Lecture 5: Personality Disorders
1/58
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
59 Terms
personality
Characteristic way of behaving, experiencing life and of perceiving and interpreting themselves, other people, events and situations
Relatively stable over time
Relatively stable over situations
Cognition, emotion, behaviour
The Big Five
Openness <-> Traditionalism
Conscientiousness <-> Headlessness
Extraversion <-> Introversion
Agreeableness <-> Antagonism
Neuroticism <-> Emotional stability
Personality disorder
Enduring problems with forming a stable positive identity and sustaining close and constructive relationships.
Personality traits are:
Extreme
Inflexible/rigid
Dysfunctional
Typically: ego-syntonous (vs. ego-dystonous)
Cf. phobia vs OCPD
Differential diagnostics
Other PD, autism, mental retardation, chronic syndrome disorder, circumstances
DSM IV (axis removed from DSM-5):
Axis I: Syndrome disorders
Axis II: Personality
DSM general criteria for personality disorders
An enduring pattern of inner experience and behaviour that deviates markedly from the expectations of the individual's culture. Manifests in 2+/4 domains:
Cognition
Affectivity
Interpersonal functioning
Impulse control
Pervasive: inflexible, across many different situations
Persistent: stable, long term, start early adulthood
Pathological: distress/dysfunction
Onset in early adulthood; not better explained by another substance/somatic/mental disorder…
Problems with DSM-5-TR approach to personality disorders
Not stable over time: ~50% don't meet criteria again after 2 years
In patients diagnosed with severe personality disorder, 99% don't meet criteria 16y later
Milder symptoms remain, but disorder are not as enduring as the DSM claims
PDs are highly comorbid: 50% have another PD; some involve similar symptoms
Arbitrary thresholds: number of symptoms is arbitrary; more of a continuum rather than yes/no, almost all disorders seem dimensional in nature
PD-NOS one of the most frequently used
ICD-11 switched to dimensional model
DSM disorders
Cluster A: 'odd, eccentric'
Paranoid PD - distrusting
Schizotypal PD - strange perceptions and behaviour; cognitive distortions, eccentric behaviour, lack of capacity for close relationships
Schizoid PD - distant; detachment from social relationships, restricted range of emotional expression
Cluster B: 'dramatic, emotional, erratic'
Antisocial - violating others' rights
Borderline - instability in self-image, relations, emotions; impulsivity
Histrionic - emotional, attention seeking
Narcissistic - inflated ego, need for admiration, lack of empathy
Cluster C: 'anxious, fearful'
Avoidant PD - socially inferior
Dependent PD - submissive, clinging
Obsessive-compulsive PD - perfectionistic, controlling
Other specified/unspecified PD; personality change due to medical condition.
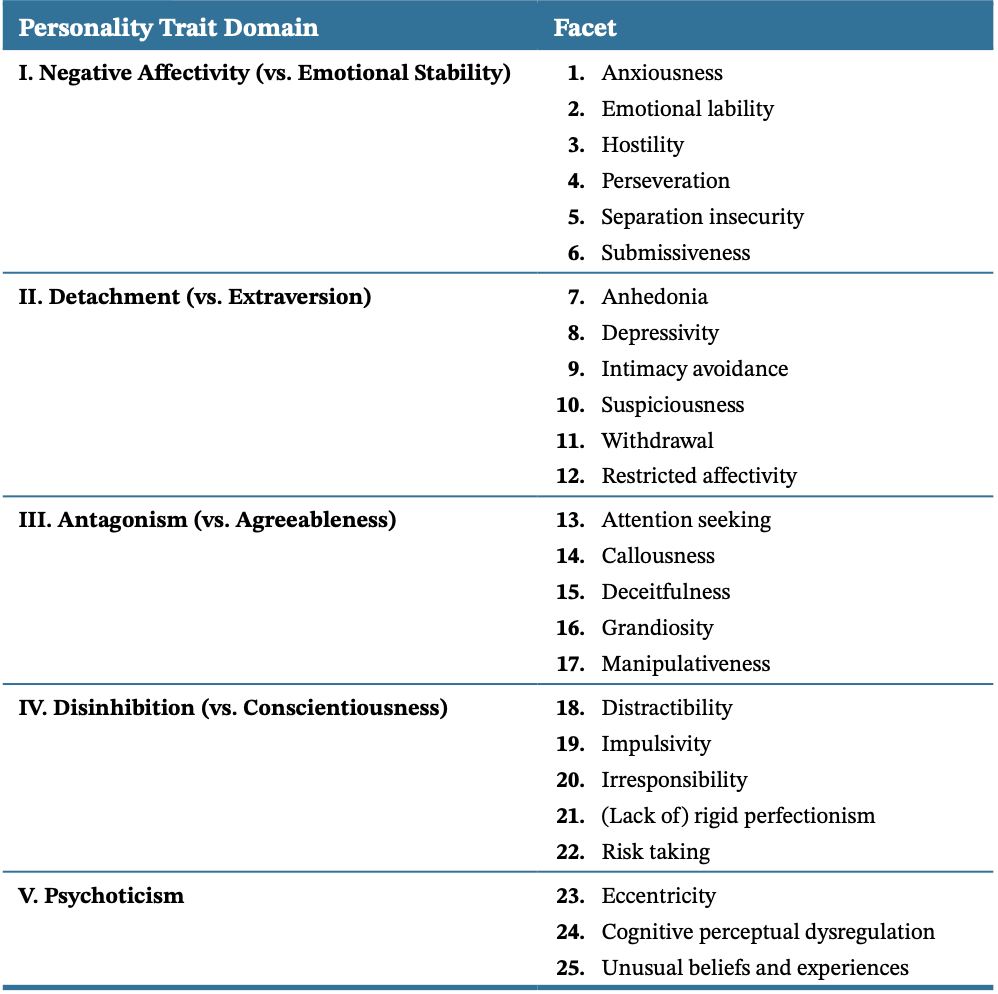
DSM Alternative model
DSM AMPD: hybrid
5 dimensions (clinical version of big 5)
25 facets
7 categorical classifications retained!
