum) then laying on this area will be uncomfortable so these patients can be laid in lateral recumbency but should be turned every 2-4 hours
Turning the patient helps to ensure lung capacity is maintained bilaterally but also helps to avoid pressure sores etc ..
Some patients may have an intercostal thoracostomy (incision made through the intercostal muscles)
In these cases, the side of the chest with the incision tends to be kept uppermost to encourage re-expansion however, they should also be turned intermittently until they are able to remain in sternal
Nursing care - Bedding
Deep comfortable bedding should be used. A waterproof liner followed by bedding that will help wick fluid away, e.g. vetbed, is recommended. Foam wedges and sandbags can be used to aid positioning
Nursing care - Nutrition
Adequate nutrition is vital in ensuring the patient’s RER is met. This may be done orally or via a feeding tube. Some attention should be paid to the underlying pathology as the nutritional needs may differ
Nursing care - TLC
Ensuring the patient is calm, keeping them warm and ensuring adequate toilet breaks/urinary catheter care can all help in the recovery of these patients
Removal of the Thoracic Drains
Drains can be kept in-situ until the fluid/air being drained is deemed to be at an acceptable level
The presence of the drain itself will create some inflammation of fluid formation therefore a level of less than 2ml/kg/day is used at a target or if no air has been drained for 12-24 hours
Once the veterinary surgeon is happy that the patient is stable and no longer requires the drain, the finger trap suture is cut and the drain is carefully withdrawn. If a purse string suture has been pre-placed, this can then be tightened and a sterile dressing placed over the wound
Complication of Thoracic drains
Complications have been noted as high as 58% with large bore drains. They occur as all stages of care and the risk can be minimised by careful technique and close monitoring
Complication of Thoracic drains during placement
Inadvertent damage to the lungs when the Trochar is placed can occur if it is advanced too far
Haemorrhage from damage to blood vessels by the Trochar (neurovascular bundles run on the caudal borders of the ribs)
Complications of Thoracic drains when in-situ
The tube can become blocked or kind therefore causing obstruction
Iatrogenic pneumothorax occurs if the clamp or 3-way tap is left open, allowing ait to move into the chest. This can also occur due to migration of the tube (allowing the drainage holes to move out of the chest) of damage to the drain by the patient
Cellulitis and infection at the skin would would can cause pain and discomfort. The risk of minimised by using gold-standard aseptic technique when handling the drain and dressings
Ascending infection can occur from bacteria at the skin entry point tracking along the tube and into the chest cavity, causing an iatrogenic prothorax
On rare occasions, cardiac arrythmias, phenic nerve irritation and Horne’s syndrome can be caused by migration of the tube at the cranial end coming into contact with the vagosympathetic trunk and the phrenic nerve
Complications of Thoracic drains - After removal
Pneumothorax can occur if the skin wound is not closed adequately, allowing air to track into the thoracic cavity
Recurrence of the effusion/air if the drain is removed too early