Chapter 15: Exercise at Altitude
1/23
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
24 Terms
What happens to barometric pressure and oxygen availability at altitude, and how does this affect the body?
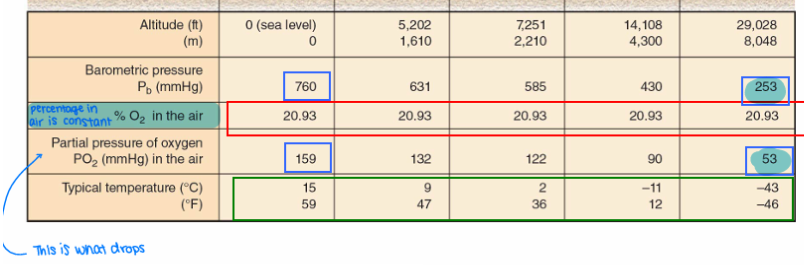
At sea level, barometric pressure (Pb) is about 760 mmHg, and the partial pressure of oxygen (PO₂) is about 159 mmHg (≈21% of Pb).
At altitude, barometric pressure decreases (hypobaria), which lowers the partial pressure of oxygen in the air (hypoxia). This leads to reduced oxygen entering the blood, causing hypoxemia (low blood oxygen).
As a result, oxygen availability for working muscles decreases, which limits exercise performance.
How do air temperature and humidity change at altitude, and what are the physiological consequences?
At altitude, air temperature decreases because air has weight, and there is less atmospheric mass above as elevation increases. Temperature drops by about 1°C per 150 m of ascent, increasing the risk of cold-related disorders.
Humidity also decreases because cold air holds very little water vapor, making high-altitude air both cold and very dry. This leads to increased dehydration, as the body loses water more quickly through both the skin and respiratory system.
How are altitude levels classified, and how do they affect physiological function and exercise performance?
Altitude is categorized based on physiological impact from reduced oxygen availability:
Sea level (<500 m): No physiological effects.
Low altitude (500–2,000 m): Minimal effects on well-being; performance may decline slightly (VO₂ max begins to decrease around 1,500 m) but can often be improved with acclimation.
Moderate altitude (2,000–3,000 m): Noticeable effects in unacclimated individuals; aerobic capacity and performance decrease, and acclimation may or may not fully restore performance.
High altitude (3,000–5,500 m): Can cause acute mountain sickness; significant performance decline that is not fully corrected by acclimation.
Extreme high altitude (>5,500 m): Severe hypoxic stress; survival is difficult and only limited human settlements exist (about 5,200–5,800 m).
For exercise physiology, altitude effects are generally considered meaningful above ~1,500 m, while below this level physiological changes are minimal.
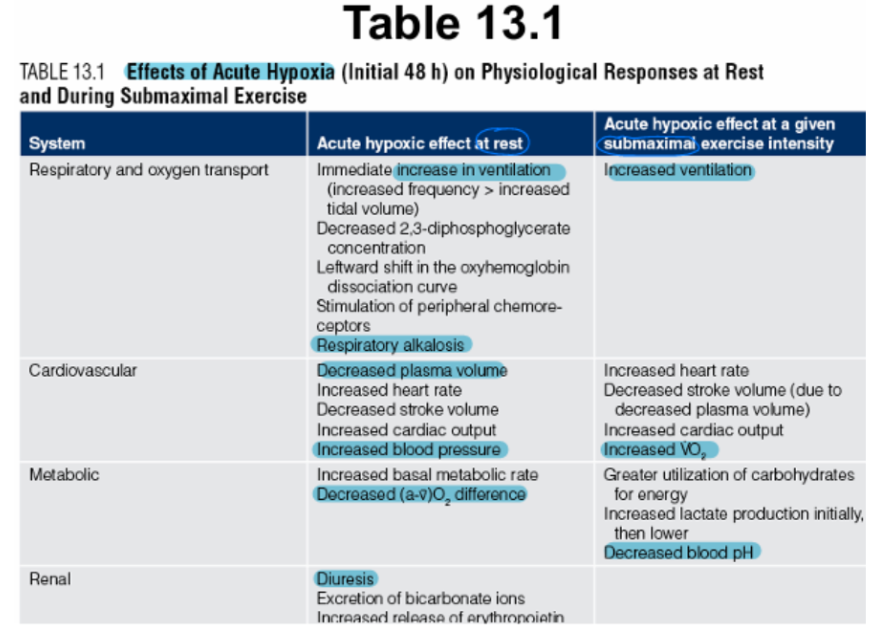
What are the acute respiratory and blood acid–base responses to altitude exposure, and how do they affect oxygen delivery?