Strengths:
Ratings more stable over time than PD diagnoses
Richer detail than categorical PDs
Related to many psych. disorders
Robustly predict outcomes like happiness, relationship quality, stress, occupational outcomes, physical health, life expectancy
More useful in communicating with clients and planning treatment
ICD-11 personality disorder
An enduring disturbance characterised by:
Problems in functioning of aspects of the self (identity, self-worth, accuracy of self-view, self-direction)
And/or
Interpersonal dysfunction (ability to develop/maintain close and mutually satisfying relationships, understand others' perspectives, manage conflict in relationships)
Severity level.
5 dimensions:
Negative affectivity (high neuroticism)
Detachment (low extraversion)
Dissociality (low agreeableness)
Disinhibition (low conscientiousness)
Anankastia (extremely high conscientiousness)
Specifier: Borderline Pattern
Epidemiology of PD
General population fit DSM classification: 9–13%
Outpatient care: 30–50%
Inpatient clinics: 50–70%
Prisons: 60–70%
Unstructured clinical interviews are not reliable, miss up to 50% of personality disorder diagnoses.
Consequences of PD
Treatable!
High disease burden
High consumption of care
Low QoL
High societal costs
Comorbidity of PDs
Other mental disorders; associated with worse symptoms
Other PD (50%):
Cluster B (e.g. antisocial + borderline)
Cluster C (e.g. dependent + avoidant)
Between clusters (e.g. borderline + dependent)
Other syndromal disorders:
E.g. avoidant + alcohol abuse; obsessive-compulsive PD + depression; borderline + PTSD; PD + anxiety/depression/addiction
How is personality produced?
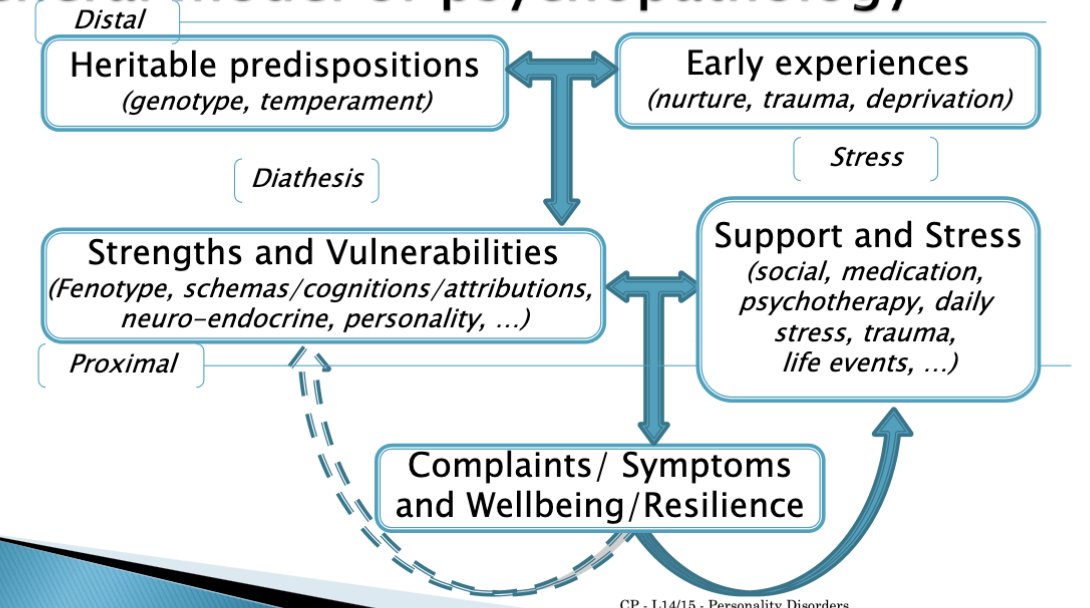
Aetiology
Early environment - adversity:
Abuse (didn't predict BPD after controlling for genetic risk; maybe parents with genetic vulnerability more likely to abuse)
Maltreatment
Aversive parental behaviour
Lack of parental affection
Neglect
Biology:
Heritability estimates: .35–.70
Shared between PDs
Neurotransmitter systems:
Dopamine (cognitive problems, cluster A)
Serotonin (anger, impulse control)
Mono-amine oxydase (MAO; agression)
Brain areas:
Lack of frontal cortical control: impulses and emotions (mid brain)
Dysfunction amygdala: hyper-emotionality, hypo-emotionality
Levels of description
Psychological:
Attachment
Attributional style
Coping styles
Process:
Cognitive biases (attention, interpretation)
Core assumptions/beliefs/schemas
Emotion regulation
impulsivity
Biological:
Endophenotypes:
Neural circuits: size, organisation, connectivity
Neurotransmitter systems
Neuro-endocrine (e.g. HPA-axis tuning)
A: Paranoid PD
Symptoms:
4+ of following signs of distrust and suspiciousness from early adulthood in many contexts:
Unjustified suspiciousness of being harmed/deceived/exploited
Preoccupation with unwarranted doubts about loyalty/trustworthiness of friends or associates
Reluctance to confide in others due to suspicion
Reading hidden meanings into benign actions of others
Bearing grudges for perceived wrongs
Angry reactions to perceived attacks on character
Unwarranted suspiciousness of partner's infidelity
A: Schizotypal PD
Bizarre thinking and functional impairments less severe than in schizophrenia
Symptoms:
A pervasive pattern of social and interpersonal deficits marked by acute discomfort with and reduced capacity for close relationships, as well as cognitive or perceptual distortions and eccentricities of behaviour, beginning by early adulthood and present in a variety of contexts, as indicated by 5+ of the following:
Ideas of reference (excluding delusions of reference)
Odd beliefs or magical thinking that influences behaviour and is inconsistent with subcultural norms (superstitiousness, belief in clairvoyance, telepathy, "sixth sense", children/adolescents - bizarre fantasies, preoccupations)
Unusual perceptual experiences, incl. bodily illusions
Odd thinking and speech (e.g. vague, circumstantial, metaphorical, overelaborate or stereotyped)
Suspiciousness or paranoid ideation.
Inappropriate/constricted affect
Behaviour/appearance that is odd, eccentric or peculiar.
