Folate and Vitamin B12 Assessment
1/91
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
92 Terms
What is folate (B9)?
refers to a family of structurally related water soluble vitamins
compounds can be interconverted with each other
What is folate crucial for (5)?
DNA synthesis
cell division
amino acid metabolism
producing RBCs
preventing neural tube defects
What are sources of folate (3)?
dark leafy greens
fruits
nuts and legumes
fortified grains and whole grains
liver
since water soluble, can be loss during cooking, hence why often it is preferred that these foods are steamed
What kind of deficiency is marked by a microcytic RBC? macrocytic RBC?
microcytic: iron deficiency
macrocytic: B12 or folate deficiency
How did we discover folate?
discovered folate through marmite
was able to cure macrocytic anemia with marmite
What is folic acid?
folic acid is the stable synthetic version used in supplements and fortification
tends to be better absorbed than folate from food sources
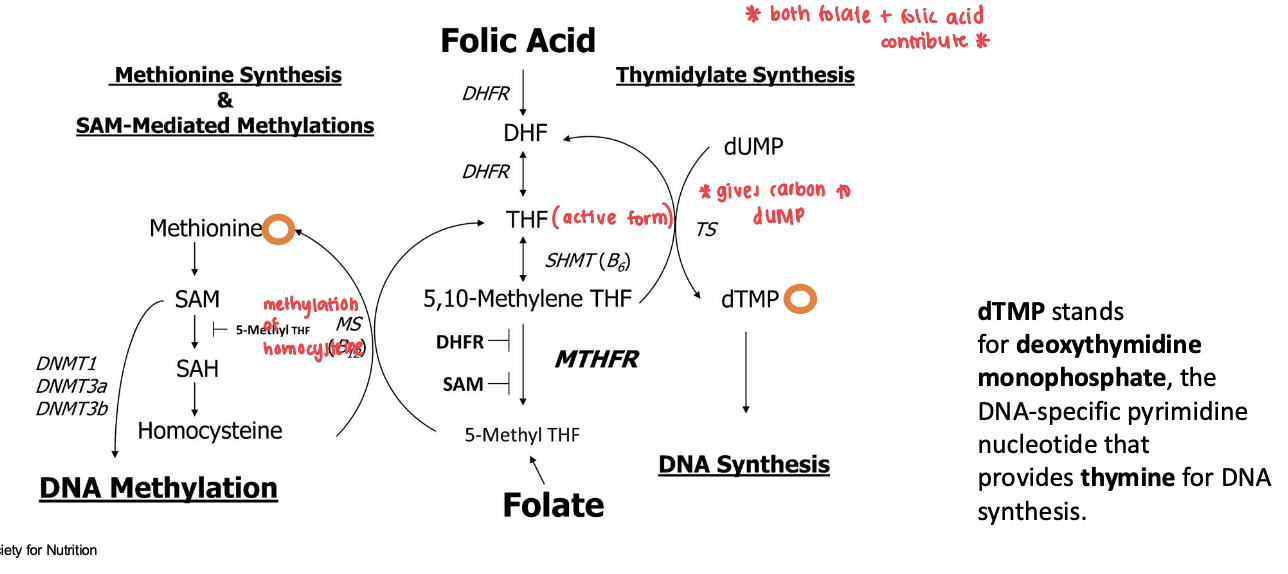
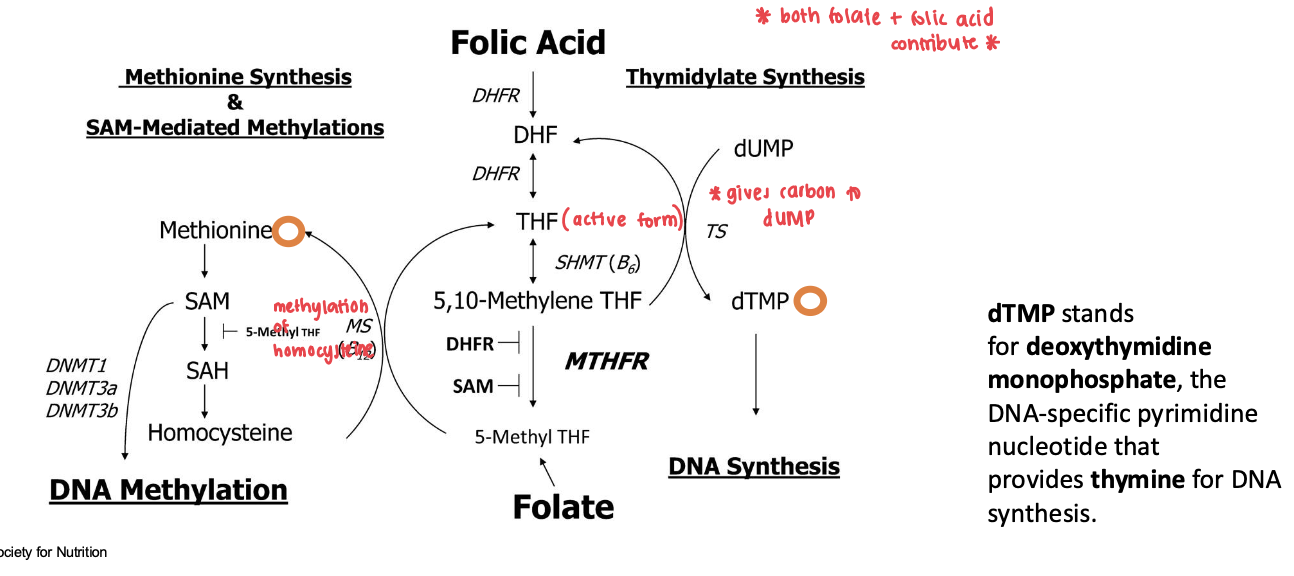
What are the three different roles that folate has when it comes to accepting/donating single carbons (one carbon metabolism)?