At altitude, reduced PO₂ stimulates chemoreceptors in the carotid and aortic bodies, causing an immediate increase in pulmonary ventilation (hyperventilation) at rest and during submaximal exercise. This involves increases in both tidal volume and breathing rate over hours to days.
Hyperventilation lowers alveolar CO₂ (PCO₂), leading to respiratory alkalosis (increased blood pH). This causes a left shift in the oxyhemoglobin dissociation curve, which initially helps oxygen loading but can limit oxygen unloading to tissues.
To compensate, the kidneys excrete bicarbonate (HCO₃⁻), gradually reducing blood pH back toward normal and helping restore acid–base balance, even though overall buffering capacity is reduced.
How does acute altitude exposure affect pulmonary diffusion, oxygen transport, and hemoglobin saturation?
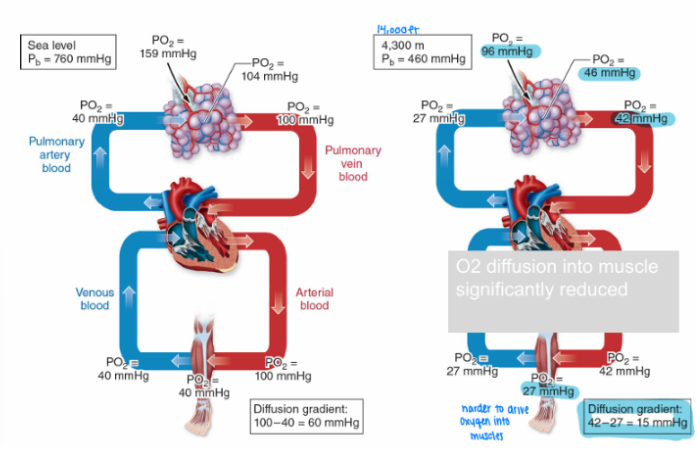
At rest, pulmonary diffusion is not usually a limiting factor for gas exchange at altitude. However, the main issue is reduced alveolar PO₂, which directly lowers oxygen availability in the lungs and leads to hypoxemia.
Because alveolar PO₂ is lower, fewer hemoglobin binding sites are saturated with oxygen, resulting in decreased oxyhemoglobin saturation.
The oxyhemoglobin dissociation curve shifts left, which helps preserve oxygen loading in the lungs and minimize desaturation. This shift partially compensates for reduced oxygen availability but does not fully prevent reduced oxygen transport to tissues.