Lack of close friends or confidants other than 1st degree relatives.
Excessive social anxiety that does not diminish with familiarity, associated with paranoid fears rather than negative judgements about self.
Does not occur exclusively during the course of schizophrenia, a bipolar disorder or depressive disorder with psychotic features, another psychotic disorder or ASD.
schizotypy
Multigenetic vulnerability
-> Biochemical deviations
-> Neurobiological deviations (endophenotypes)
Enlarged ventricles, less temporal lobe gray matter, neurotransmitter dysregulation
Vulnerability -> Schizotypal traits and/or
Psychotic decompensation: psychotic disorders, schizophrenia
There might be protective factors🤯.
~1/3rd of people diagnosed with schizotypal PD later diagnosed with schizophrenia
A: Schizoid PD
Low inter-rater reliability
Symptoms:
4+ of the following signs of aloofness and flat affect from early adulthood across many contexts:
Lack of desire for/enjoyment of close relationships
Prefers solitude to companionship
Little interest in sex
Few/no pleasurable activities
Lack of close friends
Indifference to praise/criticism
Flat affect, emotional detachment or coldness
B: Antisocial PD
5 times more likely in men🤯
3/4ths meet criteria for another disorder (commonly SUD)
>50% of prison inmates
Irresponsible behaviours: working inconsistently, breaking laws, being irritable, physically aggressive, defaulting on debts, being reckless, impulsive, not planning ahead
Little regard for truth, little remorse for misdeeds
APD: symptoms
Age 18+
Conduct disorder before 15
From 15, pervasive pattern of disregard for others' rights, indicated by 3+ of the following
Repeated engagement in illegal behaviours
Deceitfulness, lying
Impulsivity
Irritability and aggressiveness (for example, repeated physical fights or assaults)
Reckless disregard for own safety and that of others
Irresponsibility (unreliable employment or financial history)
Lack of remorse
APD: causes
Gene-environment interaction:
Genetic vulnerability for APD overlaps with SUD
Social environment plays major role in genetic expression of vulnerability
Poverty, exposure to violence
In adolescents with conduct disorder, impoverished are 2x more likely to develop APD
psychopathy
Subgroup of APD (15–25%) is also 'psychopathic':
Measure: Psychopathy Checklist - revised (PCL-R); evaluation of interview by therapist + facts (file)
Factor 1: Affect/Interpersonal (callous/unemotional, glib)
Factor 2: Behaviour (antisocial, impulsive)
Psychopathy:
Lack of positive/negative emotions
Superficial charm, used to manipulate others for personal gain
Lack of anxiety -> don't learn from mistakes
Lack of remorse -> behave cruelly toward others, impulsively
Triarchic model of psychopathy:
Three core traits underpin symptoms of psychopathy:
Boldness (fearlessness)
Meanness (aggression and lack of remorse)
Disinhibition (impulsivity)
differences between APD and psychopathy
PCL-R doesn't include affective symptoms, like shallow affect and lack of empathy
DSM criteria for APD require symptoms before age 15
APD is categorical, psychopathy is dimensional
risk for psychopathy
Threat sensitivity: deficits linked to boldness
High boldness <-> less reactivity in GSR and heart rate to aversive stimuli
Low GSR to aversive stimuli at 3 predicts psychopathy at 28
Blunted neural responsivity to aversive stimuli in psychopaths
Psychopaths don't learn to stop misconduct from punishment because they are insensitive to threats
High psychopathy <-> diminished classical conditioning when CS paired with aversive stimulus
No (expected) increase in amygdala activity
Lack of empathy (capacity to share emotional reactions of others): linked to meanness
Men with psychopathy poor recognition of others' fear, other emotions well
People with APD show less amygdala response when imagining others' pain compared to their own
vmPFC, involved in processing social and moral info and in conditioning, less active in psychopaths
Disruptions in amygdala-vmPFC connectivity when viewing others' fearful expressions predicted psychopathic traits
B: Histrionic PD