DNA synthesis
DNA methylation
Amino Acid Metabolism
What are the three components of folate?
pteridine
paba
glutamate (relevant for tail)
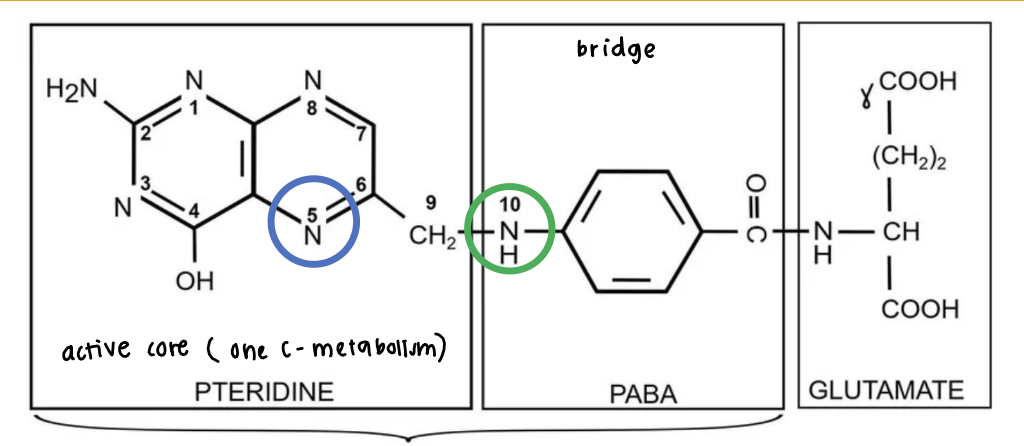
C5 and C10 are the carbons with different R groups that specify the specific folate compound we have
In terms of tails, what are two different types of folate?
polyglutamates
monoglutamates
Characteristics of folate with polyglutamate tails?
makes up 90% of natural food folates
active form
can have up to 9 glutamate residues
Characteristics of folate with monoglutamate tails?
absorbable form of folate
folic acid is an example of a monoglutamate
What R groups are added on C5 and C10 in order to make tetrahydrofolate (THF) and 5-methyltetrahydrofolate (5-MTHF)?
THF:
C5 = H
C10 = H
5-MTHF
C5 = CH3
C10 = H
Role of 5-MTHF? THF?
5-MTHF = used for transport and is the circulating form in plasma
THF = active metabolic form
both can be either polyglutamated or monoglutamated
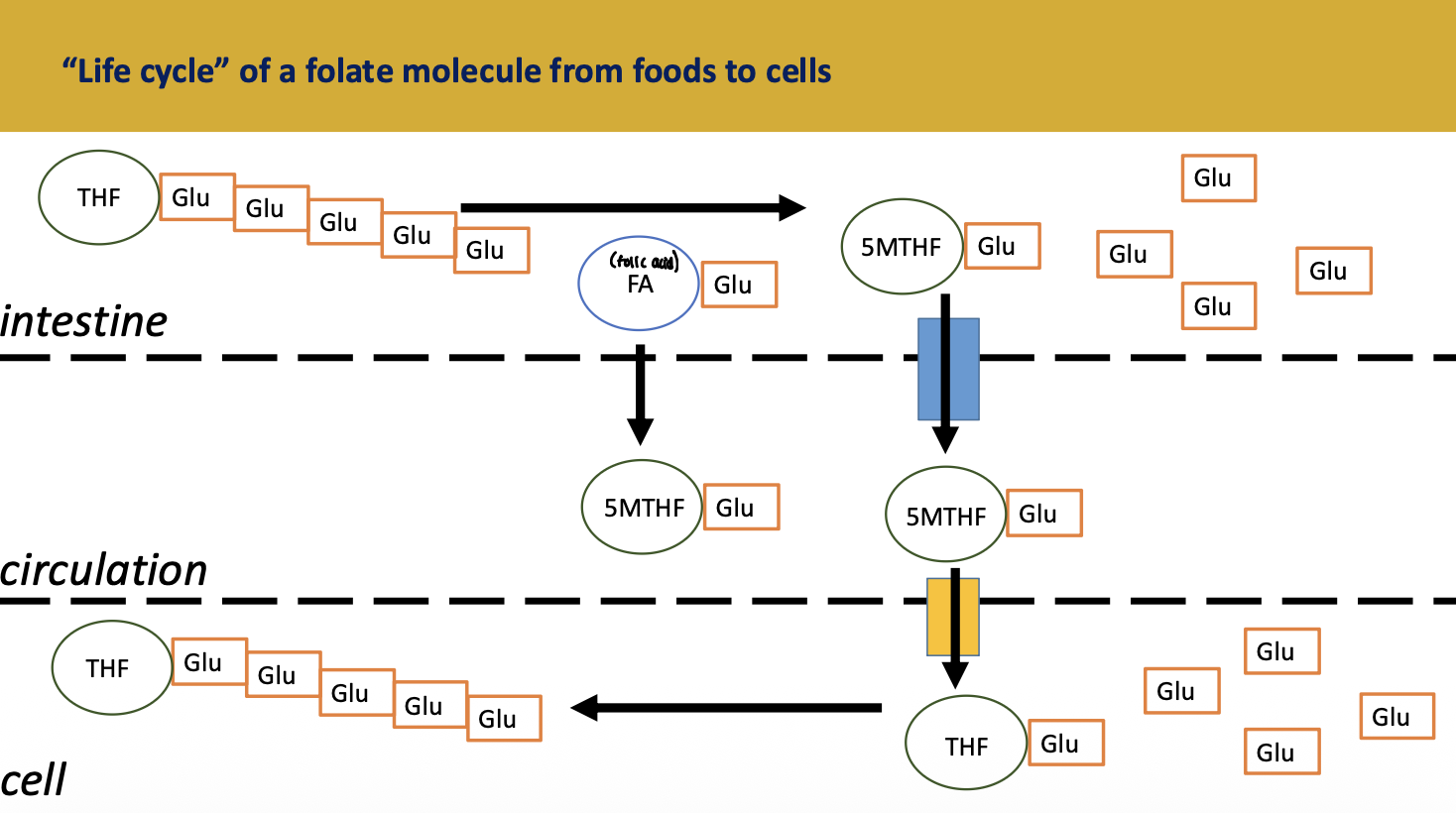
Describe the life cycle of a folate molecule from foods to cells.