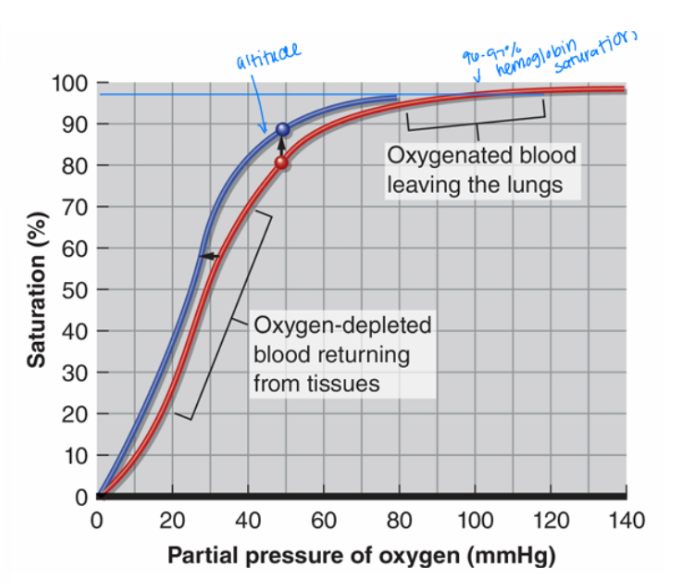
What happens to the hemoglobin curve at high altitude?
The hemoglobin curve shifts left
What are the short-term and longer-term cardiovascular and blood adaptations to acute altitude exposure?
In the short term (within hours), altitude exposure causes a decrease in plasma volume due to respiratory water loss and increased urine production, which can reduce plasma volume by up to ~25%. This leads to a temporary increase in hematocrit and blood oxygen concentration.
Over days to weeks, hypoxemia stimulates erythropoietin (EPO) release from the kidneys, which increases red blood cell production in the bone marrow, raising hematocrit over time.
Cardiovascularly, cardiac output increases at rest and during submaximal exercise despite reduced stroke volume, driven by increased sympathetic nervous system activity (epinephrine and norepinephrine) and a higher heart rate. This is a short-term, less efficient adaptation lasting about 6–10 days.
With continued exposure, muscles adapt by increasing oxygen extraction, which raises the a-vO₂ difference and reduces the need for high cardiac output.
How does acute altitude exposure affect maximal oxygen uptake (VO₂max), and what are the main cardiovascular causes?
Acute altitude exposure reduces VO₂max because of both lower oxygen availability and reduced cardiovascular performance.
At altitude, maximal cardiac output (Q̇max) decreases, driven by:
A decrease in stroke volume (SVmax) due to reduced plasma volume
A decrease in maximal heart rate (HRmax) due to reduced sympathetic nervous system responsiveness
At the same time, the PO₂ gradient is reduced, meaning less oxygen can be delivered from the lungs to the blood and then to working muscles.
Together, lower Q̇max + reduced oxygen availability = decreased VO₂max, significantly limiting oxygen delivery to muscles under hypobaric (low-pressure) conditions.
How does acute altitude exposure affect metabolism, fuel use, and lactate production?
At altitude, basal metabolic rate increases due to higher thyroxine and catecholamine secretion. At the same time, appetite often decreases, making it harder to maintain body mass and energy balance.
Fuel use shifts toward greater reliance on glucose rather than fat, and there is an increase in anaerobic metabolism, leading to higher lactic acid production initially. Over time, lactate production decreases as the body adapts, although the exact mechanism behind this (the “lactate paradox”) is not fully understood.
What are the effects of altitude?
How does altitude affect VO₂max and exercise performance, and what evidence shows the impact at extreme elevation?
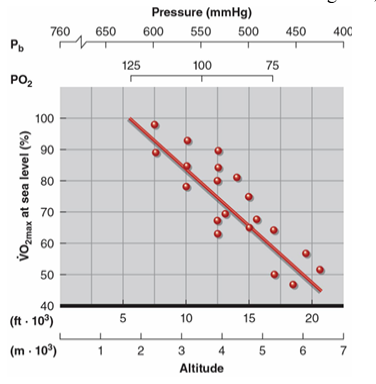
VO₂max decreases as altitude increases above about 1,500 m, when atmospheric PO₂ falls below ~131 mmHg. This decline is mainly due to reduced arterial PO₂ and lower maximal cardiac output (Q̇max).
VO₂max typically drops by about 8–11% per 1,000 m of ascent, significantly limiting aerobic performance.