5+ of the following signs of excessive emotionality and attention seeking from early adulthood across many contexts:
Strong need to be centre of attention
Inappropriate sexually seductive behaviour
Rapidly shifting, shallow expression of emotions
Use of physical appearance to draw attention to self
Speech that is excessively impressionistic and lacking in detail
Exaggerated, theatrical emotional expression
Being overly suggestible
Misreading relationships as more intimate than they are
B: Borderline (BPD)
Drastic emotional shifts
Related to interpersonal hypersensitivity:
overly sensitive to small signs of rejection, prone to anger/aggression in response
Can't bear to be alone, fear of abandonment
Chronic feelings of depression and emptiness
Most closely tied PD to distress in romantic relationships
Transient psychotic/dissociative symptoms when stressed
Highly impulsive, particularly in response to emotion states -> gambling, reckless spending, indiscriminate sexual activity, substance abuse
Have not developed a clear, coherent sense of self - major swings in basic aspects of identity (e.g. shifting between careers)
Likely to attempt suicide; self-harm (2/3rds)
Adolescents diagnosed with BPD likely to not meet criteria when reassessed in adulthood
BPD: symptoms
Pervasive pattern of instability of interpersonal relationships, self-image and affects, and marked impulsivity, beginning by early adulthood and present in variety of contexts, indicated by 5+ of the following (polythetic criteria):
Frantic efforts to avoid real or imagined abandonment
A pattern of unstable and intense interpersonal relationships characterised by alternating between extremes of idealisation and devaluation
Identity disturbance: markedly and persistently unstable self-image or sense of self
Impulsivity in 2+ areas that are potentially self-damaging (spending, sex, substance abuse, reckless driving, binge eating).
Recurrent suicidal behaviour, gestures or threats or self-mutilating behaviour
Affective instability due to a marked reactivity of mood (e.g. intense episodic dysphoria, irritability or anxiety usually lasting a few hours, rarely more than a few days)
Chronic feelings of emptiness
Inappropriate, intense anger or difficulty controlling anger (e.g. frequent displays of temper, constant anger, recurrent physical fights)
Transient, stress-related paranoid ideation or severe dissociative symptoms
BPD: neurobiological factors
Regulatory control regions (PFC, ACC)
Emotion response regions (amygdala, hippocampus)
Diminished connectivity between these two.
Repetitive TMS to dlPFC -> short-term improvements in emotion regulation in BPD patients
B: Narcissistic (NPD)
Grandiose view of their qualities, preoccupied with fantasies of great success
Interpersonal relationships affected by lack of empathy, arrogance and envy, entitlement and high expectations of others
View themselves as superior; overestimate attractiveness and contributions
When interacting with others, primary goal is to bolster own self-esteem - value being admired over closeness
Do a lot to gain admiration, pursue fame and wealth
Predicts relationship problems, seek out high-status partners
NPD: symptoms
5+ of following signs of grandiosity, need for admiration and lack of empathy from early adulthood across many contexts:
Grandiose view of one's importance
Preoccupation with fantasies of success, power, brilliance, beauty, ideal love
Belief that one is special and can be understood only by other high-status people
Extreme need for admiration
Strong sense of entitlement
Tendency to exploit others
Lack of empathy
Envious of others
Arrogant behaviour or attitudes
NPD: causes
Parenting: overly indulgent parenting promotes beliefs that child is special and behavioural expressions of specialness are tolerated
People with high levels of narcissism report parental overindulgence
Parental tendencies to perceive their children as highly superior predicted narcissism
But evidence that parental abuse or neglect is closely related to narcissistic personality disorder
Fragile self-esteem: Kohut model of narcissism