folate in foods and side cells are in the polyglutamate form aka the active form (both 5-MTHF and THF) that is not easily absorbed
intestinal absorption of folate requires hydrolysis to monoglutamate specifcially 5-MTHF monoglutamate
5-MTHF monoglutamate is circulating in the plasma and gets transoprted inside cells
5-MTHF monoglutamate drops its methyl group in the cell and becomes THF monoglutamate
THF monoglutamates are converted back to the active polyglutamate form in the cell
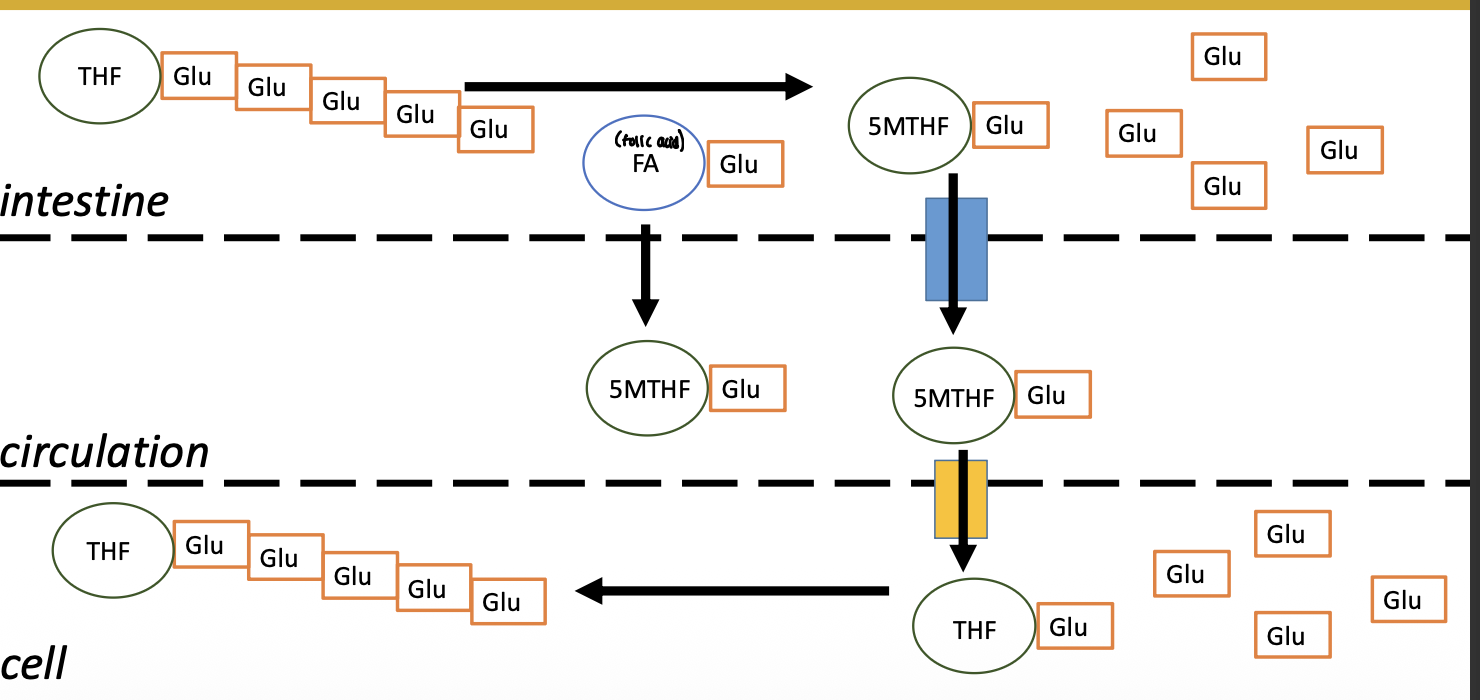
Describe the life cycle of folic acid into cells?
folic acid monoglutamate is easily abosrbed
gets reduced to THF by dihydrofolate reductase monoglutamate
inside the cell, THF monoglutamate turns into polyglutamate
Why does the glutamate tail of folate change?
polyglutamate tail is needed to trap folate in cells and increase its function
the monoglutamate form is needed for absorption and circulation
Why is folate measured in dietary folate equivalents (DFE)?