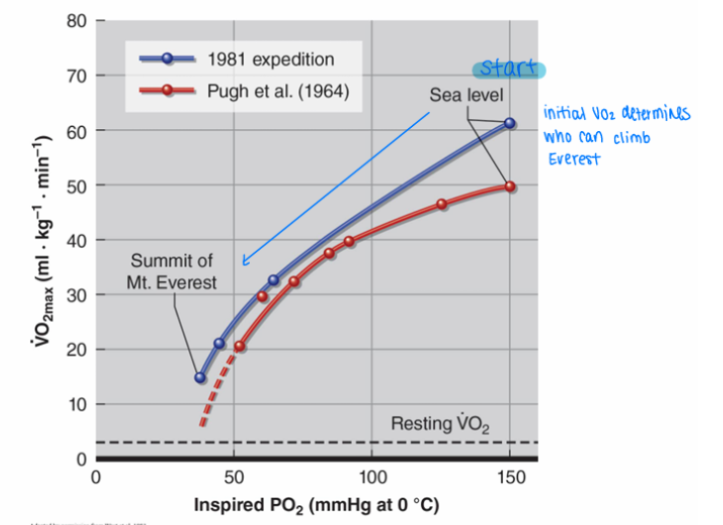
Evidence from a 1981 Mt. Everest expedition study showed VO₂max falling from 62 to 15 ml/kg/min at extreme altitude. Individuals with a sea-level VO₂max below about 50 ml/kg/min would not be able to climb such extreme altitudes without supplemental oxygen.
What effect does the VO2 max and inspired air of a person have on their ability to climb mount everst?
How does altitude affect aerobic exercise performance and perceived effort?
Aerobic exercise performance is most strongly affected by hypoxic conditions at altitude, which reduce VO₂max compared to sea level.
Because the absolute oxygen cost of a given task stays the same, but oxygen availability is reduced, the same workload becomes more difficult.
Individuals with a higher sea-level VO₂max perceive the effort as easier at altitude.
Individuals with a lower sea-level VO₂max experience a higher relative strain, making the same task feel harder.
How does altitude affect anaerobic performance and why can some short-duration events improve?
Anaerobic performance is generally unaffected and can sometimes improve at altitude because these activities rely mainly on the ATP-PCr system and anaerobic glycolysis, which require minimal oxygen.
Events such as 100–400 m sprints, and sometimes up to 800 m, may improve due to reduced air density, which lowers air resistance. This can also enhance jumping events, while effects on throwing events are variable depending on technique and conditions.
What is altitude acclimation, how long does it take, and how does it affect performance?
Altitude acclimation is the physiological adaptation to chronic exposure to high altitude that improves performance under hypoxic conditions. It involves pulmonary, cardiovascular, and skeletal muscle adaptations, but performance often still does not fully return to sea-level capacity.
Acclimation typically takes about 3 weeks at moderate altitude, with an additional ~1 week required for every 600 m increase in elevation.
These adaptations are reversed relatively quickly, with most benefits lost within about 1 month after returning to sea level.
Explain this image.
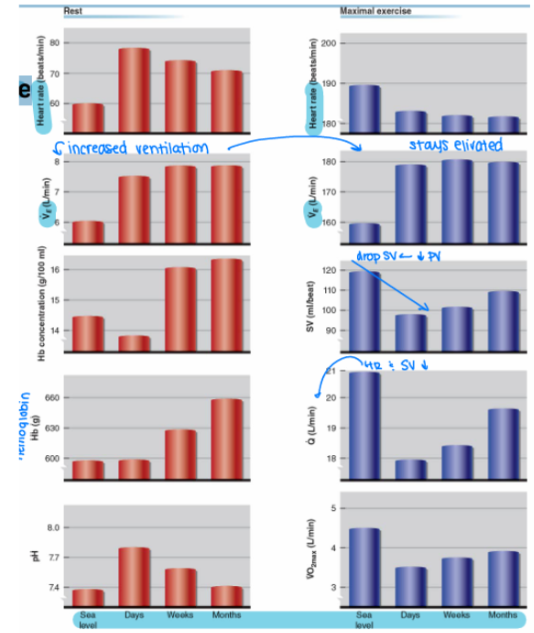
This image shows how the body responds to altitude over time at rest and during maximal exercise.