Projected on the surface: self-importance, self-importance, self-absorption and fantasies of limitless success
These mask a very fragile self-esteem
Inflated self-worth and denigration of others are defences against feelings of shame
People with NPD experience shame more frequently
Show more reactivity to negative/positive feedback
Social exclusion activates neural regions associated with pain (anterior insula, ACC): more activation in NPD - particularly sensitive to negative social interactions
Fragile self-esteem predicts poorer important outcomes
C: Avoidant
Restrained in social situations, extreme fear of saying something foolish, being embarrassed, showing signs of anxiety
Often co-occurs with social anxiety disorder - genetic vulnerabilities overlap
Symptoms:
Pervasive pattern of social inhibition, feelings of inadequacy, hypersensitivity to criticism, indicated by 4+ of the following from early adulthood across many contexts:
Avoidance of occupational activities that involve significant interpersonal conflict, because of fears of criticism, rejection, disapproval
Unwilling to get involved with people unless certain of being liked
Restrained in intimate relationships due to fear of being shamed/ridiculed
Preoccupation with being criticised/rejected
Inhibited in new interpersonal situations due to feelings of inadequacy
Viewing self as socially inept, unappealing, inferior
Reluctant to take risks or try new activities because they may prove embarrassing
C: Dependent
Excessive need to be taken care of, indicated by 5+ of the following from early adulthood across many contexts:
Difficulty making decisions without excessive advice and reassurance from others
Need for others to take responsibility for most major areas of life
Difficulty disagreeing with others for fear of losing their rapport
Difficulty doing things on own/starting projects because of lack of confidence
Doing unpleasant things to obtain others' approval and support of others
Feelings of helplessness when alone because of exaggerated fears of being unable to care for self
Urgently seeking a new relationship when one ends
Preoccupation with fears of having to take care of self
C: Obsessive-compulsive (OCPD)
Perfectionist, preoccupied with details, rules, schedules, to the point of failing to complete tasks
More oriented towards work than pleasure, social relationships suffer
Reltionships impacted by demands that everything be done the right way - their way.
Unable to discard worn out objects, even with no sentimental value, likely to be frugal
Less interpersonal difficulties than other PDs - not tied to major problems in friendships, family, romantic relationships
Different from OCD: doesn't include obsessions and compulsions
OCPD: symptoms
Intense need for order, perfection and control, indicated by 4+ following from early adulthood across many contexts:
Preoccupation with rules, details and organisation to the extend that the point of the activity is lost
Extreme perfectionism interferes with task completion
Excessive devotion to work to the exclusion of leisure and friendships
Inflexibility about morals and values
Difficulty discarding worthless items
Reluctance to delegate unless others conform to one's standards
Miserliness (adica zgarcenie ca stiu ca intrebi)
Rigidity and stubbornness
Models of PD
Learning/behavioural
Conditioning, modelling, contingencies
Linehan: emotion regulation
Cognitive
Beck: cognitive model
Young: maladaptive schemas
Psychodynamic
Mentalisation
Object-relations
Learning/behavioural models: conditioning
Classical conditioning: "if I attach to a person, I'll get hurt"
Operant conditioning: "if I force my way, I get what I want"
Modelling: witnessing your parents resolve conflict with clashes over and over
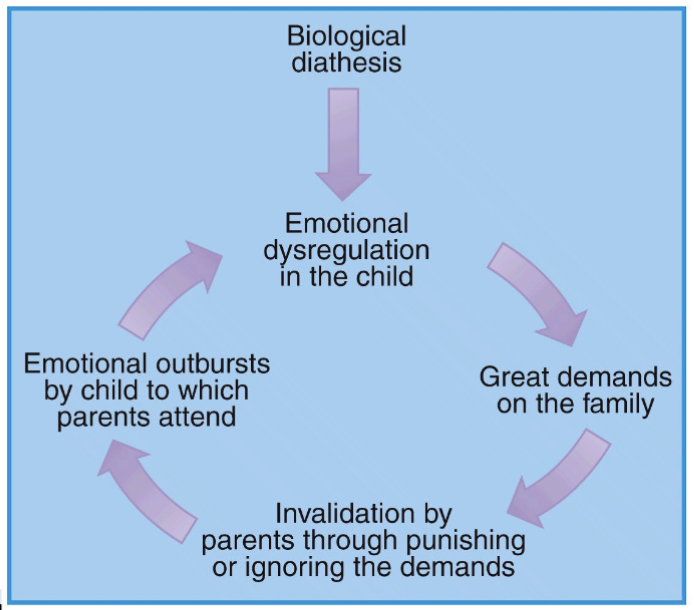
Learning/behavioural models: Linehan’s Emotional Dysregulation model of BPD
Biological vulnerability -> difficulty controlling emotions + invalidating family environment (person's efforts to communicate feelings are disregarded/punished) -> BPD
Emotional dysregulation and invalidation interact with each other.