in order to account for differences in absorption
1 microgram food folate (50% absorbed) = 1 microgram DFE
1 microgram folic acid (100 absorbed) = ~1.7 microgram DFE
What are some causes for folate deficiency/low folate status?
inadequate intake (leading cause)
increased requirements (pregnancy or disease)
decreased availability (malabsorption)
alcoholism
certain medications interfere with folate metabolism (anticonvulsants/metformin used for T2DM, methotrexate used for cancer, and antimalaria medication)
What part of our body stores folate?
liver holds 50-90% of total body folate
several months worth
releases it as monoglutamates into blood and bile
What are two clinical consequences of folate deficiency or low folate status?
megaloblastic anemia
neural tube defects (spina bifida, anencephaly)
How does folate deficiency cause megaloblastic anemia?
when folate is low, proteins and RNA synthesis occurs but DNA synthesis slows or stalls
build up turns RBC precursors large, immature, and dysfunctional
Characteristics associated with neural tube defects?
high risk of mortality and disability
largely prevented by adequate folate in first 28 days of pregnancy
molecular mechanism unknown (likely DNA synthesis and methylation related)
not all neural tube defects are caused by folate deficiency
What is the recommended intake of folic acid before pregnancy?
400 micrograms folic acid/day before pregnancy
from supplements or fortified food
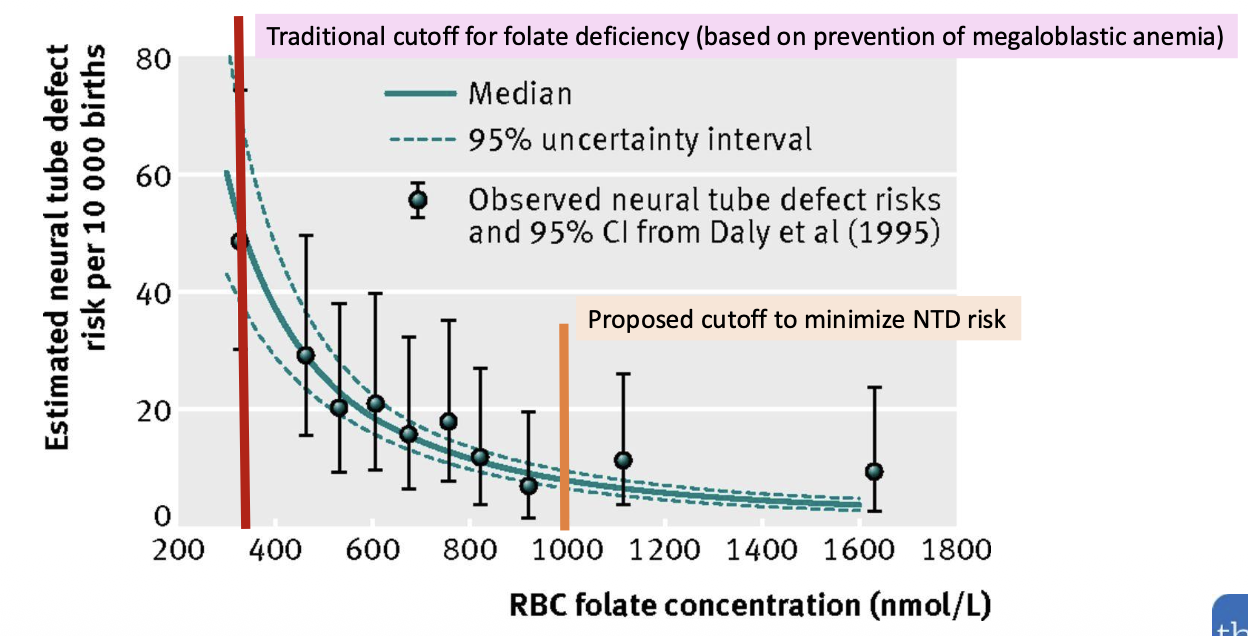
When we have folate deficiency, what clinical consequence occurs first?
increased risk for neural tube defects is thought to occur before megaloblastic anemia develops
cutoff depends on what outcome you are trying to prevent
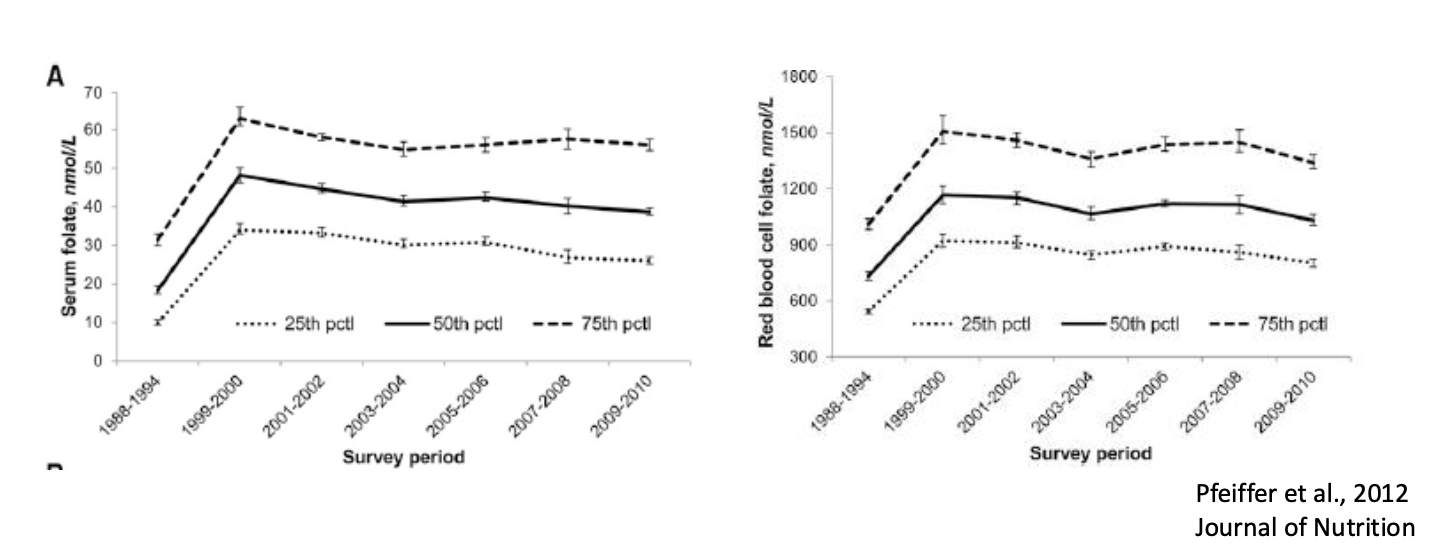
What happened in 1998 that caused such a drastic change in serum/RBC folate levels?