At rest, the body immediately increases breathing (ventilation) to get more oxygen. Over days to weeks, it gradually increases red blood cells and hemoglobin, improving oxygen-carrying capacity. Blood pH shifts at first but then returns toward normal as the body adjusts.
During maximal exercise, performance is more limited. VO₂max drops and stays reduced, mainly because:
Stroke volume decreases (less blood returning to the heart)
Maximal heart rate is slightly reduced
Even though breathing increases, it cannot fully compensate for low oxygen levels
Bottom line: the body adapts to altitude over time, but endurance performance never fully returns to sea-level levels, especially during maximal effort.
What are the main altitude training strategies and how do they affect performance?
Altitude training aims to use low oxygen conditions to stimulate adaptations (like increased red blood cell mass) that improve oxygen delivery, especially when returning to sea level.
Common strategies include:
Train high, compete low: Athletes live/train at altitude to gain adaptations, then compete at sea level where oxygen availability is higher → often improves performance.
Train high, compete high: Maintains exposure but performance is limited due to hypoxia.
Train low, compete high: No altitude adaptation benefits; performance is impaired at competition altitude.
Live high, train low, compete high: Live at altitude for RBC adaptations but train at lower altitude to maintain high training intensity, then compete at altitude.
What are two strategies for sea-level athletes competing at altitude, and what are their limitations?
Sea-level athletes competing at altitude typically use two approaches:
Compete soon after arrival at altitude: This avoids the worst acute effects of altitude, but does not allow time for acclimation, so athletes also do not gain performance benefits.
Train at altitude for ~2 weeks before competition: This allows partial acclimation and reduces early adverse effects, but aerobic training quality is reduced at altitude, which can limit training effectiveness.
What is the “live high, train low” altitude strategy and why is it most effective for performance improvement?
“Live high, train low” means athletes live at high altitude to gain physiological adaptations (like increased red blood cell production) while training at lower altitude to maintain high training intensity.
This approach allows passive acclimation to hypoxia without reducing workout quality due to low oxygen levels.
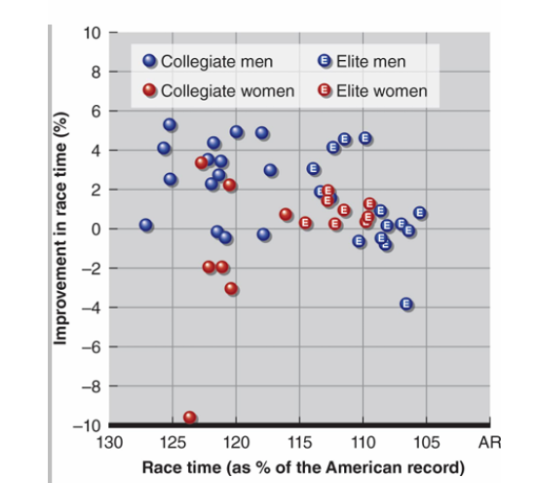
Performance studies (e.g., 5 km time trials) show:
Live high, train low → significant improvement
Live high, train high → little or no improvement
Live low, train low → no improvement
What does research show about the effectiveness of “live high, train low” altitude training?
Recent research supports the “live high, train low” model as an effective altitude training strategy. Athletes live at around 2,500 m to gain physiological adaptations while training at about 1,250 m to maintain training intensity.
When tested at sea level, this approach has been shown to improve performance, including:
About a 1.1% improvement in aerobic performance
About a 3.2% increase in VO₂max
This demonstrates that combining altitude exposure with high-quality training can meaningfully enhance endurance performance
What are the main types of artificial altitude training and how effective are they compared to “live high, train low”?