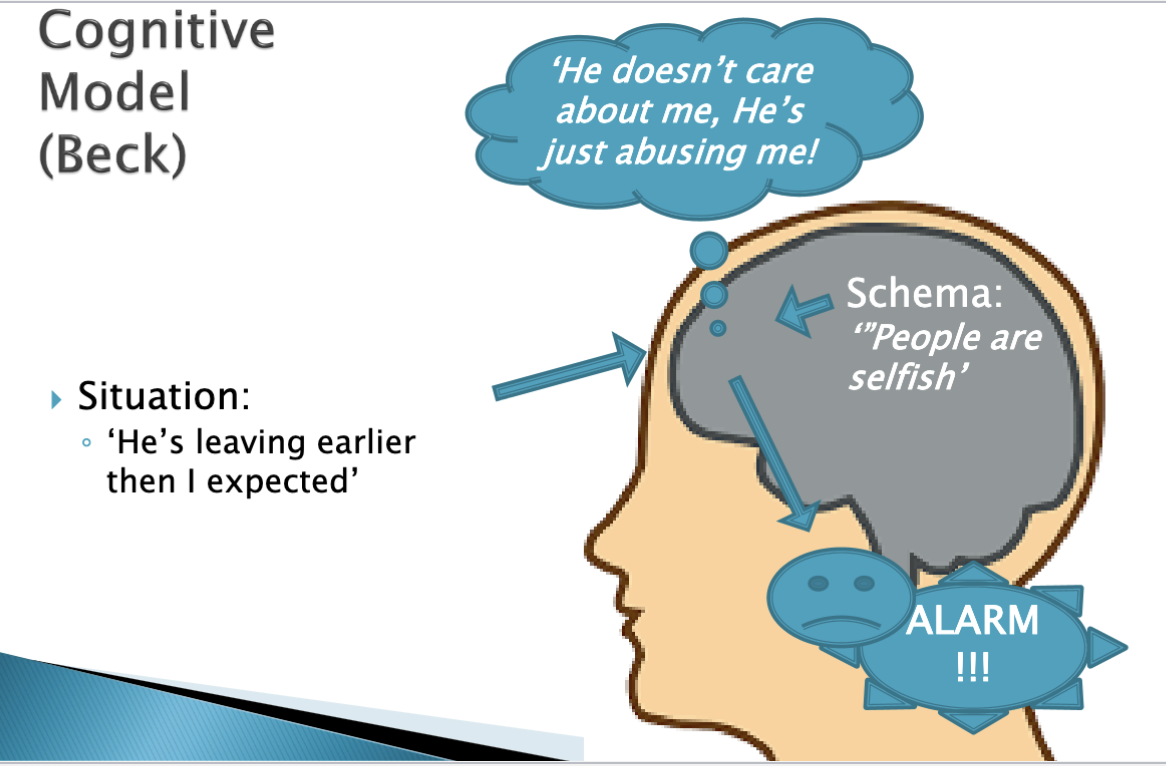
Cognitive models: Beck’s cognitive model
Beliefs about the world (schemas) affect the automatic thoughts that pop into our brain.
Cognitive models: Young’s schema theory
Extension on Beck's cognitive theory
Basic needs (safety, autonomy, boundaries..) not met
-> early maladaptive schemas
Were useful/adaptive in the past
18 or so schemas (e.g. abuse/mistrust, abandonment/instability)
Coping with schemas: submission, avoidance, overcompensation
-> Multiple modes: vulnerable child, angry child, detached protector, demanding parent, healthy adult
Psychodynamic models: Mentalisation
understanding the behaviour of the other (and yourself) in terms of their mental states
Hypothesis: mentalisation is learned as primary caretakers mirror and name the child's emotions
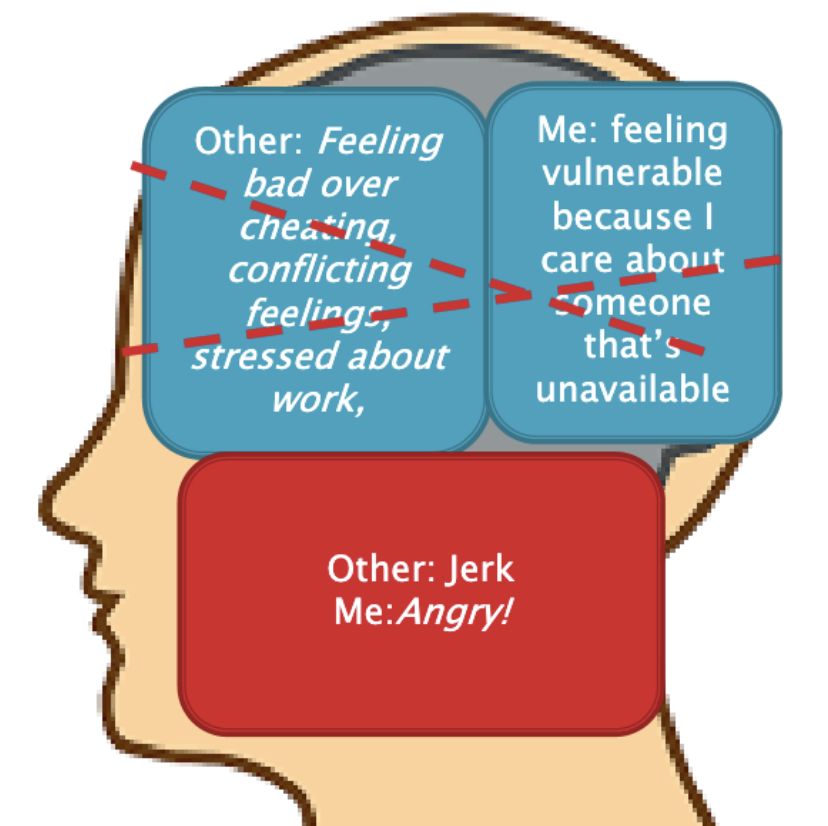
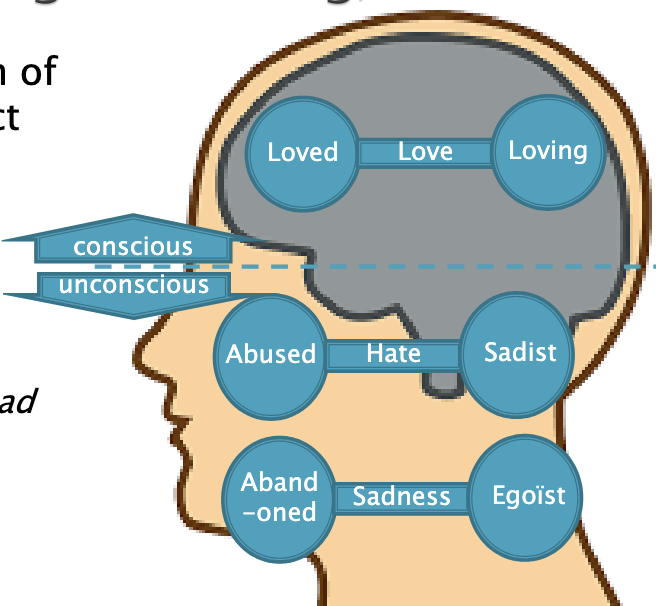
Psychodynamic models: Object-relations
internalised representation of self in relation to the object (another person: father, mother, men etc.)
In PD immature defence mechanism (e.g. splitting - all good/all bad)
Treatment of PDs
Roadblocks:
Life threatening behaviours
Therapy damaging behaviours
Motivation
Requirements:
Safe environment: clear structure, attachment figures
Incentive/invitation to revise coping: clear rationale
Possibility of new (positive) experiences
Is psychotherapy effective for changing personality?
Psychotherapy and other interventions -> significant changes in personality traits (e.g. neuroticism), often within 6 weeks.
e.g. Programs enhancing emotion regulation skills address neuroticism