The US mandated folic acid fortification of enriched grain products (flour, bread, pasta, and cereal) starting January 1, 1998
What statement on folate is incorrect?
the active form of folate is THF
the body absorbs food folates much more efficiently than folic acid
neural tube defects are responsive to folic acid but not exclusively due to folate deficiency
marmite is an excellent source of folic acid
the body absorbs food folates much more efficiently than folic acid
Describe the role of folate in one carbon metabolism.
What are three clinical measures of folate?
serum/plasma folate
RBC folate
homocysteine
Describe the changes you would see (from first to change to last) when assessing someone with folate deficiency.
FIRST TO CHANGE
low dietary folate
low serum folate
low RBC folate (due to decreased folate stores and thus low folate available for erythropoiesis)
increased homocysteine
macrocytic red blood cells
hypersegmented neutrophils (neutrophiles with increased nuclear lobes/nuclei)
megaloblastic anemia
LAST TO CHANGE
How do we measure plasma/serum folate?
a patients blood is taken after a fast and plasma/serum is isolated and multiple tests can be used to measure the concentration
folate is sensitive to oxidation so must protect samples from air, light, heat, and or add antioxidant to samples (ascorbic acid)
What are the three different test we can use to measure plasma/serum folate?
microbiological assay
competitive protein binding assays
LC-MS/MS
Characteristics of microbiological assays when it comes to measuring plasma/serum folate?
bacterial growth tends to be proportional to the amount of folate in media
specific bacteria can utilize multiple forms of folate
Characteristics of competitive protein binding assays when it comes to measuring plasma/serum folate?
Competitive binding assays determine how strongly a test substance binds to a target (like an antibody or receptor) by measuring its ability to displace a known, labeled molecule from that target. It is an inverse relationship: more unlabeled test substance means less labeled molecule binds
linked to a detection system
ex: radioassay, chemiluminescent tags
Characteristics of LC-MS/MS when it comes to measuring plasma/serum folate?
expensive
can detect different forms of folate
What are some characteristics of plasma/serum folate levels?
reflects recent intake
not a long term marker or marker of folate stores
primary form in plasma is 5-MTHF
What are three factors that increase serum folate?
hemolysis (release folate from RBCs)
non fasting status due to a recent meal
renal failure or liver disease
What are four factors that decrease serum folate?
chronic alcohol consumption (inflammation leads to less absorption)
cigarette smoking
oral contraceptive use
some medications (anti-inflammatory, asthma, anti-convulsants)
How do we measure RBC folate?
collect blood
hemolyze RBC with 1% ascorbic acid
convert polyglutamates to monoglutamates (assay is calibrated to detect monoglutamates)
use lysate in microbiological assay (same as serum/plasma folate)
Is RBC folate or serum/plasma folate a better marker of folate stores?
RBC folate is considered better bc it is less sensitive to short term changes in diet and reflects status at the time the cells are produced (between 1-100/120 days ago)
RBCs take up folate during erythropoiesis and retain this folate in the polyglutamate form
primary biomarker used by the US Institute of Medicine to set DRIs as it is highly correlated with liver foalte stores
What is used for frequently as a biomarker, serum/plasma folate or RBC folate?
serum/plasma
RBC folate is used less frequently because it is less easy to automate, have to hemolyse AND turn into monoglutamate
Is RBC folate affected by recent dietary intake?
no, not affected by recent dietary intake
What can impact RBC folate measurements?
if hemolysis occurs during blood collection
lowers the measured number of RBCs and hematocrit, however it doesn’t change how much folate was inside the cells
will have an overestimation per RBC
Which of the following statements is correct?