Artificial altitude training tries to mimic hypoxia at sea level. One method is breathing hypoxic air for 1–2 hours per day while training normally, but this has shown little to no performance improvement.
Another method involves living or sleeping in hypoxic environments (e.g., altitude apartments) to reduce PO₂ while training normally at sea level. This approach is still not fully scientifically validated.
Overall, the most effective and well-supported strategy remains natural “live high, train low”, which is especially beneficial for elite athletes. Non-elite individuals may still gain some benefit from artificial methods, but results are less consistent.
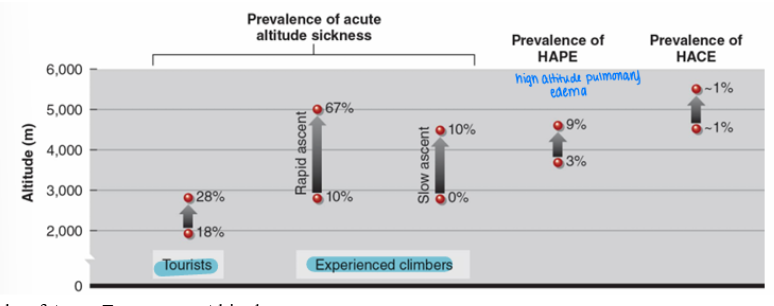
What is acute mountain sickness, when does it occur, and what factors affect its incidence?
Acute mountain sickness (AMS) is a common condition caused by rapid exposure to high altitude. It typically begins 6–48 hours after arrival, with symptoms peaking around days 2–3.
Symptoms include headache, nausea/vomiting, shortness of breath (dyspnea), and insomnia. In severe cases, it can progress into more dangerous altitude-related conditions.
Incidence varies depending on:
Altitude level (higher altitude = greater risk)
Rate of ascent (faster ascent = higher risk)
Individual susceptibility
At 2,500–3,500 m, incidence is about 7–22%, and women tend to have a higher incidence than men.
What causes altitude sickness and its key symptoms, and how are severe cases (HAPE and HACE) prevented and treated?
Altitude sickness is caused by low ventilatory response to altitude, leading to CO₂ accumulation and acidosis, along with hypoxia-induced cerebral vasodilation, which increases pressure and stimulates pain receptors.
The most common symptom is a headache, typically throbbing, continuous, worse in the morning or after exercise, and more common above ~3,600 m. Sleep is also disrupted due to Cheyne-Stokes breathing, which causes cycles of rapid breathing, slow breathing, and apnea.
Prevention and treatment include gradual ascent, acetazolamide (and sometimes steroids), and in severe cases, supplemental oxygen or hyperbaric rescue bags.
Severe altitude illness can progress to life-threatening conditions:
HAPE (high-altitude pulmonary edema)
HACE (high-altitude cerebral edema)
Both involve fluid accumulation (edema) and require immediate treatment.
What are HAPE and HACE, including their causes, symptoms, and treatments?
HAPE (High-Altitude Pulmonary Edema) is caused by hypoxic pulmonary vasoconstriction, which increases pressure in the lungs and can lead to fluid buildup (and possibly clot formation) in the pulmonary circulation. Symptoms include shortness of breath, cough, chest tightness, fatigue, low blood oxygen, cyanosis (bluish skin), confusion, and potentially unconsciousness. Treatment requires supplemental oxygen and immediate descent to lower altitude.
HACE (High-Altitude Cerebral Edema) is a severe complication of altitude illness, often occurring above ~4,300 m, involving increased intracranial pressure and brain swelling. Symptoms include confusion, lethargy, ataxia (loss of coordination), unconsciousness, and death if untreated. Treatment also requires supplemental oxygen, use of a hyperbaric bag if available, and immediate descent to lower altitude.