PDs: medications
Supplement to psychotherapy, treat accompanying depression, anxiety or cognitive symptoms.
Antidepressants - depressive symptoms
Antipsychotic drugs (risperidone, Risperidal) - some symptoms of schizotypal
Treatment: The Big Four
Dialectical Behavioural Therapy (DBT):
Third wave, acceptance and change, skills training (emotion regulation etc.)
Stabilises, works well in auto-mutilation
Schema (focused) therapy (ST):
Integrative: attachment theory, experiential therapy, cognitive therapy. Limited reparenting, imagery rescripting, chair dialogue (doesn't work),…
Wide scope, demanding of capacities
Mentalisation Based Treatment (MBT):
Foster mentalisation: modelling, small steps etc.
Simple, works well for severe cases
Transference Focused Psychotherapy (TPF):
Object-relations: the relationship with the therapist as working material
Higher dropout rate
Intermittent explosive disorder (IED)
Recurrent verbal/physical aggressive outbursts that are far out of proportion to circumstances
Difference from conduct disorder: aggression is impulsive, not preplanned
Oppositional defiant disorder (ODD)
Child doesn't meet criteria for conduct disorder (especially extreme physical aggressiveness) but
Exhibits behaviours like losing temper, arguing with adults, repeatedly refusing to comply with requests from adults, deliberately doing things to annoy others, being angry, spiteful, touchy, vindictive
Prevalence: 8%
Often co-occurs with ADHD, but is different: ODD defiant behaviour doesn’t arise from attentional deficits or impulsiveness.