RBC folate reflects recent dietary intake
serum folate reflects long term tissue stores
serum folate reflects recent dietary intake, while RBC folate reflects long term tissue stores
both measures provide identical information and are interchangeable
serum folate reflects recent dietary intake, while RBC folate reflects long term tissue stores
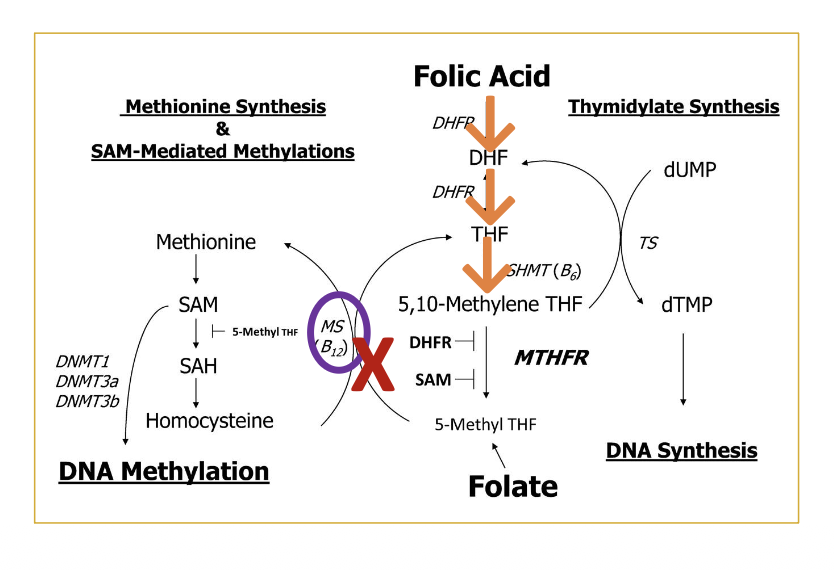
How is homocysteine modulated by folate?
a decrease in folate will cause a decrease in 5-MTHF, which doesn’t allow homocysteine to be methylated into methionine
results in homocysteine build up
Why is homocysteine build up bad?
elevated homocysteine (hyperhomocysteinemia) is considered toxic and is linked to multiple health problems such as atherosclerosis, dementia, and stroke, etc.
Besides folate, what are other factors that affect homocysteine concentrations in plasma (5)?
age, sex, pregnancy status
recent meal
sample storage (leakage from RBCs)
alcohol, caffeine, cigarettes may increase it
folate/b12 deficiency
Are homocysteine (Hcy) levels specific to foalte?
no
processes is also dependent on B12, so low availability in folate OR B12 will increase homocysteine which enters the plasma
Which step in folate metabolism is not reversible?
5,10 - methylene THF TO 5-MTHF
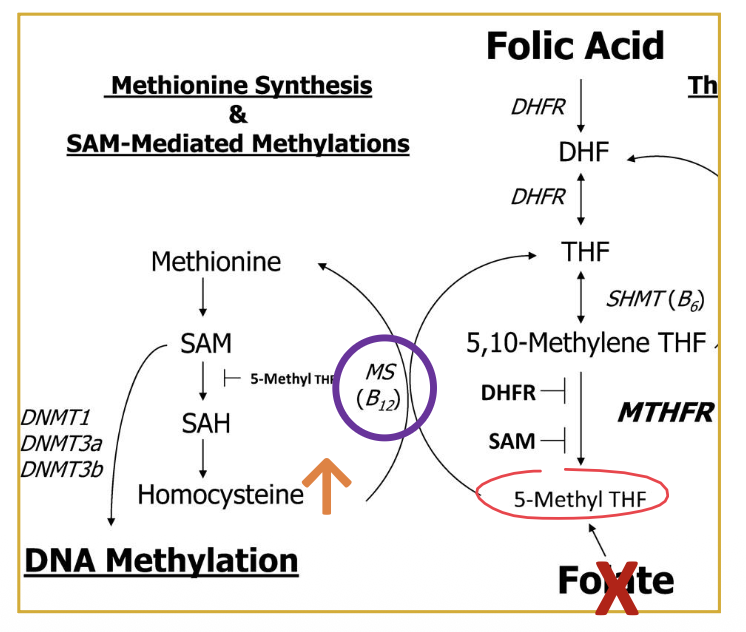
What is the methyl trap in terms of one carbon metabolism?
b12 deficiency leads to increased 5-MTHF
cant be cycled back into THF into 5,10-methylene THF which is relevant for DNA synthesis NOR can it methylate homocysteine
How common is folate toxicity?
folate toxicity is rare
water soluble, so it tends to be excreted in urine if there is an excess
excessive folic acid can be assessed via blood tests and symptoms if need be
What is important to note about the UL for folate?
UL is for folic acid only, not food folate
What is indicative of too much folate?
would measure “unmetabolized” folic acid in plasma/serum
few data is available to interpret concentrations, and even if there is, its not that much of a problem
affected by recent food intake
How does polymorphisms in genes related to folate metabolism affect folate status?
have some genes that reduce or increase the activity of MTHFR enzyme (turns 5,10-methylene THF into 5-MTHF)
What role does the C677T gene play? What role does the A1298C gene play?
C677T:
most impactful variant
people with two copies (TT) may have enzyme activity reduced by 60-70%
results in higher levels of homocysteine
A1298C:
milder effect
reduces enzyme activity by only 20%
Which form of folate is the only one that can donate a methyl group to homocysteine to produce methionine?
THF
5, 10-methylene THF
5-MTHF
folic acid
all of the above
5-MTHF
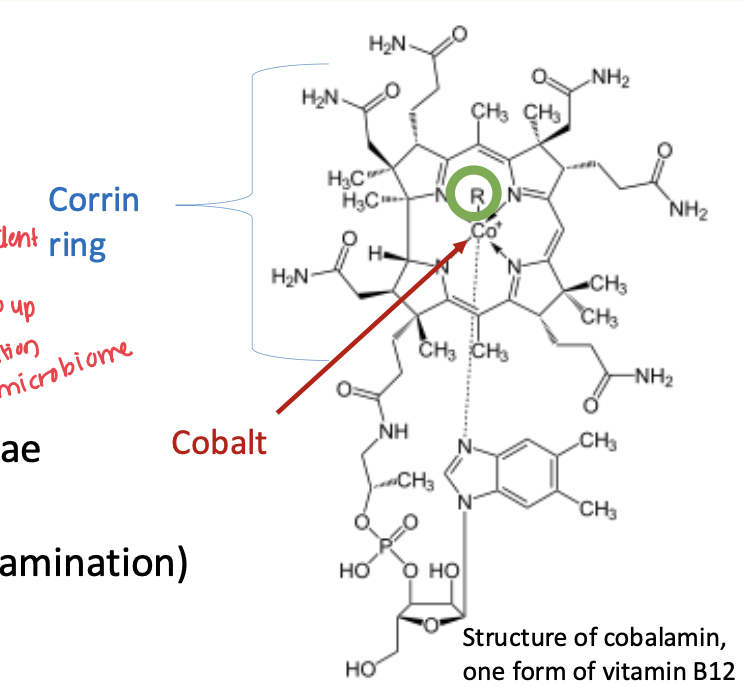
Characteristics associated with vitamin B12?
cobalt containing vitamin
two active forms
What are the essential roles of B12?
DNA synthesis
RBC formation
neurological function
What are the two active forms of B12?
methylcobalamin
5-deoxyadenosylcobalamin
What are some sources of B12?
found mostly in animal derived foods
meat
fish
eggs
dairy
fortified products (cereals and plant based milks)
gut microbes (minor contribution as they can be synthesized by bacteria, fungi, and algae)
Describe the structure of B12.
contains cobalt within a corrin ring
coenzyme present (R group) on cobalt, forms which ever structure of B12 it is
What is the role of methylcobalamin?
in cytosol
cofactor for methionine synthase in 1-carbon metabolism (helps turn homocysteine into methionine)
What is the role of 5’-deoxyadenosylcobalamin?
in mitochondria
cofactor for methylmalonyl-coenzyme A (CoA) mutase (helps turn methylmalonyl-CoA into succinyl-CoA
works independent of folate
What are two consequences of vitamin B12 deficiency?
megaloblastic anemia (due to reduced DNA synthesis)
neurological damage
How does B12 deficiency result in neurological damage?
myelin loss resulting in axonal degeneration
tingling/prickling (weakness, lack of coordination, dementia)
irreversible
impacts myelin related mitochondrial metabolism as it makes methylmalonyl-CoA mutase fail
impacts odd chain fatty acid handling accumulation
What are two general causes of B12 deficiency?
low intake (primary): vegetarian/vegan diets
malabsorption (secondary): problem with absorption and or utilization
Can B12 deficiency be treated with folic acid supplementation?
Yes, to an extent
folic acid can bypass the B12 deficient blockage when it comes to DNA synthesis specifically thymidylate/purine synthesis (could resolve megaloblastic anemia)
neurology worsens/unchecked: DNA methylation is still impacted and broken and mitochondrial toxicity continues (accumulation in odd chain fatty acids which results in demyelination AND methylmalonyl-coA mutase fails
would result in the development of wheelchair bound myelopathy years later
Is the rate of loss for folate or B12 higher?
rate of folate loss is higher than for B12
folate stores: 3-4 months
B12 stores: 3-5 years or longer
How long does it take for macrocytosis to develop due to foalte deficiency?
3-4 months
How long will it take for B12 deficiency to be severe enough?
years
neurological consequences of B12 deficiency also develop slowly over many years (may not be noticeable)
Which of the following conditions can lead to a functional folate deficiency even if a person’s dietary folate intake is adequate?
excessive consumption of leafy greens
vitamin B12 deficiency
high intake of vitamin C
lack of dietary iron
vitamin B12 deficiency
What does B12 absorption rely on?
intrinsic factor
binds B12 in the small intestine, complex is absorbed in the terminal ileum
no IF could lead to pernicious anemia
Describe the three steps in B12 absorption.
stomach: parietal cells release acid (activating pepsin) and IF, the activated pepsin degrades the food proteins and releases B12 so that it can bind to haptocorrin (transcobalamin I/TC I)
duodenum: haptocorrin gets degraded by trypsin from the pH increase, this free B12 then binds to IF
terminal ileum: IF-B12 complex is taken up by an IF receptor on an epithelial cell (cubulin), this releases B12 into circulation and binds to holo TC II (transcobalamin II)
How does B12 get recycled?
via enterohepatic circulation
secretes B12 into bile from the liver, this gets sent to the intestines and then reabsorbed
B12 reserves can last 2-5 years
How is B12 found in circulation/blood?
attached to holo TC II (transcobalmin II)
What is the role of trancobalamin II (TCII)?
delivers B12/cobalamin to cells through blood
most cells have specific TC II receptors and internalize the holo-TC II complex by pinocytosis
empty form = apoTC whereas active form = holoTC
10-30% of B12 in circulation
90 minute plasma half life
Characteristics of transcobalamin I (TC I/Haptacorrin)?
circulates in plasma
contains no cellular receptors
make up 70-90% of plasma cobalamin
half life of 9-10 days
What happens to B12 once it gets to cells via pinocytosis of trancobalamin II?
released from TCII and used as methylcobalamin in cytosol or taken up by mitochondria
What does cobalamin absorption depend on?
dose
only 2 micrograms can be absorbed by the IF system at one time (~50% of dietary B12), anything above this amount is less efficient
How long does it take for B12 to reach our bloodstream from ingestion?