Children with ODD are more deliberate in their unruly behaviour than children with ADHD
Conduct disorder is 3-4x more likely in boys
Boys are only slightly more likely to have ODD
Conduct disorder
Involves aggressive behaviours, serious rule violations (e.g. truancy), property destruction, deceitfulness
Behaviour marked by callousness, viciousness, lack of remorse
DSM-5 includes a 'limited prosocial emotions' diagnostic specifier for children with callous/unemotional traits (shallow emotions, lack of feelings of remorse, empathy, guilt)
Children with conduct disorder and callous traits had more problems with symptoms, peers and families than children with conduct disorder and no callous traits
Conduct disorder: defining symptoms
Involves a pattern of repeated destructive and harmful behaviour taking different forms, including:
Aggressive behaviour (bullying, physically hurting animals/people)
Destroying property (vandalising a building, setting a fire)
Lying or stealing (shoplifting, breaking into a house and stealing items, lying about behaviour)
Breaking rules (skipping school, missing curfew)
Conduct disorder: comorbidity
Substance abuse (conduct d. either predicts or co-occurs)
Anxiety and depression are common (15–45%)
Social anxiety/specific phobias predict conduct disorder
Conduct disorder: longitudinal course
7% of preschoolers exhibit symptoms of conduct disorder
Conduct disorder symptoms at age 3 predict conduct disorder symptoms at age 6🤯, even accounting for ADHD/ODD -> important to assess early
Moffitt: Two different courses:
Life-course-persistent pattern of antisocial behaviour: conduct problems at 3, serious transgressions into adulthood
Adolescence-limited: typical childhood, antisocial behaviour in adolescence, typical adulthoods
Result of maturity gap between physical maturation and opportunity to assume adult responsibilities/obtain rewards accorded such behaviour
Study: continued troubles with substance use, impulsivity, crime and mental health into mid 20s
In 30s, women had no more difficulties with violent behaviour, men did
Both women and men continued to have issues with substance abuse, physical health and economic issues
Conduct disorder: prevalence
5–6%
3-4x more common in boys than girls
Adolescence-limited type > life-course-persistent type
Conduct disorder: prognosis
Half of boys don't fully meet criteria at later assessment, but continue to have some conduct problems
Conduct disorder: genetic influences
Shared genetic factors with other disorders (ADHD, depression)
Some genetic influences specific to conduct disorder, antisocial behaviour
Twin studies: aggressive behaviour is more heritable than other rule-breaking behaviour
Genetic influence of rule-breaking behaviour depends on wealth of neighbourhood (genetics play more of a role in wealthy neighbourhoods)
Combination of conduct disorder and callous/unemotional traits is more heritable than just conduct disorder
Children of biological mothers exhibiting antisocial behaviour are more likely to have callous/unemotional traits
Unless adoptive mother uses positive reinforcement -> parenting is a buffer for genetic propensity
Lower heritability of callous/unemotional traits in families with more parental warmth
Aggressive/antisocial behaviours beginning in childhood (life-course-persistent) more heritable than behaviours that begin in adolescence
Conduct disorder: neurobiological influences
Deficits in regions supporting emotion, particularly empathetic responses
Children with callous/unemotional traits have difficulty perceiving distress and happiness on others' faces, but no difficulty perceiving anger
Reduced activation in regions associated with emotion and reward: amygdala, ventral striatum and PFC
Children with callous/unemotional traits have difficulty learning to associate behaviour with reward/punishment (dysfunction in amygdala and ventral striatum)
Conduct disorder: psychological influences
Children with conduct disorder (especially with c/u traits) are deficient in moral awareness
Moral awareness = sense of what is right/wrong; ability and desire to abide by rules and norms
Lack of moral awareness in adulthood figures in APD and psychopathy; risk factor
Bidirectional relationship between parenting and c/u traits
Twin receiving harsher parenting more likely to have c/u traits -> may develop in part from environmental factors
c/u traits may contribute to decreases in parental warmth -> c/u traits predict lessening in parental warmth over time
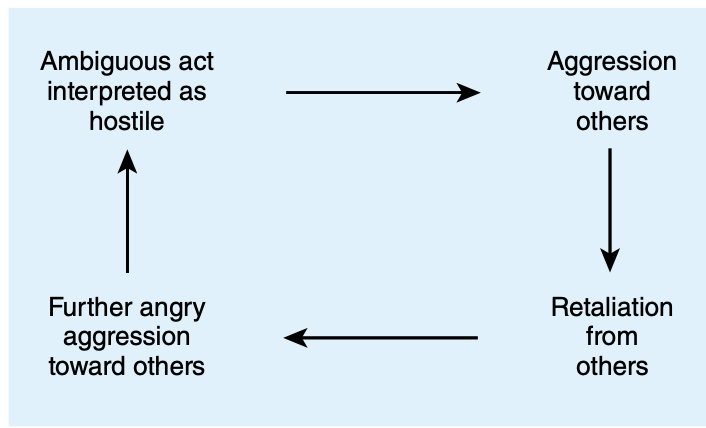
Social-cognitive approach:
Hostile bias: children more likely to interpret ambiguous acts as hostile, leading them to act more aggressively
Conduct disorder: peer influences
Acceptance/rejection by peers
Being rejected by peers -> aggressive behaviour (especially combined with ADHD)
Bidirectional, children prone to react negatively are more rejected by peers -> more likely to engage in antisocial behaviour
Affiliation with delinquent peers
Modelling or coercion.
Children with conduct disorder choose like-minded deviant peers, but also environmental factors lead to choosing deviant peers, which exacerbates conduct disorder
Treatment of conduct disorder
Family interventions:
Family checkup (FCU): prevents conduct problems and aggression in children
Three meetings to assess and provide feedback to parents about children and parenting practices
Associated with less disruptive behaviour even 2y later
Parenting management training (PMT): most effective treatment for conduct disorder and ODD
Parents are taught to modify their responses so that prosocial rather than antisocial behaviour is consistently awarded
Techniques like positive reinforcement and time-out, loss of privileges
Most effective for conduct
Multisystemic treatment (MST):
Delivering intensive and comprehensive therapy services in the community, targetting adolescent, family, school and peer group
Based on view that conduct problems are influenced by multiple factors in family as well as interactions with other social systems
Prevention programs:
Fast Track: reductions in later psychopathology and later delinquent behaviours (in part due to decrease in hostile attribution bias)