~4 hours
What are two malabsorption cases that lead to B12 deficiency?
decreased acid production (achlorohydria)/pancreatic insufficiency
damaged to ileum (gut inflammation)
What are some characteristics associated with achlorohydria/pancreatic insufficiency that causes malabsorption of B12?
can be caused by atrophic gastritis (chronic inflammation of the stomach lining)
would get impaired secretion of HCl, pepsin, and IF
increased risk with age
associated with helicobacter pylori infection
What is pernicious anemia?
subtype of B12 deficiency anemia
autoimmune cause, as the immune cells are destructing IF
can also obtain antibodies against parietal cells and IF receptor
Which part of the digestive tract is the primary site where B12-IF complex is absorbed into the bloodstream?
terminal ileum
What are the different clinical markers for B12 status?
serum/plasma B12
RBC B12 (not commonly used)
holo-haptocorrin (holo-HC: not commonly used)
holo-transcobalamin II (holo-TC II)
urinary/serum methylmalonic acid (MMA)
homocysteine (Hyc)
What is the clinical gold standard biomarker for understanding B12 status?
no clinical gold standard, make use of a combine B12 indicator instead (CB12)
score that combines plasma B12, holoTC, MMA, and Hcy
What impact does B12 have on MMA production?
inverse relationship, B12 deficiency = high MMA (> 270pmol/L)
5'‘-deoxyadenosylcobalamin acts as a coenzyme for methylmalonyl-CoA mutase (turns methylmalonyl-CoA into Succinyl-CoA, however, when inhibited it produces methylmalonic acid (MMA)
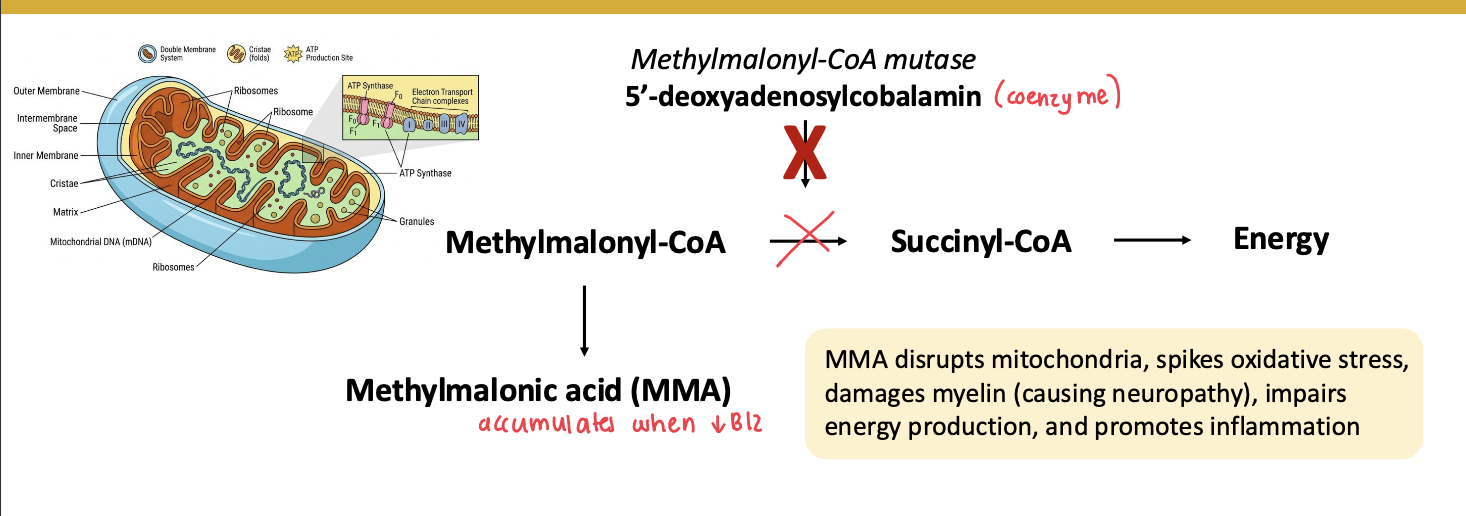
What are some characteristics of methylmalonic acid (MMA)?
has no beneficial role and is toxic
disrupts mitochondria
spikes oxidative stress
damages myelin causing neuropathy
impairs energy production
promotes inflammation
renal insufficiency can increase MMA levels
Describe the changes in biomarkers for B12 from first to change to last.
FIRST
low vitamin B12 intake/reduce absorption
decreased liver stores
decrease in serum/plasma B12
decrease in holo-TC II
increase in MMA
increase in Hcy
neurological damage
macrocytic cells
anemia
LAST
typically occurs more slowly than for folate, due to liver B12 stores and low losses of B12
What are three different laboratory techniques to measure serum/plasma B12?
competitive binding immunoassays
microbiological assay
HPLC/liquid chromatography
fasting is generally not required for any except for CB12 value
Characteristics of using competitive binding immunoassays to determine serum/plasma B12?
most common
uses IF or analogs to bind free B12
Characteristics of using microbiological assays to determine serum/plasma B12?
gold standard for accuracy
labor intensive
measures functional B12 via bacterial response from Euglena gracillis
Characteristics of using HPLC/liquid chromatography to determine serum/plasma B12?
separates and quantifies B12 forms precisely with MS
used for research
expensive